|
|
Case Reports Indian Pediatrics 2002; 39:485-488 |
||
|
Incomplete Kawasaki Syndrome in an Eighty-Days-Old Male Infant |
||
|
A.M. Vijayalakshmi
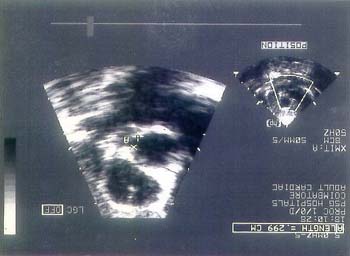
Kawasaki disease (KD) is an acute febrile multisystem vasculitis of young children. This disorder occurs worldwide with Asians being at the highest risk(1). Approximately, 20-25% of untreated KD patients develop coronary artery abnormalities with a potential for myocardial infarction and sudden death. KD has been reported from various parts of India(2-8). Kawasaki disease is rare in infants less than 3 months of age(9). Here we report a case of incomplete Kawasaki disease in an eighty-days-old male infant. This to the best of our knowledge is the youngest case ever reported in Indian literature. Case Report An eighty-days-old male infant presented with fever of 3 days duration. On examination he was febrile, sick looking and extremely irritable. He had erythematous rash over the trunk and extremities. His oral cavity and lips were deeply red and he had erythema of palms and soles. There was no conjunctival injection or cervical lymphadenopathy. The BCG vaccination site over the left arm was deeply erythematous. Cardiovascular system examination revealed heart rate of 140/min and Grade II systolic murmur over the mitral area. Liver was palpable 3 cm below the right costal margin but spleen was not palpable. On day 4 of illness (on admission), the total white blood cell count was 16,000/cumm, differential count – P-55, L-41, E-4 and hemoglobin was 10.3 g/dl. His erythrocyte sedimentation rate was 115 mm in 1st hour and platelet count was 7,02,000/cu mm. The C-reactive protein was positive and urine examination was normal. Cerebrospinal fluid examination showed lymphocytic pleocytosis (15 cells/cumm) but biochemical analysis was normal and culture was sterile. SGPT was normal and blood culture was sterile. X-ray chest and ultrasonogram abdomen were normal. On admission a provisional diagnosis of sepsis/meningitis was made. The child was started on IV ceftriaxone after lumbar puncture. He continued to have irritability, spiking fevers and erythematous rash for one week and diarrhea for 3 days during hospital stay. On 10th day of illness he developed periungual desquamation of all fingers. Three days later he developed desquamation of all toes. Complete hemogram done on 10th day of illness revealed the following features. The total white cell count was increased to 24,400/mm3. The hemoglobin was 9.2 g/dl and ESR was elevated to 135 mm in the 1st hour. The platelet count was 1143000/mm3 Baseline echocardiogram done on 7th day of illness revealed left main coronary artery size of 2 mm. Repeat echocardiogram done after 3 weeks of illness revealed aneurysm involving left main coronary artery with the diameter of 3 mm (Fig.1). As intravenous gamma globulin could not be given due to economic constraints, the child was treated with aspirin only. He was put on low dose aspirin 5 mg/kg at the time of discharge. Discussion Kawasaki disease is almost exclusively an illness of young children with about 80% of patients under the age of 4 years. The male to female ratio is 1.5:1. The etiology of KD remains unclear. An infectious etiology has been suggested; however, extensive studies have not revealed a consistent causative agent(10). The diagnosis of KD is established by the presence of fever of atleast 5 days duration and atleast four of the five principal criteria without other explanation for the illness. The five principal criteria are(11): (i) Bilateral conjunctival injection; (ii) Changes of the mucosa of the oropharynx including injected pharynx, injected or dry fissured lips, strawberry tongue; (iii) Changes of the peripheral extremities such as edema or erythema of hands or feet, desquamation usually beginning periungualy; (iv) Rash primarily trunkal, polymorphous but non vesicular; and (v) Cervical adenopathy. Not all patients with KD fulfil the classic diagnostic criteria. Children with KD manifested by fever and fewer than four of the other features are called "incomplete" or "atypical" KD(9). Incomplete KD is most common in young infants who are at greatest risk of coronary artery disease(12-14) and diagnosis of such cases is difficult. Our case had fever for 10 days and satisfied three of the five other criteria and hence fits into incomplete Kawasaki disease.
Fig. 1. Echocardiogram showing aneurysmal dilatation of left main coronary artery. Associated non cardiac features of Kawasaki disease are extreme irritability, arthritis, aseptic meningitis, diarrhea, hepatic dysfunction and hydrops of gall bladder. Our case had extreme irritability, diarrhea, aseptic meningitis and erythema at the site of BCG inoculation as the associated features. Certain laboratory features are characteristic of KD. Elevated WBC count with predominance of neutrophils is typical in acute phase. Elevated ESR and C-reactive protein are almost universally present in the first week of illness and may persist for 4-6 weeks. Normocytic anemia is common in patients during acute phase and thrombocytosis is classically associated with KD during the 2-3 week of illness(9). Our child had all the above laboratory features typical of KD. Treatment of patients with KD in the first 10 days of illness with 2 grams/kg dose of IV gamma globulin reduces the prevalence of coronary abnormalities from 20% to 2-4%. As young infants with KD frequently lack full diagnostic criteria, high index of suspicion is necessary to establish the diagnosis. Early diagnosis and appropriate treatment is important in young infants as they are at highest risk for coronary artery abnormalities. Acknowledgement We are thankful to Dr. J.S. Bhuvanesh-waran, Cardiologist, P.S.G. Hospital for performing and interpreting the Echocardio-graphic studies. Contributors: AMV reviewed the literature and drafted the paper; she will act as the guarantor for the paper. VG helped in drafting the manuscript. Funding: None. Competing interests: None stated.
| ||
| References | ||
|
![]()