|
Piyush Gupta, Geetinder Kaur, Bhawna Sharma, Dheeraj
Shah and *Panna Choudhury
From Departments of Pediatrics, University College of
Medical Sciences, Delhi 110 095; and *Maulana Azad Medical College, New
Delhi 110 002, India.
Correspondence to: Dr. Piyush Gupta, Block R-6-A,
Dilshad Garden, Near Telephone Exchange, New Delhi 110 095, India.
E-mail: drpiyush@satyam.net.in
Abstract
Objectives: To identify the characteristics of
the manuscripts submitted to the Indian Pediatrics; attributes of the
peer-review process and decision-making; and factors associated with
their acceptance or rejection. Methods: All submissions to Indian
Pediatrics during 2002 were analyzed by a retrospective review of
records. Manuscripts were categorized by their place of origin (Indian
vs. foreign), geographic region of India (north, south, east, west,
central), submitting institution (teaching vs. non-teaching), subject
(general pediatrics, systemic pediatrics, neonatology, genetic syndrome,
allied sub-specialities, etc.), and type of article (research paper,
case report, images, letter to editor, review, etc.). Manuscript details
were recorded in a database that also included information on peer
reviewer assignment, editorial and reviewer comments, and final
disposition of the manuscript. Characteristics of accepted and rejected
manuscripts were compared. Results: Indian Pediatrics received
687 manuscripts for consideration in the year 2002; mostly from Indian
authors (89%). Maximum contributions were received from North India
(236, 39%) followed by 165 (27%) from South, 95 (16%) from West, 90
(15%) from Central and 26 (4%) from Eastern part of India. Of 687
papers, 457 (66%) articles qualified for peer review. Agreement between
the reviewers was not significantly greater than that expected by
chance; kappa for inter-rater agreement was 0.35, 0.17 and 0.21 between
any two sets of reviewers for 431, 228 and 203 articles, respectively (P
<0.005). Of 687 submitted manuscripts, 294(43%) were accepted, 347(50%)
were rejected and no decision was possible on 46(7%) manuscripts. The
top reasons for rejection were 'absence of a message', 'lack of
originality', 'inadequate methods', 'not relevant to journal',
'over-interpretation of results', 'unsatisfactory writing style',
'inaccurate/inconsistent/insufficient data', and 'inappropriate
statistical analysis', in that order. Median number of days (IQR) needed
to reach the final decision was 81 (25-210) d; ranging from 8 (3-29.5) d
for Images to180 (90-341) d for Research papers. No preference for
acceptance was noted for foreign articles, geographic region of India,
type of institution, or a particular topic, on both univariate and
multivariate analysis. Conclusion: Indian Pediatrics is receiving
contributions from all over India. Majority of the manuscripts are
peer-reviewed. Of every 10 articles submitted, almost 4 are accepted.
Median time interval from submission to final decision is less than 3
months. The decision-making is not influenced by the place of origin of
manuscript.
Key words: Acceptance, Indian Pediatrics, Journal, Peer-review
Indian Pediatrics, the official scientific
publication of Indian Academy of Pediatrics (IAP) is one of the leading
peer-reviewed biomedical journals of Asia. The journal is being
regularly published on monthly basis since 1964 and is indexed by
National Library of Medicine (NLM) in PubMed and Medline. With 16,000
hard copies per month and free full-text availability online (6000 web
hits per day), the journal has the potential of making a difference to
the health of children in South Asia by influencing clinical practice
and policy. From Vol. 42, 2005, Indian Pediatrics has been selected for
coverage in Current Contents/Clinical Medicine and the Science Citation
Index Expanded (SCIE); the impact factor of the journal will be known in
2008(1).
Over the years, the journal has tried to adapt it to
suit the needs of readers and researchers alike by inviting their
comments and holding regular meetings within its editorial board and
with the office-bearers of IAP. However, at times, concerns have been
raised regarding issues such as narrow author base (articles published
mainly from few selected institutions of North India), foreign author
bias, validity and consistency of peer-review process, delay in
decision-making and biased rejections.
The present study was conducted to evaluate the
characteristics of manuscripts submitted to Indian Pediatrics;
functioning of peer review and decision-making process; and factors
determining acceptance or rejection of these submissions. This
investigation attempts to generate the relevant information; and make it
available to the readers and authors; for the sake of transparency and
sustained interest in the journal publication process.
Methods
An article submitted to Indian Pediatrics
undergoes a strictly uniform editorial process; the major steps being
reception, selection for peer-review, the peer review, review by the
editorial board, final decision, and publication, if accepted.
Reception: The article on its receipt in the
office is immediately assigned a manuscript number, if the format
broadly adheres to ‘Author Information’; otherwise it is returned
immediately without assigning an identification number. All numbered
manuscripts are then referred to the Editor-in-chief.
Initial decision: Articles, not in accordance
with the mission and vision of Indian Pediatrics, and not of interest to
its target readership, are straightaway rejected. Articles submitted for
‘Editorials’, ‘Book reviews’ and ‘Images’ sections are referred to the
editorial board for final decision. All other categories of articles
considered relevant for the journal are subjected to a blinded
peer-review.
Peer-review: A manuscript is sent to at least two
peer-reviewers, in a double blind manner. Identity of the authors is
masked before sending the article to the reviewer; similarly, reviewers’
identity is also not known to the author. Additional reviewers are
sought for articles with multispeciality interest, policy implications,
and those from the members of the editorial board. Opinion of a
biostatistician is sought on articles with lot of statistics. Reviewers
are given 4-6 weeks time to respond. A reminder is sent if there is no
response. Additional reviewers are commissioned, if there is no response
even after another 2 weeks. Once the reviewers’ comments and
recommendations are received, they are analysed by the editor(s),
leading them to the decision of whether to accept it in the current
version, return it to the authors with a request to prepare a new
modified version, or a definitive rejection. Authors are given 12 weeks
to resubmit their revised manuscript. This revised paper is again sent
to the original reviewers of this paper for reappraisal.
Decision-making: The process of modification by
the authors, reappraisal by the original reviewers, and editors’
analysis continues till the manuscript is either deemed fit for
publication, or rejection. The final acceptance letter is, however
issued only after the manuscript clears the technical and language
editing by one of the editors. Manuscripts also have to clear the
Ethical Board of Indian Pediatrics.
Role of editorial board: The Editor-in-chief and
the editorial team decides the overall policy and content of the
journal, ensures that it adheres to a strict publication schedule
(journal is posted on 17-18th of each month), keep authors informed
about their articles, select peer-reviewers and initiate the review
process, commission articles for editorials etc., supervise the
distribution and dispatch of the journal, and manage the day to day
administration of journal office. They are assisted by 3 clerical staff
for maintaining records, accounts, and website; and 2 peons.
Data collection and analysis
For the purpose of this analysis, all manuscript
files created between January 1 and December 31, 2002 were retrieved and
the details were entered in a database. Information was collected for
each manuscript pertaining to its place of origin (country, state); type
of submitting institution (whether teaching/research or non-teaching),
date of submission; category of submission (original article, brief
report, review, case report, letter, images, editorial, etc.);
and topic of the paper (general pediatrics; systemic pediatrics;
neonatology; genetic syndrome; allied sub-specialities including
pediatric surgery, ophthalmology, ENT, radiology, psychiatry,
dermatology; and all others). The initial decision of the editor on
submitting manuscript was recorded. A note was made on whether the
manuscript was reviewed and decided by the editorial board or was
selected for peer-review. For manuscript going for peer-review, number
of allotted reviewers was noted. Additional reviewers, if required later
were also added to this number. Recommendation of each of the reviewers
was categorized as ‘accept’, ‘resubmit with revision' and ‘reject’. For
a particular manuscript, comments of all reviewers were tabulated
separately. Number of revisions required by each manuscript was also
noted. Finally, the editors’ decision on the manuscript was recorded;
reasons for rejection were listed (based on reviewers and editors
assessment); and the date of decision was noted. Time taken from
submission to final decision was calculated for each manuscript.
Acceptance rate (defined as number of articles
accepted to number submitted) was compared between Indian and foreign
manuscripts; different regions of India (North [Chandigarh, Delhi,
Haryana, Jammu and Kashmir, Punjab, Rajasthan, Uttaranchal], South [Andamans,
Andhra Pradesh, Kerala, Karnataka, Pondicherry, Tamil Nadu], East
[Bihar, West Bengal, Orissa, Jharkhand, Assam, North Eastern States],
West [Goa, Gujarat, Maharashtra], and Central [Uttar Pradesh, Madhya
Pradesh, Chattisgarh]); teaching and non-teaching institutions (all
institutions running an undergraduate/postgraduate course or involved in
research were included as teaching); category of articles (Original
articles and Brief reports were considered together as Research papers);
and topic of the submitted paper.
Statistical analysis: Descriptive data is
presented as mean (SD), median (inter quartile range [IQR]), numbers and
frequencies. Quantitative variables were compared by ‘t test’ or
‘analysis of variance’; and categorical variables by ‘Chi square’ or
Fisher’s exact test. Inter-reviewer agreement was evaluated by kappa
statistic. Logistic regression analysis was employed to assess whether
the fate of manuscript (accepted vs. rest) is affected by the
country affiliation of the author, type and geographical region of
submitting institution, category of article, and topic of the submitted
paper. P<0.05 was considered as significant.
Results
Place of origin
A total number of 687 manuscripts were received in
the year 2002. Of these, 612 (89%) were from India and 75 (11%) from 17
other countries. Manuscripts were received from Turkey (n = 32),
Iran (n = 11), UK and Brazil (5 each), Oman and Australia (4
each), USA, Canada and Bangladesh (2 each) and 1 each from Russia,
Pakistan, Greece, Nigeria, Kuwait, Switzerland, Nepal and Germany.
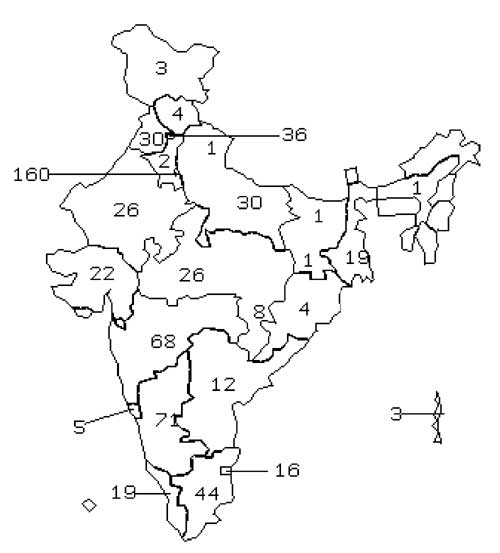
State-wise distribution of manuscripts received from different Indian
states is shown in Fig. 1. Of these, 236 (39%) submissions were
from Northern India; followed by 165 (27%) from South, 95 (16%) from
West, 90 (15%) from Central and 26 (4%) from Eastern part of India.
Two-thirds (66%) of the manuscripts were received from teaching
institutions. As expected, majority (80%) of all research papers
originated from teaching institutions. Submissions for ‘Images’ section,
however, predominated the manuscripts from non-teaching institutions
(27%) as compared to 13% from teaching institutions (P<0.05). For all
other categories, proportion of manuscripts was comparable between
teaching and non-teaching institutions.
 |
|
Fig. 1. Number of manuscripts submitted from various Indian States
during the year 2002
|
Category of submissions
Research articles (both original articles and brief
reports) accounted for maximum sub-missions (n = 214, 31%),
followed by Case Reports (n = 191, 28%), Letters to Editor (n
= 119, 17%), Images (n = 93, 14%), and Reviews (n = 41,
6%). Remaining manuscripts (n = 29) included editorials,
technical guidelines, viewpoints, and book reviews.
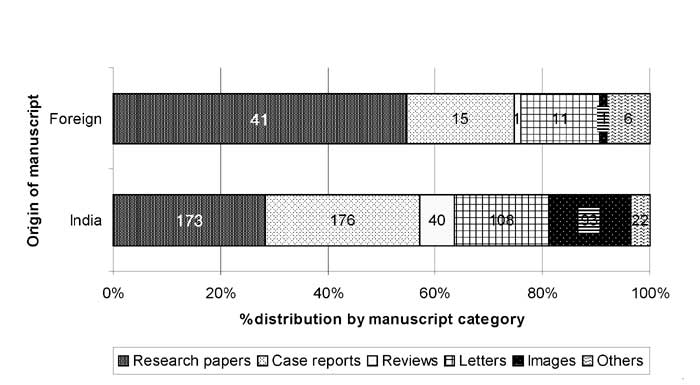
Figure 2 shows the distribution of manuscript
category to place of origin. Most (55%) contributions from foreign
authors were in the form of research articles, as compared to 28% by
Indian authors (P <0.01). Almost all manuscripts for the Reviews and
Images sections were contributed by authors from India. Editorials were
commissioned/ contributed mainly by foreign authors.
 |
|
Fig. 2. Distribution of manuscript category to place of origin
|
Table I shows that all regions submitted
comparable proportion of research papers out of total submissions. Case
reports constituted the maximum proportion of manuscripts submitted from
West India, as compared to other regions (P<0.05). Proportion of
contributions to Images and Letter sections were maximum from Southern
and Central Indian states, respectively.
TABLE I
Category-wise Distribution of Submissions from Various Geographical Regions of India
Submission
category |
All regions
(n = 612) |
North
(n = 236) |
East
(n = 26) |
West
(n = 95) |
South
(n = 165) |
Central
(n = 90) |
|
Research paper |
173 (28.3) |
72 (30.5) |
9 (34.6) |
26 (27.4) |
40 (24.2) |
26 (28.9) |
|
Case Report |
176 (28.7) |
74 (31.4) |
7 (26.9) |
38 (40.0) |
41 (24.8) |
16 (17.8) |
|
Review |
40 (6.5) |
19 (8.1) |
3 (11.5) |
6 (6.3) |
7 (4.2) |
5 (5.6) |
|
Letter to Editor |
108 (17.6) |
34 (14.4) |
4 (15.4) |
15 (15.8) |
26 (15.8) |
29 (32.2) |
|
Images |
93 (15.2) |
24 (10.2) |
3 (11.5) |
9 (9.5) |
46 (27.9) |
11 (12.2) |
|
Others |
22 (3.6) |
13 (5.5) |
0 (0.0) |
1 (1.0) |
5 (3.0) |
3 (3.3) |
Figures in parentheses indicate percentages.
Subject of manuscript
Articles were received from all spheres of
Pediatrics; maximum contributions related to systemic pediatrics (n
= 185, 27%), followed by those from General Pediatrics (n = 126,
18%). Neonatology articles constituted 9% of total submissions (n
= 63). Another major group was that of Genetic syndromes (n = 97,
14%). Manuscripts were also received from allied subspecialties (n
= 86, 12%); remaining papers were of miscellaneous nature (n =
130, 19%). Subject wise distribution of category of submissions is
depicted in Table II.
TABLE II
Subjectwise Distribution of Category of Submissions
Subject
|
All Manu-
scripts
(n = 687) |
Research
paper
(n = 214) |
Case
report
(n = 191) |
Review
(n = 41) |
Letter to
Editor
(n = 119) |
Images
(n = 93) |
Others
(n = 29) |
|
Systemic Pediatrics |
185
(26.9) |
64
(29.9) |
70
(36.6) |
13
(31.7) |
24
(20.2) |
8
(8.6) |
6 (20.7) |
|
Neonatology |
63 (9.2) |
32
(15.0) |
10
(5.2) |
4
(9.8) |
10
(8.4) |
4
(4.3) |
3 (10.3) |
|
Genetic syndromes |
97
(14.1) |
13
(6.1) |
34
(17.8) |
2
(4.9) |
2
(1.7) |
46
(49.5) |
0 |
|
General Pediatrics |
126
(18.3) |
43
(20.1) |
29
(15.2) |
4
(9.8) |
39
(32.8) |
8 (8.6) |
3 (10.3) |
|
Subspecialties |
86
(12.6) |
12
(5.6) |
36
(18.8) |
2
(4.9) |
9
(7.6) |
24 (25.8) |
3 (10.3) |
|
Miscellaneous |
130
(18.9) |
50
(23.4) |
12
(6.3) |
16
(39.0) |
35
(29.4) |
3 (3.2) |
14 (48.3) |
Figures in parentheses indicate percentages.
Initial Decision
Of 687 manuscripts submitted to Indian Pediatrics,
immediate in-house decision by the editorial board was taken for 230
(34%) articles; 88 (13%) were straightaway accepted, while 142 (21%)
were issued a letter of rejection. letters to editor (n = 73),
Images (n = 91), solicited reviews (n = 9), book reviews
and editorials (n = 17) accounted for 83% of all in-house
decisions. Only 15 research papers and 25 case-reports were turned down
without initiating peer-review process; these were either not relevant
to the target readership, had an overall improper format, or poorly
presented.
Peer review
Peer review process was initiated for 457 (65.9%)
articles. More than 90% of research papers, 86.6% of Case-reports, and
82.4% of Reviews were sent for peer review. Only 38% of Letters and 3%
of Images required peer-review.
Of all manuscripts sent for peer-review, 203 (45%)
were sent to 3 or more reviewers, 228 (50%) to 2 reviewers and remaining
26 to a single reviewer.
Agreement between the reviewers as to whether
manuscripts should be accepted, revised or rejected was not
significantly greater than that expected by chance. Kappa for
inter-rater agreement was 0.35, 0.17 and 0.21 between any two sets of
reviewers for 431, 228 and 203 articles, respectively (P <0.005).
Overall, the discrepancy between the reviewers was more than 50%.
However, the editors were more likely to publish papers when both
reviewers recommended acceptance than when they disagreed or recommended
rejection. Additionally, there was poor agreement between the reviewers
in deciding the priority of publication.
Editorial decision after peer-review
Initial reviews were available for 457 manuscripts.
Based on these comments and evaluation by at least one editorial board
member, 173 papers were rejected, 268 were sent back to authors for
revision, and 16 were accepted. Decision on maximum manuscripts (n
= 116, 43%) could be arrived at after a single revision. Two revisions
were required by 79 papers (29%); another 58 manuscripts (22%)
necessitated 3 revisions; 11 (4%) manuscripts were revised 4 times; two
manuscripts were revised 5 times; and 6 and 7 revisions were required
for 1 manuscript each. Of those sent for revision, 190 (71%) were
accepted and 32 (12%) were rejected. No final decision could be taken on
46 manuscripts (17%) because of non-response by the authors despite
repeated reminders, withdrawal by the authors, or ethical reasons; these
files were closed.
Final decision
Of 687 submitted manuscripts, 294(43%) were accepted,
347 (50%) were rejected and no decision was possible on 46 (7%)
manuscripts. The top ten reasons for rejection are summarized in
Table III.
Table III
Top Ten Reasons for Rejection of Manuscripts in Indian Pediatrics
|
Reason for rejection |
Percentage |
|
1. Absence of a message |
54.5 |
|
2. Poor originality |
43.5 |
|
3. Poor methodology |
28.2 |
|
4. Not relevant to journal |
25.4 |
|
5. Over-interpretation of results |
25.4 |
|
6. Inappropriate writing style/grammar |
24.2 |
|
7. Inaccurate/inconsistent data |
17.0 |
|
8. Poor statistical analysis |
9.8 |
|
9. Insufficient data |
8.0 |
|
10. Unsatisfactory illustrations/tables |
5.2 |
More than one reason might be operating for a given manuscript.
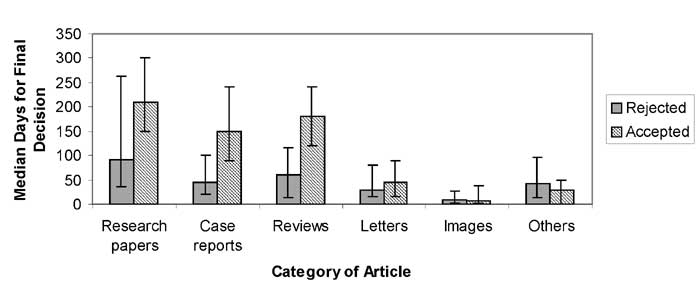
Median number of days (IQR) needed to reach the final
decision was 81 (25-210) d. The waiting period was maximum for Original
articles and Brief Reports [180 (90-341) d] and minimum for Images [8
(3-29.5) d]. Median days (IQR) to final decision for Case Reports,
Reviews and Letters was 100 (40-210), 106 (42.5-210), and 36 (19.5-90)
days, respectively. Figure 3 shows that for all categories of
article (except Images and commissioned articles), it took much lesser
time to reject than to accept them.
 |
|
Fig.3. Time taken [median (IQR)] for Final Decision on Accepted vs
Rejected Articles
|
Factors affecting acceptance
Acceptance rate of Indian and foreign submissions was
43% and 42%, respectively (P = 0.55). The acceptance rate was
similar (43%) for manuscripts from teaching and non-teaching
institutions.
Acceptance rate of articles from North India
(118/235, 50%) was not statistically different from that of Western
(44/95, 46%), and Southern (66/165, 40%) regions of the country (all
P >0.05). Lower acceptance rate was observed for manuscripts from
Eastern (8/26, 31%) and Central (26/90, 29%) India.
Acceptance rate was comparable for Research papers
(85/214, 40%), Case reports (74/191, 39%), Reviews (15/41, 37%) and
Images (33/93, 36%). Acceptance rate was higher for Letters to the
editor (66/119, 56%) and commissioned articles (21/29, 72%).
Papers from allied sub-specialties had the highest
acceptance rate of 63% (54/86), as compared to papers from systemic
pediatrics (42%), neonatology (44%), and general pediatrics (34%).
Lowest acceptance rate (29%) was documented for manuscripts concerned
with genetic syndromes.
On multivariate logistic regression, the only factor
having a significant association with higher acceptance rate was the
paper being a Letter to the Editor or commissioned article. No
preference for acceptance was noted for foreign articles, region of
India, type of institution (teaching or else), or a particular topic.
Discussion
We conducted a retrospective analysis on submissions,
peer review process, and the acceptance of articles submitted during the
year 2002. The analysis year was chosen as 2002 because of the spillage
of manuscripts submitted during the calendar year over subsequent 2
years leading to final decision regarding all manuscripts submitted only
by the end of 2004. At the time of start of this study, this was the
most recent year for which decisions on all manuscripts had been taken.
There is no reason that analysis of "Indian Pediatrics 2002
submissions" is not generalizable to other recent years as there has not
been any major change in the constitution of editorial board or reviewer
database since then. The number of submissions has however gone up from
687 (2002) to 805 (2004). Number of submissions to Indian Pediatrics is
higher than that for Indian Journal of Medical Research
[manuscripts received (year): 2002 (307), 2003 (375), 2004 (405), and
2005 (490)] (personal communication) even though Indian Journal of
Medical Research (IJMR) is a general medical journal. Journal of
Postgraduate Medicine, published quarterly from Mumbai received 770
manuscripts for review in 2005(2). These are much lower than submission
rates to major general, medical journals such as BMJ (6000-7000 per
annum)(3). Similar data were not available for Indian Journal of
Pediatrics, the only other indexed pediatric journal from India.
Journals are often accused of publishing more
material from its place of publication. It is expected that the journals
get more articles from and near the area where it is based. What is to
be seen whether the proximity of the place to the journal has any
influence on the acceptance rate. In the present study, the maximum
contributions were from Northern India (area in proximity to ‘Delhi’ the
journal base) followed by Southern and Western India. Factors that could
have influenced the higher submissions from Northern region include
comparatively higher population of subjects, researchers, doctors, and
tertiary care teaching hospitals/institutes in this geographic area
including All India Institute of Medical Sciences (AIIMS), Delhi and
Post Graduate Institute of Medical Education and Research (PGIMER),
Chandigarh. However, we did not observe any regional preference in the
acceptance rate of manuscripts from different regions of India. This
highlights the journal’s policy of unbiased peer-review and
decision-making.
It is a good sign that Indian Pediatrics
received maximum contributions in form of research articles. This is
expected if teaching institutions contribute more to the journal.
Research and publication is an integral part of duties/responsibilities
of postgraduate students, residents and faculty. It was heartening to
note that practitioners and those from non-teaching institutions are
also contributing equally to other sections of Indian Pediatrics;
especially to the Images section.
Peer-review is supposed to improve the credibility
and quality of a paper(4,5). This is despite the fact reported by most
journals that inter-rater agreement between reviewers generally ranges
from fair to poor(6-8). Present study confirms this fact with respect to
Indian Pediatrics. Another drawback of peer-review is that most
articles rejected in peer-review by one journal are able to clear the
peer-review process and get published in another journal!(9,10). Yet
another issue is whether peer-review should be masked or not? A survey
conducted in 1988 revealed that only 16 of the 86 journals examined were
following blinding the reviewers(11). A randomized controlled trial(12)
has indicated that "masking reviewers to author identity does not
improve the quality of reviews". There is no study to suggest for or
against the utility of blinded peer review in Indian settings. Most of
reviewers and authors of articles submitted to Indian Pediatrics
are from India. It is also being felt lately that despite masking,
re-viewers sometimes are probably able to guess the authors’ identity.
This is expected, as the researcher database in India is limited to few
institutes only. There is a need to conduct a detailed analysis of
various aspects of peer review at Indian Pediatrics to answer all
these issues.
The top ten reasons for rejection of articles in
Indian Pediatrics are similar to that reported earlier(13); originality,
carrying of a message and sound study design are usually enough for the
editor to consider the paper(14). To have an ultimate favorable
decision, it is up to the author to sense the mood of the editor and
revise it accordingly. The acceptance rate of 42% at Indian Pediatrics
is much higher than IJMR, which reports an acceptance rate of only 19%
in 2004 and 27% in 2005 (personal communication). However, Indian
Pediatrics has also noted a downward trend in the acceptance rate in
most recent years (approximately 30% in 2004 and 2005; personal
communication). Due to increase in the number of submission of articles,
Journal of Postgraduate Medicine also reported a declining
acceptance rate which was approximately 20% in the year 2005(2).
Acceptance rate for Indian Journal of Pediatrics was not
available. The declining acceptance rate of manuscripts over the years
(42 % to 30%) by Indian Pediatrics indicate stricter peer-review
process and compares favorably with western journals including The
Lancet and BMJ (10-12%)(4). It is well known that the rejection rate
also tends to rise with increasing number of submissions; mainly due to
relative shortage of print space in the journal. This increases the
chances of acceptance of a crisp and concise manuscript(15).
Data are not available to compare the submission to
acceptance period of Indian Pediatrics with other biomedical
journals in India. However, there is a general feeling that the
disposition of articles is definitely faster at Indian Pediatrics.
Journal of Postgraduate Medicine, Mumbai has claimed to be having a
mean submission to acceptance period of just 69 days(2); however, no
breakup is available according to the category of the article and
whether this included rejected papers also.
Medical journals are the main sources of
dissemination of new knowledge, changes in practices and policies and
research ideas related to life sciences. What gets published in a
journal has long-term and widespread implications. However, often the
journals are accused of a biased approach in publication preferring
reputed/influential authors, authors from a particular region or
institute and biased peer-review process. The editor of the journal is
often perceived as a "demon", whose sole purpose is to find faults with
the articles and finding one or other ground for rejecting the
article(16). It is therefore pertinent that the journals themselves do a
regular self-appraisal and present the results to the concerned readers
to maintain transparency. It is also important to appraise the
researchers and authors of the factors associated with acceptance or
rejection of the articles so that the quality of submissions could be
improved, and publication time decreased. We hope that the present
article serves as a humble beginning.
Contributors: PG conceived the idea of this study
and provided the study design. Data were collected and tabulated by GK
and BS. PG, DS and PC analyzed and interpreted the results. PG and DS
drafted the manuscript, with intellectual inputs from all others. All
authors approved the final manuscript.
Funding: None.
Competing interests: PG and PC are Associate
editor and Editor-in-Chief of Indian Pediatrics, respectively. DS is
member of the editorial board. They work for Indian Pediatrics in an
honorary capacity and do not stand to gain financially by increase in
its authorship/readership.
|
Key Messages |
|
• Research articles
contribute maximally to manuscripts submitted for
consideration of publication to Indian Pediatrics.
• Lack of message and originality, poor
methodology, over-interpretation of results are the major
reasons for rejection of articles.
• Acceptance rate of manuscripts from
different regions of the country are comparable indicating no
regional preference and highlights unbiased peer-review and
decision-making policy of ‘Indian Pediatrics’.
• Increasing number of manuscript submission
with declining acceptance rate over the years indicate stricter
peer-review process and compares favorably with reputed indexed
journals.
|
|
