|
|
Original Article Indian Pediatrics 2003; 40:510-517 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Resuscitation of Asphyxiated Newborns with Room Air or 100%Oxygen at Birth: A Multicentric Clinical Trial |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
S. Ramji*, R. Rasaily**, P.K. Mishra+, A. Narang++, S.
Jayam+++, A.N. Kapoor**, From the *Department of Pediatrics, Maulana Azad Medical College, New Delhi, **Division of Reproductive Health & Nutrition, ICMR, New Delhi, +K.G. Medical College, Lucknow, ++Department of Pediatrics, P.G.I. Chandigarh, +++Department of Pediatrics, KG Hospital Chennai, Correspondence to: N.C. Saxena, Chief, Division of Reproductive Health and Nutrition, Indian Council of Medical Research, Ansari Nagar, New Delhi 110 029, India. Manuscript received: June 18, 2002, Initial review
completed: July 23, 2002, To compare the short-term efficacy of room air versus 100% oxygen for resuscitation of asphyxic newborns at birth. Design: Multicentric quasi randomized controlled trial. Setting: Teaching hospitals. Inclusion criteria: Asphyxiated babies weighing> 1000 grams, with heart rate <100/min and/or apnea, unresponsive to nasopharyngeal suction and tactile stimuli and having no lethal abnormalities. Intervention: Asphyxiated neonates born on odd dates were given oxygen and those on even dates room air for resuscitation. Outcome measures: Primary: Apgar score at 5 minutes; Secondary: Mortality and Hypoxic ischaemic encephalopathy (HIE) during first 7 days of life. Results: A total of 431 asphyxiated babies, 210 in the room air and 221 in 100% oxygen group were enrolled for the study. Both the groups were comparable for maternal, intrapartum and neonatal characteristics. The heart rates in room air and 100% oxygen groups were comparable at 1 minute (94 bpm and 88 bpm), 5 minutes (131 bpm and 131 bpm) and 10 minutes (135 bpm and 136 bpm). Median apgar scores at 5 min [7 versus 7] and 10 minutes [8 versus 8 ], in the room air and oxygen groups respectively, were found to be comparable. Median time to first breath (1.5 versus 1.5 minutes) was similar in the room air and oxygen group. Median time to first cry (2.0 versus 3.0 minutes) and median duration of resuscitation (2.0 versus 3minutes) were significantly shorter in the room air group. The number of babies with HIE during first seven days of life in the two treatment groups (35.7% babies in room air and 37.1% in the 100% oxygen group) were similar. There was also no statistically significant difference in the overall and asphyxia related mortality in the two treatment groups (12.4% and 10.0% in room air versus 18.1% and 13.6% in oxygen group). Conclusion: Room air appears as good as 100% oxygen for resuscitation of asphyxic newborn babies at birth. Key words: Asphyxia neonatorum, Hypoxic ischemic encephalopathy (HIE), Mortality, Oxygen, Resuscitation. BIRTH asphyxia is one of the major causes of early neonatal mortality in India. Report of the National neonatal perinatal database on intramural births from 16 centers indicate that amongst institutional births the incidence of birth asphyxia is around 5% and it accounts for 24.3% of neonatal deaths(1). Apart from high mortality, birth asphyxia is also an important cause of neuromotor disability. It has been estimated that 5 million asphyxiated babies are born worldwide every year. Approximately one million of these babies die and an equal number of babies develop neurodevelopmental sequaele such as cerebral palsy, mental retardation and epilepsy(2). Effective resuscitation at birth can reduce the mortality and sequelae of birth asphyxia. Standard guidelines for resuscitation of asphyxiated newborn recommend use of 100% oxygen for assisted ventilation(3). Recent evidence suggests that resuscitation with high concentration of oxygen lead to excess release of free oxygen radicals during the posthypoxic reoxygenation phase. This has the potential to cause cellular and organ damage(4-6). These observations initiated several experimental studies to investigate the efficacy of room air in neonatal resuscitation. Experimental studies in piglets have indicated that outcome of resuscitation with room air is comparable to the outcome of resuscitation with 100% oxygen(7-10). Preliminary studies comparing room air with 100% oxygen for resuscitation of the asphyxiated newborn have indicated that room air is as effective as 100% oxygen(11-12). The present study was carried out to test the hypothesis that room air is as effective as 100% oxygen for resuscitation of asphyxic newborns at birth. Subjects and Methods This was a multicentric quasi randomized trial, carried out at four centers in India between 1995 and 1997 at Maulana Azad Medical College, New Delhi; Kasturba Gandhi Hospital, Chennai; Postgraduate Institute of Medical Education and Research, Chandigarh and King George’s Medical College, Lucknow. Newborn babies weighing more than 1000 grams having heart beat less than 100/minute and/or apnoeic, unresponsive to nasopharyn-geal suction and tactile stimuli who required assisted ventilation were included for the study. Newborn babies having lethal anomalies, hydrops fetalis and congenital pulmonary or cyanotic heart defects were excluded from the study. Primary outcome measure was Apgar score at 5 minutes. Secondary outcome measures were neonatal mortality and Hypoxic-ischemic encephalo-pathy during first seven days of life. To detect a difference of 1 with a standard deviation of 2 in the apgar score at 5 minutes with a 5% error probability and power of 95%, it was estimated that each group would require 144 patients. It was decided to recruit a total of 300 subjects. The asphyxic babies were resusci-tated with room air when born on even dates and 100% oxygen when born on odd dates to avoid practical difficulties in using random slips which may have caused a delay in institution of emergency therapy. The treatment allocation was not blinded for practical reasons. The neonates were ventilated with an infant resuscitation bag with a ventilatory frequency of 40-60 breaths per minute. The resuscitation bag had a facility to attach an oxygen reservoir to deliver 100% oxygen. Newborns in the 100% oxygen group were resuscitated by connecting the bag to oxygen reservoir with oxygen flow at 4 liters /minutes. Neonates in the room air group who remained bradycardic (heart rate <100/min) and/or cyanosed after 90 seconds of resuscitation (treatment failures) were switched to be resuscitated with 100% oxygen supplementa-tion. In order to know how many infants had treatment failure in the 100% group, similar data was also recorded in that group. At each center the personnel involved in the study were recruited by the investigator who also ensured their training and compliance to the treatment protocol during the study period. In all neonates baseline maternal variables (parity, labour induction, fetal distress, mode of delivery, duration of labour) were recorded. At each center two trained personnel were available at the time of birth of an asphyxiated baby. One of the personnel monitored the time and outcome measures. Each baby was assessed at every 30 seconds till 90 seconds, at 3 minutes, 5 minutes, 10 minutes. Heart rate and colour of babies were recorded at 1, 1.5, 5 and 10 minutes. Apgar scores were noted at 1, 5 and 10 minutes. All babies were assessed for treatment failure at 90 seconds (defined as presence of cyanosis and or heart rate <100/ minute). The time of appearance of first spontaneous breath, first cry and duration of assisted ventilation were noted. The babies were further monitored for presence of HIE as described by Sarnat and Sarant(13) and for neonatal survival. Each participating center obtained approval from their own institute’s ethical committee. Informed consent was obtained from parents for participating in the study at the time of admission. X2 test was used to compare proportions between the groups. Means were compared by student-t test. Duration of resuscitation, time to first breath, time to first cry and apgar scores were compared by Mann-Whitney U test. Two way analysis of variance with replications was applied to study the effect of two treatment interventions on heart rate measured at 1, 5 and 10 minutes. Neonates in the room air group switched to 100% oxygen at 90 seconds were retained in the originally enrolled group and analyzed as intention to treat basis. Results A total of 433 asphyxic babies (66 from Delhi; 180 Chennai, 89 Chandigarh and 98 from Lucknow) were enrolled from four centers. Two babies meeting the exclusion criteria were excluded from analysis. Thus only 431 babies were considered for analysis. Of these 210 babies received room air and 221 babies 100% oxygen for resuscitation (Fig. 1).
Table I gives the profile of important maternal, labour and neonatal characteristics. The two groups were comparable in terms of duration of labour, induction of labour, presence of fetal distress, and/or meconium-stained liquor and type of delivery. They were also comparable for birth weights and gestation. TABLE I Base line Maternal and Neonatal variables
*Includes data only of 3 centers: number of subjects in room air group = 168 (LSCS = 54) and in 100% oxygen group = 174 (LSCS = 73), percentages are calculated from 3 center data. TABLE II Outcome variables in Babies Resuscitated with Room Air and 100% Oxygen
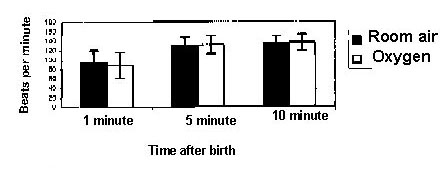
Table II summarizes the important outcome parameters in the two groups. The median apgar score at 5 and 10 minutes, time to first breath and treatment failure were similar in both the groups. Median time to first cry and median duration of resuscitation was significantly longer in 100 % oxygen group. Also, the room air group had significantly higher 1 minute apgar score than the oxygen group. Mean (SD) heart rates (bpm) at 1, 5 and 10 minutes after birth were 94.4 ± 26.1, 131.5 ± 17.7, 135.4 ± 14.1 and 87.7 ± 27.6, 131.1 ± 14.3, 135.8 ± 17.5 in babies resuscitated with room air and 100% oxygen respectively (Fig. 2). Two way analysis of variance with replications for heart rate measured at 1 min, 5 min and 10 min did not show any significant difference in the treatment groups, or interaction between the treatment regimen and time after birth.
Fig.2. Heart rate (mean, SD) changes in room air and oxygen group at 1,5 and 10 minutes A total of 157 (36.4 %) babies, 75 (35.7%) in the room air group and 82 (37.1%) in the 100% oxygen group had developed hypoxic-ischemic encephalopathy (HIE) during first 7 days of life. The proportion of babies in stages I, II and III of HIE were 22.6%, 8.9%, 8.3% in the room air and 16.7%, 14.9%, 9.8% in the oxygen group. These differences were not significant. Excluding the babies who died or were discharged from hospital, a total of 367 babies were available on day 7 for assessment of neurological status, 185 in the room air group and 182 in the 100% oxygen group. Of these 21 (11.3%) babies in the room air and 16 (8.8%) babies in the 100% oxygen group still had features of HIE (p = 0.41). Mortality was comparable between the groups (OR 0.64, 95% CI 0.36-1.13). Of asphyxia related mortality, 19 babies in the room air and 25 babies in 100% oxygen group were observed to have treatment failure at 90 seconds. These differences were statistically not significant. Discussion Birth asphyxia is not only a major cause of early neonatal mortality, it is also an important cause of neuromotor disability in children. The standard recommended practice for resuscitation of asphyxic newborn babies has been the use of 100% oxygen for assisted ventilation(3). Experimental studies in animals(7-10) and pilot studies in neo-nates(11-12) have indicated that room air is as effective as 100% oxygen in resuscitation of asphyxic newborns. Studies have also indicated that excess release of free oxygen radicals when high concentration of oxygen is used for resuscitation may exacerbate brain injury(4-6). Experimental studies in animals(7-10) has shown that outcome of resuscitation with room air is comparable to the outcome of resuscitation with 100% oxygen. In a study in newborn rabbits no difference was observed in time to first breath and survival whether room air or oxygen was used for resuscitation(7). Studies carried out in young and newborn pigs with room air have also demonstrated that room air resuscitation normalizes blood pressure, acid-base vari-ables and cerebral blood flow as efficiently as 100% oxygen(8-10). These observations have important implications in developing countries like India where almost two thirds of deliveries are taking place at home or in facilities where oxygen is not available. Preliminary studies comparing room air with 100% oxygen for resuscitation of the asphyxiated newborn have indicated that room air is as effective as 100% oxygen(11-13). In the study carried out by Ramji, et al. (11), 84 neonates were resuscitated with either room air or 100% oxygen. Heart rate came to normal as quickly in the group resuscitated with room air as in the 100% oxygen group. Apgar score at 1 minute was similar in both the groups, but at 5 minutes, apgar score was higher in the room air group than in the oxygen group. In a subsequent multicentric study Saugstad, et al.(12) also did not find any difference in heart rate observed during first 30 minutes of life in asphyxiated neonates resuscitated with either room air or 100% oxygen. There were significantly more babies with very low 1 minute apgar score in the 100% oxygen group than in the room air group. However, at 5 minutes and 10 minutes of age there was no significant difference between the two groups. Time to first breath was also found to be shorter in the room air group as compared to the 100% oxygen group. There were no significant differences in mortality or HIE between the two treatment groups. More recently, Vento, et al.(14) studied 830 asphyxiated asphyxic newborns over a six years period and observed that the room air group required shorter time of positive pressure ventilation and the oxygen group showed significantly more oxidative stress as compared to room air group even upto 28 days of life. The present study has also shown that outcome of asphyxiated babies resuscitated with room air is similar to those resuscitated with 100% oxygen. There were no significant differences in the improvement in heart rate measured at 1, 5, and 10 minutes and in the apgar score in the two treatment groups at 5 and 10 minutes, time to first cry and duration of resuscitation were significantly shorter in room air than in the 100% group. There were 39.0% babies in room air and 40.3% in the 100% oxygen group who were designated as treatment failure at 90 seconds, and this is similar to that reported in the earlier studies(12,14). Overall mortality in the group resuscitated with room air (12.4%) appeared lower than in the group resuscitated with 100% oxygen (18.1%). Asphyxia related mortality was also higher in the group resuscitated with 100% oxygen (13.6%) than in the room air group (10.0%), but the difference was not statistically significant. The observations of the present study are similar to that of the previous studies, which have also demonstrated that room air resuscitation is as effective as resuscitation with 100% oxygen. Though purists may argue about the lack of randomization as lacunae, it may be worth pointing out the results of both the present and previous multicentric study are similar. Besides, the results of these studies are also in agreement to that of the randomized, blinded trial of Vento, et al.(14). The finding of these clinical studies indicate that there is an emerging need to change resuscitation guidelines for newborns. These findings have important implications especially in situations where oxygen is not available for resuscitation of asphyxic newborns. The recent NRP 2000 guidelines also now recommends that room air ventila-tion can be used as an-alternative if 100% supplemental oxygen is not available(15). However, long term follow up studies need to be carried out to assess neurodevelopmental outcome in babies resuscitated with room air and 100% oxygen. The subset of preterm population in the present study was too small to conclude on efficacy of room air for assisted ventilation of preterm; this needs to be researched. Acknowledgement The authors are grateful to the superintendent of the hospitals for allowing to carry out the study and also to Ms. S. Choudhury, Ms. U. Dhillon and Mr. Lakshmi-narayan for the support in data cleaning and data entry. The authors also acknowledge the inputs provided by Dr. S.K. Bhargava, eminent pediatrician during planning of the study protocol. Contributors: SR designed the study, conducted the study, helped in analysis, reviewed and edited the manuscript. RR made tabulation plan, helped in analysis and drafted the manuscript. PKM, AN and IS conducted the study. AN Kapoor monitored the study initially. AM did data management and was the programmer of the study. IK and AM conducted the analysis. BNS coordinated the study and NCS reviewed the manuscript and will act as guarantor for the paper. Funding: Indian Council of Medical Research, New Delhi. Competing interest: None.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()