|
|
Case Reports Indian Pediatrics 2006;43:535-538 |
||||
|
Treatment of Acute Infectious Purpura Fulminans with Activated Protein C |
||||
|
M.R. Lokeshwar
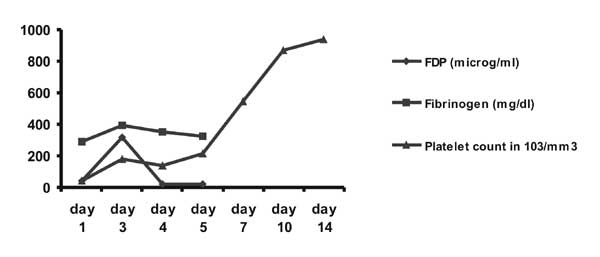
Purpura Fulminans (PF) is an acute syndrome characterized by rapidly progressive skin necrosis and disseminated intravascular coagulation (DIC). Infectious PF is most commonly associated with meningococal sepsis followed by pneumococcal sepsis, measles and neonatal group B streptococcal infections(1). Since acute infectious PF is associated with a 50% mortality and significant morbidity despite antimicrobials, novel therapies have been evaluated(1-3). We report our experience with APC (drotrecogin alpha activated) use in two children with infectious PF. Case Reports Case 1 A 5-month previously healthy male presented with fever (102ºF) of one day duration. Physical examination was normal except for fever and subtle bluish ecchymotic patches over knees. Shortly after admission, he developed cold clammy extremities, poor peripheral pulses and a generalized petechial rash. Fluid resuscitation and intravenous ceftriaxone were initiated promptly with restoration of satisfactory circulatory status. Complete blood count showed neutrophilic leucocytosis (TLC 22,600, 86% poly-morphs) with fragmented cells and poly-chromatic macrocytes. DIC profile was deranged (Fig. 1). There was severe metabolic acidosis, elevated BUN, low serum calcium/ albumin and mildly elevated liver enzymes. The blood culture grew Streptococcus pneumoniae, sensitive to penicillin G. CSF was normal.
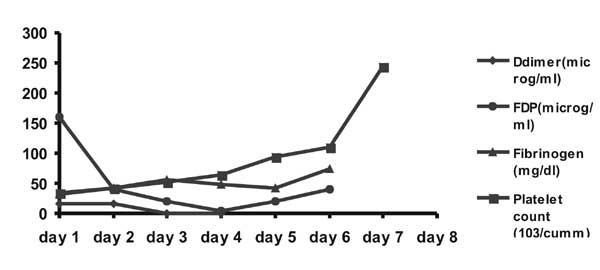
The clinical and metabolic abnormalities resolved over 24-36 hours. But then, the ecchymotic lesions over the knees became darker and the terminal digits of hands and feet became gangrenous suggestive of PF. The DIC profile worsened (Fig. 1). Protein C activity was 29% of normal. After obtaining informed consent, APC therapy was initiated at 24 µg/kg/hour for 96 hours. No fresh lesions appeared and FDP’s declined (Fig. 1). Mild prolongation of APTT occurred but there was no clinical bleeding. Two weeks later only sequelae was dry gangrene of the terminal digits of the hands. Protein C and S activity three months after recovery was normal. Case 2 A 15-month-old previously healthy male presented with two day’s fever and vomiting. At admission, there was marked irritability, pallor, cold extremities, tachycardia, normal rectal temperatures and normal blood pressure. He had blackish necrotic indurated lesions on the cheek, trunk and the limbs. The WBC count was 11,900/cumm with 70% neutrophils and 8% band forms. There was elevated BUN, metabolic acidosis, hypoproteinemia and hypoalbuminemia, hypocalcemia, and elevated liver enzymes. The DIC profile was abnormal (Fig. 2). CSF showed 1280 RBC, 1680 WBC (83% polymorphs), protein of 307 mg/dL and sugar of 37 mg/dL, gram-negative cocci on gram stain and meningococci on latex agglutination. CSF and blood cultures were sterile. Protein C and Protein S activity was 24% and 55% of normal.
In view of severe meningococcal sepsis with PF, fluid resuscitation and intravenous ceftriaxone was started immediately. APC therapy was initiated after parental consent. There was a progressive improvement in peripheral perfusion with resolution of lesions. The DIC parameters improved (Fig. 2). Following discontinuation of APC infusion there was a decline in fibrinogen levels with rise in FDP but with no adverse clinical consequences. The child was normal at discharge. Discussion We demonstrated a satisfactory clinical outcome in two children with acute infectious PF with use of APC. There were no obvious adverse effects. The cost of APC was Rs. 1,00,000 in case 1 and Rs 1,60,000 in case 2. However, in the absence of a control group we cannot attribute the satisfactory clinical outcome in both the index cases only to APC. Adjunct therapies evaluated in infectious PF include Protein C, APC, antithrombin III, FFP, plasma exchange, tissue plasminogen activator, heparin, dextran, topical nitro-glycerin, prostacyclin, hirudin and even regional nerve blocks(1). The experience with most except Protein C is anecdotal. Protein C is critical in regulation of microvascular coagulation. Protein C is converted to APC when thrombin complexes with thrombomodulin (an endothelial cell glycoprotein) in the presence of the endothelial Protein C receptor(4). APC with Protein S limits generation of thrombin by inactivating Factor Va and VIIIa and promotes fibrinolysis. Most importantly, APC by virtue of inhibiting leucocyte cytokine release/ expression of leucocyte adhesion molecules and limiting thrombin production exhibits potent anti-inflammatory activity(4). In sepsis there is depletion of Protein C (degree of depletion inversely correlates with the outcome) as well as decreased conversion of Protein C to APC(5,6) Thus the rationale for using Protein C/APC in severe sepsis. The link between sepsis and activation of the coagulation cascade is most prominent in patients presenting with infectious PF(3). In four uncontrolled studies involving 53 patients with meningococcal PF treated with protein C, mortality was 10% (predicted mortality 30-50%) and amputation rate was 15% (expected amputation rate 33%)(3). No adverse effects attributable to protein C were observed. Since these studies were non-randomized, improvements over historical controls could have been due to better supportive care and other therapies. APC should be theoretically superior to Protein C in management of sepsis/ PF as there is impaired conversion of protein C to APC in severe sepsis(7). In a multicentric placebo controlled randomized trial in adults with severe sepsis (PROWESS), initiating APC therapy within 48 hours of onset of organ dysfunction resulted in 6.1% absolute and 19.4% relative reduction in 28-day mortality(8). The risk of bleeding was marginally more in the APC group. An open label non-randomized study on 83 children with severe sepsis demonstrated that the safety, pharmacokinetics and pharmaco-dynamics of APC were similar to adult patients(9). A phase 3 randomized efficacy study is currently underway in pediatric sepsis. Experience with APC use in infectious PF is limited(10). However, since presence of PF in sepsis classifies sepsis as severe and since some patients in the PROWESS study did have PF (though not analyzed separately), the results of the PROWESS study can be extrapolated to infectious PF. It can also be hypothesized that APC may improve the outcome of sepsis associated PF significantly more than the garden variety of severe sepsis due to the pivotal role of APC in infectious PF. There is definitely a need for adjunct therapy in acute infectious PF in children. Lack of level 1 evidence on efficacy of Protein C/APC in childhood sepsis, risk of serious bleeding and high cost of therapy are factors that need to be addressed before APC becomes the standard of care for childhood infectious PF. Contributors: All authors were involved in case-management, review of literature and drafting of manuscript. Funding: None. Competing interests: None.
| ||||
|
References | ||||
|
![]()