|
|
|
Indian Pediatr 2020;57:808-810 |
 |
Epidemiology and
Clinical Features of Coronavirus Disease 2019 in Moroccan
Children
|
|
K El Fakiri, H Nassih, I Ait Sab, G Draiss and M Bouskraoui
From Department of Pediatrics, Child and Mother Hospital, Mohammed VI
University Hospital Center, Marrakesh Medical and Pharmacy Faculty,
Caddy Ayad University, Marrakesh, Morocco.
Correspondence to: Dr Houda Nassih, Pediatric unit ‘B’, Department of
Pediatrics, Child and Mother Hospital, Mohammed VI University Hospital
Center, Marrakesh Medical and Pharmacy Faculty, Caddy Ayad University,
City of Marrakesh, Morocco. [email protected]
Received: May 14, 2020;
Initial review: June 19, 2020;
Accepted: July 03, 2020
Published online: July 12, 2020; PII: S097475591600207
|
Objectives: This study aims to analyze the epidemiological and
clinical features of coronavirus disease 19 (COVID-19) in a Moroccan
pediatric population. Methods: A retrospective study of a cohort
of 74 children with RT-PCR confirmed COVID-19. We collected information
on clinical and laboratory features of all children (age <18 years)
admitted between 2 March, 2020 and 1 April, 2020. Results: The
mean (SD) age of the 74 children (40 girls) was 7 (1.5) years. The mean
(SD) time from illness onset to diagnosis was 2 (1) days. 54 children
were asymptomatic, while eight had fever, and five cases had cough.
Recovery was after a mean (SD) of 12 (1) days. Conclusions:
COVID-19 was mostly mild in the pediatric population in Morocco.
Keywords: Outcome, Pandemic, RT-PCR, SARS-CoV-2.
|
|
E
mergence of coronavirus disease 2019
(COVID-19) has attracted global attention, and the WHO has
declared the severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) infection as a pandemic. As of May 25, 2020, a
total of 7756 cases, which 9% of them are children, occurred in
Morocco [1]. Worldwide, it has been reported that the disease is
mostly asymptomatic, or mild-moderate in nature in children
[2-4]. To date, not much information is available about COVID-19
in Moroccan pediatric population. Our study aims to detail
clinical features and outcome in Moroccan children infected with
SARS-CoV-2 virus.
METHODS
We retrospectively reviewed records of 74
children confirmed with SARS-COV-2, who were managed in Mohammad
VI university hospital of Marrakesh from March 2, 2020, to April
1, 2020. The ethics committee of our hospital approved this
study. COVID-19 pediatric cases were defined as follows:
Possible case: when a history of contact with a confirmed case
of SARS-COV-2, and/or an acute respiratory infection of unknown
etiology are present; and confirmation of infection was obtained
from all patients at admission by detection of SARS-COV-2
nucleic acid on nasopharyngeal swab specimens using RT-PCR.
All confirmed COVID-19 cases <18 years were
included except from newborns. Parents or guardians of all
participants provided informed consent enrolled in this study.
We collected data regarding epidemiological, demographical,
clinical symptoms, laboratory measure-ments, imaging findings,
management, and outcome. Laboratory workup carried out in all
patients at diagnosis included complete blood count, CRP,
procalcitonin, urea, creatinine, AST, ALT, PTT, aPTT, D-Dimer,
ferritin, LDH, CPK, fibrinogen, and serum electrolytes. Computed
tomography (CT) scan was done in those with severe
manifestations. Patients were classified as follows:
Asymptomatic infection (children without manifestations of
clinical symptoms of COVID-19 testing positive to SARS-COV-2);
Acute upper respiratory tract infection (children with fever,
cough, pharyngeal pain, nasal congestion, fatigue, headache,
myalgia or discomfort, and without signs of pneumonia by chest
imaging or sepsis); Mild pneumonia (when children have a fever,
respiratory symptoms such as cough, and chest imaging indicating
pneumonia, but not reaching the criteria of severe pneumonia);
Severe pneumonia (when any of the following criteria are
present: (i) increased respiratory rate:
³60
breaths/min (<2 years), ³40
breaths/min (between 2 and 5 years),
³30
breaths/min (³5
years); (ii) oxygen saturation <94%; (iii)
hypoxia; (iv) disturbance of consciousness; and, (v)
food refusal or feeding difficulty, with signs of dehydration);
and, Critical cases (who meet any of the following criteria and
require ICU care: respiratory failure requiring mechanical
ventilation, shock, or with other organ failure).
Treatment was prescribed according to the
Moroccan Ministry of Health recommendations [5]. RT-PCR tests
were done on the ninth, 14th, 21st, and 28th days from
diagnosis. Recovery was declared when there was clinical
improvement, child was afebrile for more than three days, and at
least one negative RT-PCR result was obtained. All statistical
data were processed using the Excel professional 2016 software.
RESULTS
Out of 74 children with confirmed COVID-19
included in our study, 34 (46%) were boys. The median age was 7
years (range, 2 month – 17 year). Medical history was marked by
two cases of mild intermittent asthma, one case of type 1
diabetes, one case of epilepsy, and one case of Down syndrome
with intraventricular shunt. All the cases exhibited familial
aggregation and had a history of close contact with their adult
relatives who were diagnosed with COVID-19, except for one child
who contacted the disease from a housemaid, and a second one who
contacted from a neighbor. All our patients had satisfactory
nutritional state, as well as normal growth parameters.
 |
|
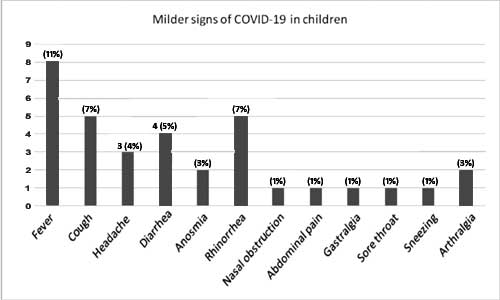
Fig. 1 Symptoms in children
with confirmed COVID-19.
|
Fifty-four (73%) children were asymptomatic.
The remaining twenty patients had mild symptoms (Fig.
1), mainly symptoms of flu, with a mean (SD) time from
illness onset to diagnoses of 2 (0.5) days. Most frequent signs
were fever (10.8%), cough (6.7%), rhinorrhea (6.7%), and
diarrhea (5.4%). Hematological abnormalities were marked by
lymphocytosis in 8% of cases, while the rest were characterized
by high creatinine phosphokinase (CPK), lactate dehydrogenase
(LDH), and mild hepatic transaminitis (<1.5 times normal) (Table
I).
Table I Laboratory Abnormalities in Pediatric Patients with Coronavirus Disease-2019 in Morocco (N=74)
|
Laboratory test |
Number (%) |
|
Complete blood count |
|
|
Anemia |
4(5) |
|
Hyperleucocytosis |
2(3) |
|
Leucopenia |
1(1) |
|
Lymphopenia |
2(3) |
|
Lymphocytosis |
6(8) |
|
AST (³40 IU/L) |
22(30) |
|
ALT (³40 IU/L) |
22(30) |
|
Ferritin (>150 ng/mL) |
2(3) |
|
LDH (>290 IU/L) |
32(43) |
|
CPK (>25 IU/L) |
10(13.5) |
|
Procalcitonin (>0.5 ng/mL) |
9(12) |
|
AST - Aspartate aminotransferase; ALT - alanine
aminotransferase; LDH - lactic dehydrogenase; CPK -
creatinine phosphokinase. |
Management consisted of supportive care:
hydration, antipyretics and nutritional support. The 15-year-old
girl was started on chloroquine 5 mg/kg/12h for five days (after
documenting a normal electrocardiogram) with azithromycin (10
mg/kg the first day; then 5 mg/kg/day for five days) along with
vitamin C (1g twice a day for ten days) and zinc (90 mg twice a
day for ten days). By the third day, evolution was marked by
severe side effects (diplopia, nausea, epigastric pain), when we
switched to hydroxychloroquine (5 mg/kg/12h to complete a total
of ten days). Subsequently, improvement was noted and no new
side effects were seen. Breastfeeding was maintained in a
two-months-old infant while respecting airborne and contact
protection measures. No case was hospitalized in the intensive
care unit or needed respiratory assistance. No patient died.
Resolution of symptoms occurred by the
seventh day in most (80%) cases. The average (SD) hospital stay
was of 13 (3) days (range, 10-21 days). Negative RT-PCR results
were obtained after a mean (SD) time of 14 (2) days (50% by
ninth day, 75% by the 14th day, 94% by the 21st day), while four
cases remained positive until the 28th day.
DISCUSSION
In Morocco, till date, approximately 600
children have been affected with COVID-19. Marrakesh is at the
heart of the epidemic, with 19% of nationwide cases. All the
pediatric cases are admitted to our center. Retrospective study
of these cases found that our series agrees with those
previously published, suggesting that most pediatric COVID-19
cases are females [6]. Children of all ages were susceptible to
COVID-19 similar to other studies [7,8]. The most affected
proportion of children were aged between 10 and 14 years, with a
mean age similar to a Korean report [9], while a Spanish series
found that most affected children were younger [6]. A Chinese
series reported that over 90% of children were either
asymptomatic or with mild-moderate manifestations [4]. The
majority of our cases were asymptomatic because these infections
were recognized mostly through contact tracing. Median time
from illness onset to diagnosis was similar to the Chinese
series [4]. All the symptomatic cases were upper respiratory
infections, while other series found more severe cases [9-11].
Lymphopenia has been reported in COVID-19 previously also [9],
and was seen in 3% of our children.
The Moroccan ministry of health approved in
early April, 2020, a nationwide protocol using chloroquine or
hydroxychloroquine associated with azithromycin in all COVID-19
severe pediatric cases [5]. We used this protocol in only one
case with an immunocompromized condition (type 1 diabetes).
Finally, we were well aware of the impact of the psychological
state on the well-being of our children, so as recommended by
Massimo, et al., [12], we organized various activities
such as anniversary parties, as well as providing hospitalized
children with toys and books to alleviate loneliness.
In conclusion, COVID-19 in Moroccan children
seems to be mild, with non-specific clinical and biological
findings, and with a rare need of specific treatment. Other
studies are necessary to verify these findings from this
preliminary report.
Ethics Clearance: Ethics Committee of
Mohammed VI University Hospital Center of Marrakesh, Morocco;
No. SD269815/20 dated May 02, 2020.
Contributors: KF: concept and designed
the study, analyzed data and drafted the manuscript; HN: helped
in data analysis and writing; GD, MB, IS: supervised data
analysis. All authors approved the final manuscript.
Funding: None; Competing interest:
None stated.
| |
|
What This Study Adds?
•
Our study describes the
North African experience with COVID-19 in children.
|
REFERENCES
1. The Official Coronavirus Portal in Morocco
[Internet]. Available from:
http://www.covidmaroc.ma/pages/Accueil.aspx. Accessed May
12, 2020.
2. Wu Z, McGoogan JM. Characteristics of and
important lessons from the coronavirus disease 2019 (COVID-19)
outbreak in China: Summary of a report of 72 314 cases from the
Chinese Center for Disease Control and Prevention. JAMA.
2020;323:1239-42.
3. Balasubramanian S, Rao NM, Goenka A,
Roderick M, Ramanan AV. Coronavirus disease 2019 (covid-19) in
children - What we know so far and what we do not. Indian
Pediatr. 2020;57:435-42.
4. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang
Z, et al. Epidemiology of COVID-19 among children in
China. Pediatrics. 2020;e20200702.
5. Moroccan Ministry of health
recommendations for the therapeutic management of confirmed
COVID-19 cases [Internet]. Available from:
http://www.covidmaroc.ma/Documents/2020/coronavirus/PS/Covid-19Prise
%20en% 20charge%20th%C3%A9rapeutique%20des%20cas%20
confirm%C3%A9s%20(23mars2020).pdf. Accessed May 23,
2020.
6. Tagarro A, Epalza C, Santos M,
Sanz-Santaeufemia FJ, Otheo E, Moraleda C, et al.
Screening and severity of coronavirus disease 2019 (COVID-19) in
children in Madrid, Spain. JAMA Pediatr [Internet]. Available
from: https://jamanetwork.com/journals/jamapediatrics/full
article/276439. Accessed May 27, 2020.
7. Wei Xia , Jianbo Shao, Yu Guo, Xuehua Peng
, Zhen Li , Daoyu Hu . Clinical and CT features in pediatric
patients with COVID 19 infection: Different points from adults.
Pediatr Pulmonol. 2020;55:1169-74.
8. Choi S-H, Kim HW, Kang J-M, Kim DH, Cho
EY. Epidemiology and clinical features of coronavirus disease
2019 in children. Clin Exp Pediatr. 2020;63:125-32.
9. Liu W, Zhang Q, Chen J, Xiang R, Song H,
Shu S, et al. Detection of COVID-19 in children in early
January 2020 in Wuhan, China. N Engl Med. 2020;382:1370-1.
10. Wang D, Ju XL, Xie F, Lu Y, Li FY, Huang
HH, et al. Clinical analysis of 31 cases of 2019 novel
coronavirus infection in children from six provinces (autonomous
region) of northern China. Zhonghua Er Ke Za Zhi. 2020;58:E011.
11. Feng K, Yun YX, Wang XF, Yang GD, Zheng
YJ, Lin CM, et al. Analysis of CT features of 15 children
with 2019 novel coronavirus infection. Zhonghua Er Ke Za Zhi.
2020;58:275-8.
12. Pettoello-Mantovani M, Pop TL, Mestrovic
J, Ferrara P, Giardino I, Carrasco-Sanz A, et al.
Fostering resilience in children: The essential role of
healthcare professionals and families. J Pediatr.
2019;205:298-99.e1.
|
|
|
 |
|
