|
Nandkishor S. Kabra
Ganesh Srinivasan
Rekha H. Udani
From the Department of Neonatology, KEM Hospital, Parel, Mumbai 400 012, India.
Reprint requests: Dr. Nandkishor S. Kabra, 3/58 Epping Road, Lane
Cove, Sydney, NSW2066, Australia. E-mail:
[email protected]
Manuscript Received:
June
12, 1998;
Initial review completed: August 12, 1998; Revision Accepted: February 18, 1999
The birth of child with a caudal appendage resembling a tail generates an unusual amount of interest, excitement and anxiety (1). True human tail is a rare event with fewer than 40 cases reported in the literature(2). It is defined as a caudal, vestigial, midline protrusion with skin covering a combination of muscle and adipose tissue(3). We are reporting a case of true tail in a neonate, a rare event in human.
Case Report
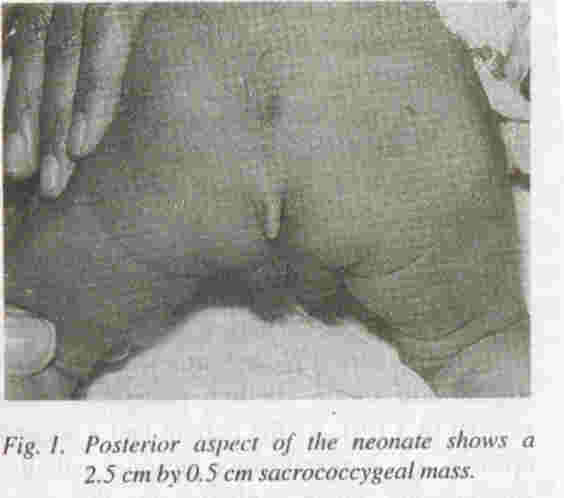
A 3 kg male neonate delivered at our hospital was the product of full term gestation to 30 years old primigravida mother with no history of drug exposure during pregnancy or diabetes mellitus. The general and systemic examination of neonate was essentially normal except for tuft of hair in sacrococcygeal region in midline and a soft tissue tail like mass in the same region just below the tuft of the hair (Fig. 1). Possibility of true neonatal tail verse's pseudotail was considered. The neonate did not have any other congenital anomaly. There was no family history of con- genital anomaly. The soft tissue mass in the sacrococcygeal region was tail like, soft, well circumscribed measuring 2.5 cm by 0.5 cm.
Radiography and ultrasonography of spine did not show any abnormality. This ruled out the possibility of spinal dysraphisam and parasite fetus (pseudotail).
For confirming the diagnosis of true tail, surgical excision of mass was planned, but very unfortunately it was not carried out as parents refused to give consent. Despite repeatedly explaining the parents, the simple nature of surgical excision of the mass, need for confirmation of diagnosis and excision being the definitive therapy for true tail; they have refused to do so. They have not followed up with us later on inspite of persuasion.
Discussion
Caudal appendages are unusual malformations and are divided into true tails and pseudotails (lipoma, teratoma, myelomeningocoele and parasitic fetus)(3). Simple surgical excision of true tail has been advocated(4). However, recent reports emphasize the associated midline anomalies that might change the surgical approach in these patients(5-7). It is important to make distinction between true and pseudotail in lumbosacaral region since the treatment and prognosis are different(2).
A true tail in human is vestigial and never contains vertebrae in contrast to vertebrate animals. It has been suggested that true tail is a dermal appendage coincidentally located in the sacrococcygeal
region(1). In most patients it is located in the sacrococcygeal region and can be located 1.5 cm to one side. Though anomaly occurs in both sexes, a slight predominance in males is known(8). It affects all races(8). Familial cases have been reported(3). Caudal appendages are reported also to be associated with other congenital anomalies in 29% of cases(9) and spina bifida has been the most frequent coexisting anomaly. Cleft palate was reported once(10). Spinal dysraphism should be excluded in all
patients with caudal appendages prior to excision since neurosurgical intervention may be required(6,7). A thorough neurological examination and imaging studies of the vertebral column are recommended to exclude this possibility(9). In a recently reported case, congenital heart disease, anal and vaginal atresia and horseshoe kidney were associated midline anomalies(2). Our patient did not have any other midline anomaly or other con- genital abnormality. Several previous reports documented movement and contraction of tail(3), whereas others indicated lack of move- ment(2) as in our neonate.
Microscopic examination of all true human showed skin covering a core of adipose tissue, collagen fibers and skeletal muscle fibers. No bone or cartilage has been documented. An associated lipoma(6), lipomeningocele(6,7), capillary hemangioma(8), or juvenile hemangioendothelioma(10), well
developed neurones, glial fibers, and calcification have also been reported(6).
After excluding associated spinal deformities, surgical removal is the treatment of choice. A thorough histopathologic examination of the mass is recommended to exclude teratomatous growth or other neoplasms(2).
Acknowledgements
We wish to thank Dr. P.M. Pai, Dean, Seth G.S. Medical College and K.E.M. Hospital for granting permission to publish this report.
|
1.
Ledley FD. Evolution and the human tail. N Engl J Med 1982; 306: 1212-1215.
2.
Alashari M, Torakawa 1. True tail in a new- born. Pediatr Dermat 1995; 12: 263-266.
3.
Dao AH,Netsky MG. Human tails and pseudotails. Hum Patho11984; 15: 449-453.
4. Spiegelmann R. Schinder E, Mintz M, Blaksein A. The human tail a benign stigma. J
Neurosurg 1985; 63:
461-462.
5.
Ohhara Y. Human tail and other abnormalities of the lumbosacrococcygeal region relating to tethered cord syndrome. Ann Plast Surg 1980; 4: 507-510.
6.
Belzberg AJ, Myles ST, Trevenen CL. The hu- man tail and spinal dysraphism. J Pediatr Surg 1991; 26: 1243-1245.
7.
Matsumoto S. Yamamoto Y, Okura K. Human tail associated with lipomeningocoele.Neurol Med Chir (Tokyo) 1994; 34: 44-47.
8.
Parsons RW. Human tails. Plast Reconstr Surg 1960; 25: 618-621.
9.
Durbow TJ, Wackyn PA, Leasavoy MA. De- tailing the human tail. Ann Plast Surg 1988; 20: 340-344.
10.
Lundberg GO, Parsons RW. A case of human tail. Am J Dis Child 1962; 104: 72-73.
|