|
|
Case Reports Indian Pediatrics 2006; 43:252-254 |
||||
|
Safe and Painless Manipulation of Penile Zipper Entrapment |
||||
|
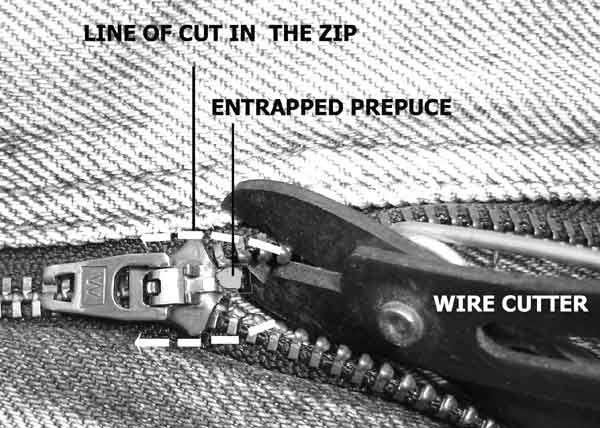
Abstract: Key words: Children, Injury, Penis, Zipper. Entrapment of penile foreskin is quite a distressing situation for the child and the parents and can be a frustrating management problem. Any overzealous intervention would simply worsen the situation. Also, attempts to cut open the zip fastener are time taking and may not be either helpful or feasible in all the situations. The approach to the zipper manipulation should be quick, simple, non-traumatic and reproducible irrespective of the age of the child, mechanism and site of entrapment, presence of the local edema and zipper size or design. Case Report The technique described was applied in three consecutive boys of 5-7 years. All of them had entrapment of the prepuce while fastening the zip. In two of them, the ventral prepuce was entrapped whereas the third boy had entrapped the dorsal skin of his shaft. In each of these, the prepuce was entrapped between the zip and the zip fastener. In the first case, parents had tried some lubricant in vain. In the second case, the parents had cut the pant off the zip and further, in an attempt to extricate the prepuce, had cut the lower (zipped) end of the zip and peeled apart the two halves. But the zip fastener, still holding the prepuce, did not budge from its place. In the third case a local doctor had tried unfastening the zip after infiltration of 2% lignocain in the prepuce, but failed to release the prepuce and rather caused further ecchymosis. All these boys were very frightened at presentation. Technique In all these cases only one method was applied. Step 1: Just ahead of the entrapped foreskin, using an ordinary wire cutter, the two unzipped halves were first given transverse cuts over the free margin so that the tooth line is divided, and then, further cutting the cloth strips just lateral to the tooth lines, the cuts were extended along the sides of the zip fastener (Fig. 1).
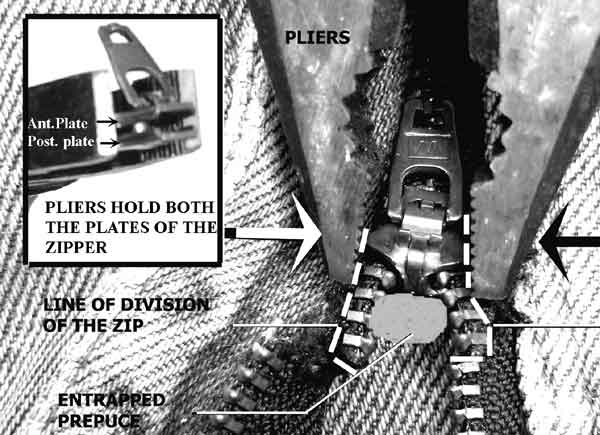
Step 2: The zip fastener was then held with pliers from side to side ensuring that the lateral margins of its both anterior and posterior faceplates were within the grip of the pliers (Fig. 2). Applying a strong compression, the entrapped foreskin was released instant-aneously. This maneuver was painless. It was due to an increased gap between the two faceplates of the zip fastener when compression was applied from the lateral sides. The increased gap resulted in loosening the interdigitation of the teeth of the two halves of the zip, allowing the prepuce to be slipped off.
The first step is essential to facilitate a proper grip of the pliers over the sides of the two faceplates together (Fig. 2 inset). Unless the cloth strips are cut upto the sides of the zip fastener, the posterior plate, which is behind the zip line, cannot be properly held, as the pliers are applied from the anterior surface of the zipper. If there is no enough width of the cloth strip between the central teeth line and the stitching of the zip to the pant, the cut in the zip should be extended upto the sides of the zip fastener by cutting through the pant fabric. No local anesthesia is required. The children can simply be taken into confidence. Small babies, if required, may be sedated. Discussion Entrapment of unprotected penis into zipper is the most common cause of prepuceal injury in children(1). These children are often distressed and frightened due to several unsuccessful and painful attempts at extrication by the parents(2). In these cases, various management strategies are reported, including an aggressive approach of partial excision of the entrapped foreskin, or a circumcision under general anesthesia(3). The non aggressive management strategies involve some form of mechanical disengagement of the zipper from the skin. One of the crude methods is to push the zip fastener in the opposite direction from which it had originally trapped the skin(4) However, tugging at the zipper in either directions may result in a tighter entrapment or a further bruising as it tends to re-enact the original trauma in the reverse. Another technique described is to unfasten the zipper one tooth at a time, alternating sides(1-4). Also reported is giving transverse cuts through the cloth strips holding the tooth line, and allowing disengagement from both sides of the entrapment(5). Still others report use of mineral oil followed by traction(2). However, the most common method described so far, involves the division of the median bar connecting the anterior and posterior faceplates of the zip fastener, using a bone cutter or a mini hacksaw(6-9). These strategies of zip manipulation, while effective, are not very rapid and cause sufficient movement of the zipper and the penis and therefore, often require local anesthesia. Moreover, if the median bar lies deep or a portion of the entrapped prepuce projects ahead of the zip fastener, it may be very difficult and potentially dangerous to divide the median bar using these methods. The technique reported here is simple, safe, quick, and painless. As it does not involve a division of the median bar, it can be used in all the cases of prepuceal entrapment regardless of the size of the zip, the mechanism of entrapment, the position or projection of the prepuce, and an associated edema. Funding: None. Competing interests: None.
| ||||
|
References | ||||
|
![]()