|
|
|
Indian Pediatr 2018;55: 254 -256 |
 |
Peripheral Precocious
Puberty Caused by Human Chorionic Gonadotropin Producing Pineal
Gland Tumor
|
|
SK Hammadur Rahaman 1,
Deepak Khandelwal1,
Rajesh Khadgawat1,
Devasenathipathy Kandasamy2
and Sameer Bakhshi3
From Departments of 1Endocrinology, 2Radiology
and 3Medical Oncology, AIIMS, New Delhi, India.
Correspondence to: Dr SK Hammadur Rahaman, Department of
Endocrinology and Metabolism,
AIIMS, New Delhi 110 029, India.
Email: [email protected]
Received: May 22, 2017;
Initial review: July 03, 2017;
Accepted: December 01, 2017.
|
Background: Pineal gland lesions usually present with central
precocious puberty. Case characteristics: A 3½-yr-old boy
presented with precocious puberty. Clinically and biochemically, it was
gonadotropin releasing hormone (GnRH) independent. Serum and CSF beta-hCG
levels were increased. Thin section magnetic resonance imaging of brain
revealed a pineal gland tumor. Outcome: He received chemotherapy
followed by radiotherapy and responded well. Message: CSF
b-hCG
should be measured in all cases of peripheral precocity, and if CSF
beta-hCG is elevated, thin section magnetic resonance imaging of brain
should be considered.
Keywords: Cerebrospinal fluid
b-hCG,
Diagnosis, Magnetic resonance imaging.
|
|
I
ntracranial germ cell tumors (GCT) are rare
accounting for 0.4-3.4% of all pediatric brain tumors in Western
countries and upto 11% from Japan and other Asian countries [1,2]. Among
all types of GCTs, germinomas are the most common [3]. They are most
commonly located in pineal and suprasellar regions of brain. Human
chorionic gonadotropin (hCG) secreting GCTs in pediatric age group are
extremely rare. Here we describe a case of hCG-secreting pineal tumor
which presented with gonadotropin independent precocious puberty, and
responded well to chemotherapy and radiotherapy.
Case Report
A 3½-yr-old boy was brought with complaints of
progressive penile enlargement, noticed by the mother since the age of
two and half years with change in voice and appearance of pubic hair for
last 6 months. He had accelerated growth and aggressive behavior. The
child did not have headache, vomiting, visual impairment or seizures.
There was no evidence of salt wasting crisis, bony pain, fracture or
deformity. He was born out of non-consanguineous marriage at full term
with an uncomplicated neonatal course. His developmental milestones were
appropriate for age. Family history was non-contributory.
He was alert, hyperactive, normotensive with no
facial asymmetry, bony deformity or hyperpigmentation. Anthropometry
revealed height of 107cm, weight of 22 kg (both >97th centile); mid
parental height (MPH) was 163 cm (5th centile) [4]. Testicular volume
was 6 mL on both sides, with stretched penile length of 8 cm and Tanner
stage 3 pubic hair. There was no hepato-splenomegaly. Fundus examination
did not show any abnormality. Rest of the general and systemic
examinations were within normal limits.
Investigations revealed normal hemogram, kidney and
liver function tests. Bone age was 5.5 years (advanced by two years,
according to Greulich and Pyle’s atlas). He had normal thyroid function,
elevated serum total testosterone (5.09 ng/mL) and suppressed
gonadotropins (Leuteinizing hormone [LH] 0.21 mIU/mL; Follicle
stimulating hormone [FSH] 0.66 mIU/mL) which did not increase after
Gonadotropin releasing hormone (GnRH) agonist stimulation test. A
diagnosis of peripheral precocity was made. On further evaluation, serum
17 hydroxy-progesterone (1.37 ng/mL; normal value 0.1-1.39 ng/mL) and
dehydro epiandrosterone sulphate (DHEAS) levels (27.8 mcg/dL; normal
value <27 mcg/dL) were within normal range for age. However, serum beta-hCG
level (31.49 mIU/mL; normal value <5.0 mIU/mL) was increased which was
confirmed by three repeated estimations. Hence, a possibility of
peripheral precocity caused by beta-hCG producing lesion was considered.
Ultrasound scrotum and contrast enhanced computed
tomography (CECT) chest and abdomen were normal. Magnetic resonance (MR)
of sella and brain revealed a subtle abnormality in pineal gland without
any definite lesion. 18FDG
PET/CT scan and 68Ga-DOTANOC
PET/CT scan did not show any abnormal uptake. In view of non-localisation
of the source of hCG, cerebrospinal fluid (CSF) analysis was performed
which revealed a high CSF beta-hCG level (49.21 mIU/mL, normal value
<5.0). Notably, alpha fetoprotein was normal both in the peripheral
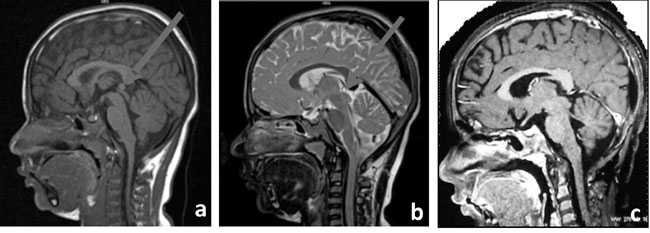
blood and CSF. To characterise the lesion of pineal gland, thin section
MR brain showed a 8.0 x 6.0 x 5.0 mm cystic pineal lesion with blood
fluid level within (Fig. 1 a and b).
 |
|
Fig. 1 Thin section MR brain in
sagittal section T1 weighted (a) and T2 weighted (b) image
showing 8.0 × 6.0 × 5.0 mm pineal gland with necrosis (white
dot) within. MR Brain (c) after 4 cycles of chemotherapy
revealed disappearance of pineal tumor.
|
A diagnosis of peripheral precocious puberty caused
by beta-hCG secreting pineal tumor was made. He was treated with four
cycles of bleomycin, etoposide and cisplatin (BEP) chemotherapy with
dramatic response. There was regression of secondary sexual characters.
Serum testosterone level and beta-hCG levels both in serum as well as
CSF normalised (Table I). Repeat MR sella revealed
disappearance of pineal lesion (Fig. 1c). Thereafter he
received radiotherapy to the brain. At 12 months of follow up, he was
tumor-free and clinically well.
TABLE I Baseline Hormonal Parameters and Tumor Markers in Index Patient
|
At presentation |
After chemotherapy |
Age appropriate |
|
|
2 cycles |
4 cycles |
normal value |
|
Serum total testosterone (ng/mL) |
5.09
|
1.2
|
0.29 |
0.02-0.25 |
|
Serum β-hCG (mIU/mL) |
31.49
|
5.09 |
<1.2 |
<5.0 |
|
CSF β-hCG (mIU/mL) |
49.21
|
9.27 |
2.45 |
<5.0 |
Discussion
Precocious puberty caused by pineal GCT may be
gonadotropin-dependent, causing interference with gonadostat or may be
gonadotropin-independent caused by secretion of hCG, which acts
biologically like LH. In our case, pineal lesion produced hCG causing
peripheral precocity, as evidenced by high hCG level in CSF and serum
and negative gonadotropin releasing hormone stimulation test. Ectopic
hCG secreting tumors are known to cause precocity in boys and
occasionally peripheral precocity in girls [5,6]. The postulated
mechanisms of precocity in females are: low FSH activity of very high
hCG and high aromatase activity of pineal tumor.
The role of tissue biopsy to confirm pineal area
tumors and its surgical management remains contro-versial as the tumors
are heterogeneous and the procedure may result in severe complications.
Our case responded well with four cycles of cisplatin, etoposide and
bleomycin followed by radiotherapy. There are reports of hCG-secreting
pineal germ cell tumors which respond well to radiotherapy [7,8] or both
radiotherapy and chemotherapy [5,6,9]. Kuo, et al. [10]
successfully treated a 9-year-old boy with pineal GCT and peripheral
precocious puberty without any surgical intervention.
In this case, we first diagnosed peripheral precocity
secondary to an hCG secreting tumor. CSF hCG levels were elevated which
indicated central nervous system as the likely tumor site, but initially
imaging of brain could not localize any lesion. So, it was a challenge
to localize the source of hCG as nuclear imaging like
68Gallium DOTANOC PET/CT and
18FDG PET/CT were normal. Finally,
it was the thin section MRI that picked up the lesion.
Present case report suggests measurement of CSF beta-hCG
in all cases of peripheral precocious puberty, and if CSF beta-hCG is
elevated thin section MR brain is advisable. It also highlights the
complete clinical, biochemical and radiological resolution of the tumor
with nonsurgical management.
Contributors: SHR, DK: wrote the manuscript; RK,
DK, SB: edited the manuscript.
Funding: None; Competing interests: None
stated.
References
1. Jennings MT, Gelman R, Hochberg F. Intracranial
germ-cell tumors: Natural history and pathogenesis. J
Neurosurg.1985;63:155-67.
2. Hoffman HJ, Otsubo H, Hendrick EB, Humphreys RP,
Drake JM, Becker LE, et al. Intracranial germ-cell tumors in
children. J Neurosurg. 1991;74:545-51.
3. Matsutani M, Sano K, Takakura K, Fujimaki T,
Nakamura O, Funata N, et al. Primary intracranial germ cell
tumors: a clinic analysis of 153 histologically verified cases. J
Neurosurg. 1997;86:446-55.
4. Agarwal DK, Agarwal KN, Upadhyay SK, Mittal R,
Prakash R, Rai S. Physical and sexual growth pattern of affluent Indian
children from 6-18 years of age. Indian Pediatr. 1992;29:1203-82.
5. O’Marcaigh AS, Ledger GA, Roche PC, Parisi JE,
Zimmerman D. Aromatase expression in human germinomas with possible
biological effects. J Clin Endocrinol Metab. 1995;80:3763-6.
6. Starzyk J, Starzyk B, Bartnik-Mikuta A, Urbanowicz
W, Dziatkowiak H. Gonadotropin releasing hormone- independent precocious
puberty in a 5 year-old girl with suprasellar germ cell tumor secreting
ß-hCG and a- fetoprotein. J Pediatr Endocrinol Metab. 2001;14:789-96.
7. Ahmed SR, Shalet SM, Price DA, Pearson D. Human
chorionic gonadotrophin secreting pineal germinoma and precocious
puberty. Arch Dis Child. 1983;58:743-5.
8. Takahashi H, Tokuda N, Kariya H. Precocious
puberty in a seven-year-old boy due to human chorionic gonadotropin
producing pineal tumor detected by nuclear magnetic resonance computed
tomographic scanning. Acta Paediatr Jpn. 1990;32:88-93.
9. Chan HSL, Humphreys RP, Hendrick EB, Chuang SH,
Fitz CR, Becker LE. Primary intracranial chorio-carcinoma: A report of
two cases and a review of the literature. Neurosurgery. 1984;15:540-5.
10. Kuo HC, Sheen JM, Wu KS, Wei HH, Hsiao CC.
Precocious puberty due to human chorionic gonadotropin-secreting pineal
tumor. Chang Gung Med J. 2006; 29: 198-202.
|
|
|
 |
|
