|
|
|
Indian Pediatr 2020;57: 834-841 |
 |
Consensus Statement of Indian Academy of
Pediatrics on Early Childhood Development
|
|
Ketan Bharadva, 1 Digant
Shastri,2 Narayan Gaonkar,3
Rhishikesh Thakre,4
Jayashree Mondkar,5 Ruchi
Nanavati,6 Suchit Tamboli,7
Swati Vinchurkar,8 Antony
Kollannur R,9 Samir Dalwai,10
Mahesh Patel,11 Parul Valia,12
Leena Srivastava,13 Chhaya
Prasad,14 Amola Patel,15
Jeeson Unni16 and
Somashekhar Nimbalkar17
From 1Infant and Young Child Feeding Chapter of Indian Academy of
Pediatrics (2019-2020); 2Indian Academy of Pediatrics (2019); 3UNICEF,
Gujarat; 4Consultant Neonatologist Aurangabad, Maharashtra; 5Department
of Pediatrics, LT Medical College & General Hospital, Mumbai,
Maharashtra; 6Department of Neonatology, KEM Hospital, Mumbai,
Maharashtra; 7Developmental Pediatrician, Ahmednagar, Maharashtra; 8Urja
Development Center, Surat, Gujarat; 9National Health Mission, Ernakulam,
Kerala; 10New Horizon Group, Mumbai; 11Consultant Pediatrician, Surat,
Gujarat; 12Developmental Pediatrician, Baroda, Gujarat; 13Neuro
Developmental Pediatrics Chapter of Indian Academy of Pediatrics
(2018-2019); 14Developmental Pediatrician, Chandigarh; 15Developmental
Pediatrician, Ahmedabad, Gujarat; 16Neuro Developmental Pediatrics
Chapter of Indian Academy of Pediatrics (2018-2019); 17Department of
Pediatrics, Karamsad Medical College, Karamsad, Gujarat; India.
Correspondence to: Dr. Ketan Bharadva, Masoom Children’s Hospital,
1st Floor - Mayuri Apartment, Bhulka Bhavan Crossing, Near Water Tank,
Adajan, Surat 395009, Gujarat State, India.
Email: [email protected]
Published online: May 22, 2020;
PII: S097475591600185
|
|
Justification:
Early Childhood Development
(ECD) has lifelong impact on learning, education,
productivity, socio-emotional functioning, health and
disease. A Consensus Statement for promoting ECD is needed
to improve patient care and promote research. Process:
Indian Academy of Pediatrics convened a National
Consultative Meeting on 20 September, 2019 at Surat to
discuss the way forward for pediatricians in ECD and form a
consensus advisory statement. Experts from Chapters of
Infant and Young Child Feeding, Neurodevelopmental
Pediatrics, Neonatology, Growth Development and Behavior,
Adolescent Health Academy, Parenting for Peace and UNICEF
participated. Objectives: To formulate, endorse and
disseminate a consensus advisory statement of working at
current levels of resources and to build future framework
for ECD from Indian perspective. Conclusions:
Interventions for ECD should begin from conception to
adolescence, prioritized in first 3 years, inclusive and
equitable for all, especially for high risk, vulnerable and
marginalized families. Pediatric clinics can play a pivotal
role as cost effective delivery points for guidance and
interventions. Age appropriate approaches, active care
giver’s involvement, advocacy and integration with different
sectors, community and policy makers should be done to
enable supportive environment. Research should be promoted
into finding cost effective novel scalable interventions.
Keywords: Intervention,
Management, Screening, Surveillance.
|
|
E
arly Childhood (up to 6 to 8 years) is the time
of formation of base of all lifetime learning, education, productivity,
socio-emotional functioning, health and disease. A slight shift in
trajectory of child development in its initial journey can make a huge
drift in its adulthood outcomes. Adversities and support during
pregnancy, early childhood to adolescence have potential to change the
whole life of the individuals and the society.
The first 1000 days (conception to 2 years age) are
most sensitive and crucial in development [1]. Neuroplasticity declines
after early childhood. Thereafter less stimulated synapses during first
1000 days get pruned and will be lost for a life time [2]. Science has
also begun to decipher the impact of environmental factors and parenting
quality on genetic expressions spreading over more than one generation
[3]. Children’s developing brain needs nurturing care [4] in the form
of: good healthcare; enriching nutrition with responsive feeding [5];
stimulating experiences with responsive positive parenting (prompt,
consistent and appropriate child-caregiver interactions with play, talk
and love); early learning provided by parents and family members [6];
and security and safety. They should be supported by an environment
enabling such needs. It is also evidenced that deficits in ECD (Early
Childhood Development) cannot be effectively repaired when interventions
are done after 24 to 36 months age [7,8].
The prevalence of improper child development is much
higher than generally estimated. The four risk factors are recognized as
eligible for prompt actions are: stunting, low cognitive stimulation,
iodine deficiency, and iron deficiency anemia. With majority childhood
adversities being manageable and preventable the interventions in ECD
are far more warranted as cost effective. ECD has far reaching
implications in development of nation and inactions in ECD are very
costly [9].
IAP has long recognized the importance of a focus on
brain development. There are dedicated chapters to the cause of specific
areas of ECD. Assimilation of currently published guidelines related to
ECD and bridging the gaps in view of needs of ECD should be done as a
detailed module. From amongst these some guidelines are already in place
and published by IAP and its sub-chapters on topics of neonatal
resuscitation, different aspects of nutrition and feeding, child safety,
immunization, disabilities, etc [10-22].
Pediatric clinics and hospitals are point of care
opportunities for ECD care. High risk assessment, anthropometric
monitoring, treatment of illnesses, immunization, diet counseling and
therapeutic ties with families are routine for them. Busy practices
frequently miss developmental surveillance and screening, anticipatory
guidance including safety and tips for responsive nurturing parenting
care. They can be developed to work comprehensively for ECD to improve
patient care and promote research (Web Table I) [23].
OBJECTIVES
Increasing importance and evidences of ECD mandates
the need for formulation of consensus guideline statement on it for the
Indian pediatric facilities to work comprehensively, based on WHO (World
Health Organization) - UNICEF (United Nations Children’s Fund) framework
on Nurturing Care for ECD. To gather the currently available resources
published by IAP (Indian Academy of Pediatrics) backing up the ECD; and
gaps where pediatric facilities can work better or do advocacy or
liaison with other faculties in improving ECD. To formulate and
disseminate a comprehensive advisory for pediatric facilities in
contributing to ECD, and to make a framework for future actions in ECD.
The consensus guideline would help achievement of Sustainable
Development Goals (SDGs) and global targets set in Comprehensive
Implementation Plan on Maternal, Infant and Young Child Nutrition; and
The Global Strategy for Women’s, Children’s, and Adolescents’ Health.
PROCESS
IAP organized a National consultative meeting of
experts on 20 September, 2019, during the West zone PEDICON at Surat.
Experts from United Nations Children’s Fund and Indian Academy of
Pediatrics from fields of developmental pediatrics, neonatology,
nutrition and feeding, neurology, public health, child safety and
general pediatrics from different parts of India were present at the
discussion. Discussion took place for development in different age
groups. Detailed articles were submitted later on them to formulate a
module. This consensus statement is formed as an excerpt of the
discussions and contents of the draft module. Search was made in
databases of MEDLINE through Pubmed, Google Scholar, Cochrane library,
and recent systematic reviews using combination of keywords viz.,
early childhood development, stimulation, early intervention, nurturing
care, responsive feeding, child nutrition, child safety, parenting, care
for development, preschool learning. Child development, infant and young
child feeding, parenting nurturing care, india, first 1000 days, and
further expanded through related articles and reference lists of the
articles.
RECOMMENDATIONS
General Recommendations
• WHO-UNICEF guidelines on Care of development
[24,25] be adapted as reference for care development frame, till new
Indian research-based evidence is available.
• IAP should join global partnership for ECD –The
ECD Action Network (ECDAN).
• Psychosocial interventions to support maternal
mental health should be integrated in early childhood health and
development services [25]. All mothers should be screened for
depression between 1 and 3 months postnatally. Parenting
interventions improves maternal depression also [26]. During routine
visits for child, mothers should be guided and reminded to take iron
and calcium supplements and healthy diet; and visit
obstetrician/family physician for general health, contraception,
family planning, reproductive and sexual health.
• Pediatricians should lead awareness generation
in care givers and the development of training module for frontline
workers.
• Family focused care with adequate involvement
of fathers is a must. The health and leave policies should be family
friendly [24].
• Gender equity and female education should be
propagated.
• Identification and attention to specific needs
of vulnerable, at risk and marginalized children during routine care
should be done with extra efforts [24].
• Promote early responsive caregiving (positive
parenting) and early learning. Support for it should be included as
part of interventions for optimal nutrition of infants and young
children as responsive feeding strategies. Parents and other
caregivers should be supported in doing so [5,24,25]. Encourage and
support combined play times, life skill education and emotionally
healthy home and school environments. Promote age-appropriate play
and cultural toys. In resource-poor settings delivery of parenting
inter-ventions by trained non-professionals through local community
organizations should be promoted [26].
• Pediatricians should routinely talk to parents
and caretakers of children under 5 years of age regarding adequacy
of physical activity, sedentary behavior and sleep [27].
• Care takers should be routinely guided about
regulations and guidelines for use of screens and digital devices
right from the delivery rooms, to TV programs and internet
availability for children in school and homes, especially background
running of television before the age of 2 years [28].
• ECD needs a structured approach at
pediatricians’ clinics using a comprehensive checklist.
o Age group-wise single page content health
file should be made in line of MCP (mother child protection)
card to include each domain of ECD viz., standardized nutrition,
development, parenting tips, stimulation, preschool learning and
safety advices.
o Display of public information of ECD
domains in waiting rooms including audio visual formats should
be done.
o A parent friendly IAP digital app for
comprehensive approach to ECD should be made and disseminated.
• Advocacy and integration be done with other
sectors like obstetrics, education, social welfare, child safety,
politics, international, national and local - social or governmental
agencies and media at large etc. Facilitate formation,
funding, implementation, coordination and monitoring-evaluation of
high quality intervention programs and public policies [4,24].
• Expert inputs are needed to finalize the
preschool learning & education advises by pediatricians:
o Awareness among caretakers of early
childhood including school teachers and policy makers, about all
aspects of child development, emotions and behavior at different
ages, guidance on safety-security, sleep, nutrition and screen
viewing.
o Awareness in preschool teachers in age
appropriate activities, pre-reading, pre-writing and attention
skills, should be universal [29].
o School / daycare crèche policies,
guidelines and trainings should be developed in consultation
with IAP for age, development, behavioral and emotion
appropriateness. Guidelines for school entry with readiness and
age appropriate activities at schools.
• Curriculum for graduate and postgraduate
medical students should also include socio-emotional,
speech-language, and social communication domains of development.
• Promote research in developing local and
innovative methods in ECD science and delivery of care.
• Anganwadis need an additional trained worker in
early stimulation and care for child development for under-3
children in addition to current practice of only pre-school
education of 3-6 years.
• Pediatric facility staff needs to be trained to
sensitively facilitate identification and referral for safety and
security issues of children. Facilities should display/disseminate
relevant awareness material [20,22].
Recommendations in Neonatal Period
• Early identification and treatment of perinatal
asphyxia in delivery room.
• Identifying high risk newborn following birth
and at hospital discharge.
• Stratification of newborn based on risk factors
(Table-I) [30]. Other risk factors for neuro
developmental delay are preterm babies with any one or more of: PDA
(patent ductus arteriosus, NEC (necrotizing enterocolitis, CLD
(chronic lung disease), recurrent apnea, EUGR (extra uterine growth
restriction), shock, PPHN (persistent pulmonary hypertension in
newborn), complex congenital malformations, need of significant
resuscitation, need for postnatal steroids, post surgery of CDH
(congenital diaphragmatic hernia) and TEF (tracheo-esophageal
fistula).
• Metabolic and hearing screening for all normal
newborns.
• Identification of ‘high risk’ newborns and
screening for significant hyperbilirubinemia (BIND Score and use of
Bhutani’s hour specific nomogram chart [31,32]
• Optimizing nutrition: Ensuring lactation by
breastfeeding, helping maintenance of lactation in mothers of babies
admitted in NICU and early detection and support for breastfeeding
problems.
• Screening for hypoglycemia: Identify ‘at risk’
and screen all ‘high risk’ and sick newborns for glucose at 2 hours
of age and every 4-6 hourly till first 48 hours of age and full
feeds.
• Detection and management of postnatal hypoxia
(for preterm newborn - Silverman Anderson Score, for full term
newborn – Downes and Vidyasagar Score).
• Developmentally Supportive Care (DSC) in NICU
including promotion of KMC (Kangaroo Mother Care) as comprehensive
maternal care for development and nutrition.
• Follow up of NICU graduate using checklist. ‘At
risk’ neonates may seem healthy and NICU graduates need a structured
follow up, as they are at risk of significant neuro morbidity [33].
Table I Risk Factor-based Stratification for Follow-up Care
|
At risk |
Risk factors |
Care by |
|
Mild |
>37 week, >2.5 kg, HIE stage I, Transient hypoglycemia,
Suspected sepsis, |
Pediatrician |
|
Jaundice in preterm, Grade I/II IVH (intraventicular hemorrhage) |
|
|
Moderate |
33-36 weeks, 1500-2500 gms, HIE stage II, Sepsis, jaundice with
exchange
|
Neonatologist / developmental
|
|
transfusion, >Grade II IVH, Prolonged encephalopathy,
Uncomplicated
|
pediatrician |
|
course on ventilation, Hypoglycemia >3 days, Need for some
resuscitation |
|
|
Severe |
<1500 gms, <33 weeks, Multi organ injury, HIE stage III, >7 days
|
Developmental Early Intervention
|
|
ventilation, meningitis, kernicterus, abnormal neurologic
exam at
|
Centre (DEIC) |
|
discharge, PVL (periventricular leucomalacia) or hydrocephalus, |
|
|
low Apgar at 5 min., Symptomatic hypoglycemia |
|
|
Modified from reference 30; HIE: Hypoxis ischemic
encephalopathy. |
Interventions in the Neonatal Unit
The core objective of management of high risk babies
is to have a ‘brain protective’ management strategy throughout the
course of stay in NICU. Common brain protective strategies that need to
be kept in mind include [34]:
• Care during resuscitation: Use room air
/ low oxygen up to 30%, for babies >32 weeks of gestation, tailoring
oxygen delivery based on recommended target oxygen saturation in the
first minutes after birth, labor room CPAP (Continuous Positive
Airway Pressure) stabilization for preterm [10].
• Optimizing nutrition: EUGR is associated
with poor neuro developmental outcomes [35]. Use mother’s own milk
(MOM), donor human milk (DHM), TPN (total parenteral nutrition),
early trophic feeds. Use of MOM/DHM for its benefits in reducing
late onset sepsis, NEC and ROP (retinopathy of prematurity)
[12,13,15].
• Gentle Ventilation: Non-invasive
ventilation/gentle ventilation/volume targeted ventilation to reduce
incidence of BPD (broncho pulmonary dysplasia) and related morbidity
[36].
• Maintaining hemodynamic stability to
minimize post-natal ischemic brain injury [37].
• Therapeutic hypothermia: For babies with
HIE (hypoxic ischemic encephalopathy), if facilities exist [38].
• Neuro-protective care/Brain sensitive
care/DSC [39,40]: Protect sleep cycles, especially REM (rapid
eye movement) sleep; quiet environment (<45 dB); protecting eyes
from bright lighting; clustering of care; hourly ‘no touch’ rounds;
reduction of positional deformities by maintaining infants in a
midline, flexed, contained, comfortable position with nesting, hand
containment, swaddling and gentle handling; and prolonged KMC [41].
• Skin care: Minimize use of tape, moisten
adhesive skin interface before removal [42].
• Promote self-regulation and
neurodevelopmental organization: ‘cue based care giving’ by
identifying stress cues, stability cues and self-help cues for
autonomic, motor and state stability.
• Tactile stimulation: Touch, gentle
massage.
• Minimizing pain: Non-pharmacologic and
pharma-cologic pain relief, containment, hand holding, KMC,
breastfeeding/breastmilk use, non-nutritive sucking, oral sucrose
[43].
• Involvement of family members in care of baby
and decision-making.
Neonatal Developmental Intervention by Family Members
at Home
• Visual stimulation: Decoration of
surroundings, with moving and brightly colored objects. Black and
white contrast sends the strongest signals to newborn brain.
• Auditory stimulation: By talking,
singing, recorded mother’s voice, recorded heart beat and musical
toys. Radio, television etc sounds should be avoided in first
two years.
• Tactile stimulation: Non–nutritive
sucking, stroking, flexing, massaging with or without oil or cream,
rubbing, positioning and giving bath. Massage advices are not
recommended in high risk neonates with increased muscle tone.
Massage should be done very carefully in preterm babies and term
babies having asymmetric reflexes or neurologic compromise.
• Vestibular-kinesthetic stimulation:
Rocking, oscillating beds e.g., water beds.
• Carry in arms: Avoid use of baby pods
and cots. They interfere with the proprioceptive sensory input which
the baby gets when carried in the arms of the caregiver.
• Avoid overstimulation.
Recommendations in Post-neonatal Period
• Age appropriate development surveillance using
red flags checklist at each routine healthy baby visits. Problems
found during it should be addressed with screening test [44].
• Display of red flags and basic stimulation tips
at different ages in waiting areas.
• All children should undergo developmental
screening using standard tools at 9, 18, 24 and 36 months [44,45].
• Detailed assessment to be undertaken of high
risk children and screening positive cases.
• Early intervention for the high risk and
developmentally delayed children.
• Stimulation and parenting advices to be
delivered in waiting rooms by trained health care workers. Use CDC
(Centers for Disease Control and Prevention) milestone tracker app
till evidence based Indian app on public domain is available.
• The international prescriptive standards
designed by WHO multi-centric study are recommended for growth
monitoring. Each well baby visit should incorporate nutrition
monitoring and advices.
• Use Child Behavior Checklist (CBCL) for early
pick up of problems like attention deficit.
• School readiness screening should be encouraged
at pediatric clinics before the child is placed in preschool or
kindergarten [46].
• Mapping of facilities for detailed diagnostic,
therapeutic and supportive medical and nonmedical services will be
done by the NDP (Neuro developmental pediatrics) and GDBP (Growth
development and behavior) chapters and published in the module.
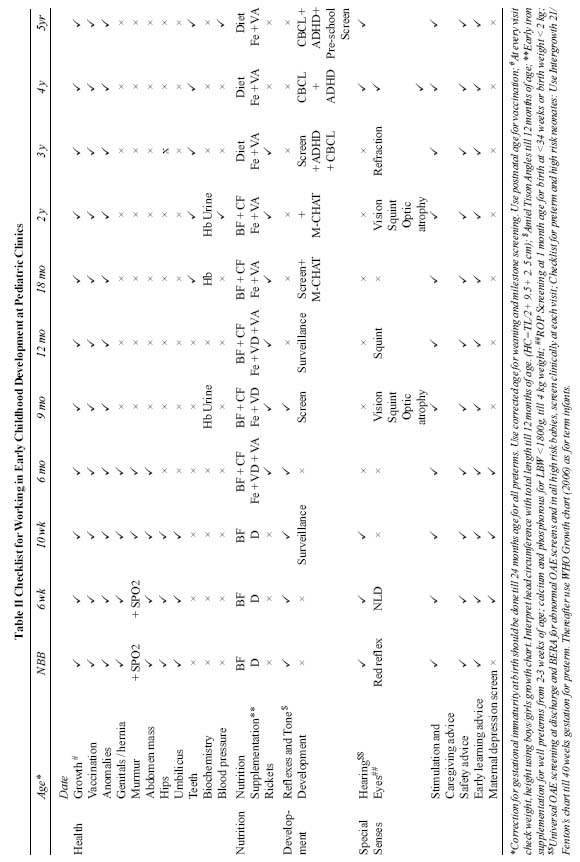
For purpose of including in routine practice, the
recommended actions are arranged age-wise as a checklist (Table II).
Conclusions
This consensus statement is envisaged to guide Indian
pediatric fraternity to improve practices and advocacy in ECD as per
view of experts from across the country. There is urgent need to act
fast in this subject in consideration of low awareness towards combined
efforts in its divergent areas. Convergence of efforts with other
medical and nonmedical faculties will bring newer aspects of promoting
ECD. Newer evidences are building up fast in this subject, which will
lead to update of this consensus with the feedbacks from field gather.
Disclaimer: This consensus statement is prepared
for assisting pediatricians in accordance with current scientific
evidence and guidelines for acting in early childhood development as a
whole; however, many areas are still not clearly defined. These
statements cannot establish a standard of care, and decisions about
treatment should be based on the judgment of the clinician on the merits
of the individual cases dealt by them.
Funding: UNICEF-Gujarat funded the national
consultative meeting for preparation of this advisory. It had no role in
the development of the content of the advisory.
Competing interests: None stated.
Annexure
Participants at the National Consultative Meeting for
IAP Consensus Guidelines on ECD (in alphabetical order):
Dr. Abraham Paul, Developmental Pediatrician,
Ernakulam; Dr. Amola Patel, EB member GDBP Chapter of IAP,
Ahmedabad; Dr. Antony Kollanur R, Consultant, Public Health,
Child Survival and Development. Ernakulam; Dr. Arun Phatak,
Baroda; Dr. Bipin Desai, Surat; Dr. Chetan B Shah, Surat;
Dr. Chhaya Prasad, Developmental Pediatrician, Chandigarh; Dr.
Digant Shastri, President Central IAP; Dr. Hariprakash Hadial,
Newborn Care Consultant, UNICEF Gujarat; Dr. Hitesh Jariwala,
President SPACT Surat; Dr. Hitesh Shinde, Secretary SPACT, Surat;
Dr. Jeeson Unni, President NDP Chapter, Ernakulam; Dr. Kamlesh
Parekh, ‘Parenting for Peace’ Surat; Dr. Kanaksinh Surma, Surat;
Dr. Ketan Bharadva, President IAP-IYCF Chapter, Surat; Dr.
Kirit Sisodiya, Pediatrician, Surat; Dr. Leena Srivastava,
Secretary NDP Chapter, Pune; Dr. Mahesh Patel, Pediatrician,
Surat; Dr. Milind Wadekar, President SOG-FOGSI, Surat; Dr.
Nandini Mundkur, Developmental Pediatrician, Banglore; Dr. Nirav
Jariwala, Pediatrician Surat; Dr. Parul Valia, Developmental
Pediatrician, Baroda; Dr. Prashant Kariya, Secretary AHA-Surat,
Surat; Dr. Rakesh Desai, Pediatrician Surat; Dr. Ravindra
Bagal, Health Officer, UNICEF, Gujarat; Dr. Rhishikesh Thakre,
Neonatologist, Vice President NNF, Aurangabad; Dr. Ritesh Shah,
Pediatric Neurophysician, Surat; Dr. Ruchi Nanavati,
Neonatologist Mumbai; Dr. Salim Hirani, President AHA-Surat,
Surat; Dr. Samir Dalwai, Developmental Pediatrician, Mumbai;
Dr. Somashekhar Nimbalkar, Neonatologist, Karamsad; Dr. Suchit
Tamboli, Developmental Pediatrician, IPP GDBP Chapter of IAP,
Ahmednagar; Dr. Sushma Desai, EB member AHA, Surat; Dr. Swati
Vinchurkar, Developmental Pediatrician, Gujarat Coordinator NDD
Chapter, Surat.
Invited but could not attend the meeting: Dr. MKC Nair
(Trivandrum), Dr. Vibha Krishnamurthy (Mumbai), Dr. Roopa Srinivasan
(Mumbai), Dr. Pankaj Buch (Jamnagar), Dr. Jayashree Mondkar (Mumbai) and
Dr. VP Goswami (Indore).
REFERENCES
1. Christian P, Murray-Kolb LE, Tielsch JM, Katz J,
LeClerq SC, Khatry SK. Associations between preterm birth,
small-for-gestational age, and neonatal morbidity and cognitive function
among school-age children in Nepal. BMC Pediatr. 2014;14:58.
2. Tierney AL, Nelson CA. Brain development and the
role of experience in the early years. Zero Three. 2009;30:9–13.
3. Lake A, Chan M. Putting science into practice for
early child development. Lancet. 2015;385:1816–7.
4. Black MM, Walker SP, Fernald LCH, Andersen CT, Digirolamo AM, Lu
C, et al. Advancing early childhood development: from science to
scale 1. Lancet. 2017;389:77-90.
5. Black MM, Aboud FE. Responsive Feeding Is Embedded
in a Theoretical Framework of Responsive Parenting. J Nutr.
2011;141:490-4.
6. Eshel N, Daelmans B, Cabral De Mello M, Martines
J. Responsive parenting: Interventions and outcomes. Bull World Health
Organ. 2006;84:992-8.
7. Windsor J, Benigno JP, Wing CA, Carroll PJ, Koga
SF, Nelson CA, et al. Effect of foster care on young children’s
language learning. Child Dev. 2011;82:1040-6.
8. McLaughlin KA, Sheridan MA, Tibu F, Fox NA, Zeanah
CH, Nelson CA, et al. Causal effects of the early caregiving
environment on development of stress response systems in children. Proc
Natl Acad Sci USA. 2015;112:5637-42.
9. Richter LM, Daelmans B, Lombardi J, Heymann J, Boo
FL, Behrman JR, et al. Investing in the foundation of sustainable
development: pathways to scale up for early childhood development.
Lancet. 2017;389:103-18.
10. Bansal SC, Nimbalkar SM. Updated neonatal
resuscitation guidelines 2015–major changes. Indian Pediatr.
2016;53:403-8.
11. Paul A, Prasad C, Kamath SS, Dalwai S, Nair MKC,
Pagarkar W. Consensus statement of the Indian Academy of Pediatrics on
newborn hearing screening. Indian Pediatr. 2017;54:647-51.
12. Tiwari S, Bharadva K, Yadav B, Malik S, Gangal P,
Banapurmath CR, et al. Infant and young child feeding guidelines,
2016. Indian Pediatr. 2016;53:703-13.
13. Bharadva K, Mishra S, Tiwari S, Yadav B, Deshmukh
U, Elizabeth KE, et al. Prevention of Micronutrient Deficiencies
in Young Children: Consensus Statement from Infant and Young Child
Feeding Chapter of Indian Academy of Pediatrics. Indian Pediatr.
2019;56:577-86.
14. Balasubramanian S, Shah A, Pemde HK, Chatterjee
P, Shivananda S, Guduru VK, et al. Indian Academy of Pediatrics
(IAP) Advisory Committee on Vaccines and Immunization Practices (ACVIP)
Recommended Immunization Schedule (2018-19) and Update on Immunization
for Children Aged 0 Through 18 Years. Indian Pediatr. 2018;55:1066-74.
15. Infant and Young Child Feeding Chapter, Indian
Academy of Pediatrics, Bharadva K, Tiwari S, Mishra S, Mukhopadhyay K,
Yadav B, et al. Human milk banking guidelines. Indian Pediatr.
2014;51:469-74.
16. Dalwai S, Choudhury P, Bavdekar SB, Dalal R,
Kapil U, Dubey A, et al. Consensus statement of the Indian
Academy of Pediatrics on integrated management of severe acute
malnutrition. Indian Pediatr. 2013;50:399-404.
17. Nair MKC, Prasad C, Unni J, Bhattacharya A,
Kamath SS, Dalwai S. Consensus statement of the Indian Academy of
Pediatrics on evaluation and management of learning disability. Indian
Pediatr. 2017;54:574-80.
18. Dalwai S, Ahmed S, Udani V, Mundkur N, Kamath SS,
Nair MKC. Consensus statement of the Indian academy of pediatrics on
evaluation and management of autism spectrum disorder. Indian Pediatr.
2017;54:385-93.
19. Dalwai S, Unni J, Kalra V, Singhi P, Shrivastava
L, Nair M. Consensus statement of the Indian Academy of Pediatrics on
evaluation and management of Attention Deficit Hyperactivity Disorder.
Indian Pediatr. 2017;54:481-8.
20. Seth R, Srivastava RN. Child Sexual Abuse:
Management and prevention, and protection of children from Sexual
Offences (POCSO) Act. Indian Pediatr. 2017;54:949-53.
21. Khadilkar A, Khadilkar V, Chinnappa J, Rathi N,
Khadgawat R, et al. Prevention and Treatment of Vitamin D and Calcium
Deficiency in Children and Adolescents: Indian Academy of Pediatrics
(IAP) Guidelines. Indian Pediatr. 2017;54:567-73.
22. Aggarwal K, Dalwai S, Galagali P, Mishra D,
Prasad C, Thadhani A. Recommendations on recognition and response to
child abuse and neglect in the Indian setting. Indian Pediatr.
2010;47:493-504.
23. Rushton FE, Kraft C. Building brains, forging
futures: the pediatrician’s role. Int J Pediatr Adolesc Med. 2014;1:3-7.
24. World Health Organization, United Nations
Children’s Fund WBG. Nurturing care for early childhood development: a
framework for helping children survive and thrive to transform health
and human potential. Geneva: World Health Organization; 2018.
25. Improving early childhood development: WHO
guideline. Geneva: World Health Organization; 2020.
26. Singla DR, Kumbakumba E, Aboud FE. Effects of a
parenting intervention to address maternal psychological wellbeing and
child development and growth in rural Uganda: a community-based, cluster
randomised trial. Lancet Glob Heal. 2015;3:e458-69.
27. Guidelines on physical activity, sedentary
behaviour and sleep for children under 5 years of age. Geneva: World
Health Organization; 2019.
28. Anderson DR, Subrahmanyam K and on behalf of the
Cognitive Impacts of Digital Media Workgroup. Digital screen media and
cognitive development. Pediatrics. 2017;140:S57-61.
29. Berlinski S, Galiani S, Gertler P. The effect of
pre-primary education on primary school performance. J Public Econ.
2009;93:219-34.
30. Kadam A. Follow up of high risk newborn. In:
Thakre R, Murki S, editors. Protocols in Neonatology. 2nd ed. New Delhi:
Jaypee Brothers; 2019.
31. Radmacher PG, Groves FD, Owa JA, Ofovwe GE,
Amuabunos EA, Olusanya BO, et al. A modified Bilirubin-induced
neurologic dysfunction (BIND-M) algorithm is useful in evaluating
severity of jaundice in a resource-limited setting. BMC Pediatr.
2015;15:28.
32. Bhutani VK, Johnson L, Sivieri EM. Predictive
ability of a predischarge hour-specific serum bilirubin for subsequent
significant hyperbilirubinemia in healthy term and near-term newborns.
Pediatrics. 1999;103:6-14.
33. Mwaniki MK, Atieno M, Lawn JE, Newton CRJC.
Long-term neurodevelopmental outcomes after intrauterine and neonatal
insults: A systematic review. Lancet. 2012;379:445-52.
34. Lea CL, Smith-Collins A, Luyt K. Protecting the
premature brain: Current evidence-based strategies for minimising
perinatal brain injury in preterm infants. Arch Dis Child Fetal Neonatal
Ed. 2017;102:F176-82.
35. Schneider N, Garcia-Rodenas CL. Early nutritional
interventions for brain and cognitive development in preterm infants: A
review of the literature. Nutrients. 2017;9:E187.
36. Jensen EA, Chaudhary A, Bhutta ZA, Kirpalani H.
Non-invasive respiratory support for infants in low- and middle-income
countries. Semin Fetal Neonatal Med. 2016;21:181-8.
37. Sahni M, Jain S. Hypotension in neonates.
Neoreviews. 2016;17:e579-89.
38. Natarajan G, Laptook A, Shankaran S. Therapeutic
hypothermia: How can we optimize this therapy to further improve
outcomes? Clin Perinatol. 2018;45:241-55.
39. Altimier L, Phillips R. The Neonatal Integrative
Developmental Care Model: Advanced Clinical Applications of the Seven
Core Measures for Neuroprotective Family-centered Developmental Care.
Newborn Infant Nurs Rev. 2016:230-44.
40. Milette I, Martel M-J, da Silva MR, Coughlin
McNeil M. Guidelines for the Institutional Implementation of
Developmental Neuroprotective Care in the NICU. Part B: Recommendations
and Justification. A Joint Position Statement From the CANN, CAPWHN,
NANN, and COINN. Can J Nurs Res. 2017;49:63-74.
41. Baley J. Skin-to-skin care for term and preterm
infants in the neonatal ICU. Pediatrics. 2015;136:596-9.
42. New Neonatal Skin Care Evidence Based Practice
Guideline. Nurs Womens Health. 2013;17:545–6.
43. Hardy W. Facilitating Pain Management. Adv
Neonatal Care. 2011;11:279-81.
44. Duby JC, Lipkin PH, Macias MM, Wegner LM, Duncan
P, Hagan JF, et al. Identifying infants and young children with
developmental disorders in the medical home: An algorithm for
developmental surveillance and screening. Pediatrics. 2006;118:405-20.
45. Mukherjee SB, Aneja S, Krishnamurthy V,
Srinivasan R. Incorporating developmental screening and surveillance of
young children in office practice. Indian Pediatr. 2014;51:627-35.
46. Shrivastava S, Patil V, Shelke M, Anvikar M,
Mathur A, Pathak A. Assessment of school readiness of children and
factors associated with risk of inadequate school readiness in Ujjain,
India: An observational study. BMJ Paediatr Open. 2019;3:e000509.
|
|
|
 |
|