|
|
|
Indian Pediatr 2020;57: 795-797 |
 |
Correlation of Aortic Intima-Media Thickness
With Birthweight in Healthy Term and Near Term Neonates
|
Ranganatha Ashok Devaranavadagi 1,
Vijay Halagappanavar Vamadevappa2
and Girish Gururaja1
From Departments of 1Pediatrics and 2Radiology,
Apollo BGS hospital, Mysore, Karnataka, India.
Correspondence to: Dr Girish Gururaja, Consultant
Neonatologist, Apollo BGS hospital, Adichunchanagiri road,
Kuvempunagar, Mysore, Karnataka 570 023, India.
Email: [email protected]
Submitted: August 19, 2019;
Initial review: November 14, 2019;
Accepted: March 14, 2020.
Published online: June 12, 2020.
PII: S097475591600201
|
Objectives:
The
primary objective was to correlate aortic intima-media
thickness (aIMT) measured at L1-L2 with birth weight in
neonates born at ³35
week of gestation. The secondary objective was to compare
aIMT in small for gestational age (SGA) and appropriate for
gestational age (AGA) babies in this cohort. Methods:
Prospective observational study enrolling 200 newborns. aIMT
was measured on day 3 of life using 10-12 MHz ultrasound
probe. Relevant maternal and baby details were collected and
analyzed. Results: Mean (SD) aIMT was 0.43 (0.15) mm.
There was a negative correlation between aIMT and
birthweight (r= -0.64). Mean (SD) aIMT in AGA was
significantly lesser than in SGA babies (0.36 (0.11) vs.
0.64 (0.08) mm; P<0.0001). Conclusion: aIMT
progressively decreases with increase in birthweight.
Keywords: Atherosclerosis, Barker hypothesis,
Outcome, Small for gestational age.
|
M
ost of adult onset cardiovascular
diseases and stroke are end result of atherosclerosis;
which, contrary to prior belief, begins during fetal life
itself [1,2]. The first atherosclerotic lesion begins in the
abdominal aorta [3]. Ultrasound based measurement of aortic
intima-media thickness (aIMT) is a feasible and accurate
marker of atherosclerotic risk [4,5]. Studies in developed
countries have demonstrated a difference in aIMT between
small for gestational age (SGA) and appropriate for
gestational age (AGA) babies but absolute aIMT values are
conflicting [6-8]. There is a paucity of data on normative
values of aIMT in various birthweight cohorts and data on
aIMT values in SGA and AGA babies in Indian population. We
conducted this study to correlate aIMT with birthweight in
term and near-term babies and compared its value between AGA
and SGA babies.
METHODS
This prospective study was conducted at
Apollo BGS Hospital, Mysore from December, 2017 to November,
2018, after clearance from institutional ethics committee.
After informed parental consent, babies of 35 to 41 weeks
gestation were included in this study. Babies with
congenital anomalies and babies who were discharged within
two days of birth were excluded. Pre-pregnancy weight of
mother was obtained from antenatal card. Mother’s weight at
the time of delivery was recorded using standard electronic
weighing machine, and weight gain during pregnancy was
calculated. Gestational age was calculated from last
menstrual date, if not known, dating scan during first
trimester or modified New Ballard scoring of neonates was
used to ascertain gestational age. Birthweight was measured
using a calibrated electronic weighing machine, and length
was measured with an infantometer using standard methodology
[9].
Intergrowth-21 charts were used to plot
anthropometric details of the baby [10]. Ultrasound
examination was done for all the enrolled babies on day 3 of
life to measure aortic intima-media thickness. All the
ultrasound scans were carried out by a single radiologist
who was blinded to birthweight and weight group of the baby.
High resolution B mode measurement was performed using
linear high-resolution probe of 10-12 MHz at L1-L2 i.e.
supra renal aorta using Philips HD 11xe ultrasound system (Koninklijke
Philips NV). Intima-media thickness was defined as distance
from the leading edge of first echogenic line to the second
line. The first line represents lumen-intima interface, and
second line represents collagen containing upper layer of
the adventitia. The image was focused on the dorsal wall of
the aorta, and a gain setting was used to optimize image
quality.
Statistical analyses: All the data
were entered in a Microsoft excel sheet and analyzed using
SPSS 22.0. Pearson correlation coefficient was calculated
for continuous variables and ANOVA was used to compare aIMT
across different birthweight categories. All the tests of
significance were carried out at 5% level of significance.
RESULTS
A total of 200 (94 females) babies were
enrolled in the study. Mean (SD) pre-pregnancy weight of the
mothers was 55.32 (7.05) kg, mean (SD) height was 158 (4.67)
cm and mean (SD) weight gain during pregnancy was 14.12
(2.62) kg. The mean (SD) birth weight of enrolled babies was
2.79 (0.60) kg, mean (SD) length was 48.75 (2.76) cm and
mean (SD) head circumference was 33.03 (1.47) cm.
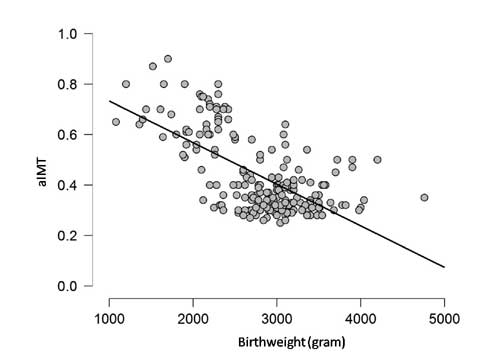
The mean (SD) aIMT observed in our study
was 0.43 (0.15) mm. aIMT showed a negative correlation with
birthweight and length of the baby with correlation
coefficient (r) of –0.64 and –0.61 (Fig. 1).
However, there was a poor correlation of aIMT with
gestational age (r= –0.31), maternal weight (r=
–0.03), maternal height (r = –0.12) and weight gain
during pregnancy (r= –0.29). There was no significant
difference in mean (SD) aIMT in male and female babies [0.45
(0.16) and 0.43 (0.14)].
 |
|
Fig. 1 Scatter diagram of
correlation of aortic intima-media thickness (aIMT)
|
Value of aIMT was significantly more in
SGA babies than their AGA counterparts (Table I).
For every given gestation, SGA babies had significantly
higher aIMT than AGA babies (Table II).
Table I Aortic Intima-Media Thickness in Different Birthweight Groups (N=200)
|
AGA |
SGA |
LGA
|
|
(n=136) |
(n=54) |
(n=10) |
|
Birthweight, kg |
2.99 (0.35) |
2.07 (0.36) |
3.91 (0.37) |
|
Gestational age, wk |
38.2 (1.3) |
37.3 (1.5) |
38.9 (1.1) |
|
aIMT,* mm |
0.36 (0.08)
|
0.64 (0.11)
|
0.36 (0.08) |
|
Values in mean (SD); aIMT: aortic intima media
thickness; *P<0.001; AGA: appropriate for
gestational age; SGA: small for gestational age;
LGA: large for gestational age. |
Table II Aortic Intima-Media Thickness among Infants With Different Gestational Age (N=200)
|
Aortic intima-media thickness, mm |
|
Gestational age |
|
AGA* |
|
SGA |
|
n |
mean (SD) |
n |
mean (SD) |
|
35-36 wk |
16 |
0.41 (0.13) |
17 |
0.66 (0.11) |
|
37-38 wk |
59 |
0.35 (0.07) |
23 |
0.64 (0.12) |
|
39-40 wk |
61 |
0.36 (0.08) |
14 |
0.62 (0.1) |
|
AGA: appropriate for gestational age; SGA: small
for gestational age; P<0.001 for aortic intima-media
thickness between SGA and AGA babies in different
gestational age groups; *P=0.03 for comparison
between different gestational age groups among AGA
babies. |
DISCUSSION
In this study, we enrolled 200 healthy
neonates of 35-41 weeks of gestation and aIMT was measured
on dorsal wall of aorta between L1-L2, and this was
correlated with birth weight. aIMT was higher in babies with
lower birth weight irrespective of gestational age. Similar
correlation was found between length and aIMT. SGA babies in
our study had significantly higher aIMT than their AGA
counterparts. Mean aIMT value was fairly static across
gestation age of 35-41 weeks within SGA and AGA categories.
We had a relatively large sample size,
and all the aIMT measurements were done by a single
radiologist blinded to birthweight cohort, hence eliminating
the possibility of any inter observer variation. However, we
did not look into risk factors for SGA and possible
differential effect of these risk factors on aIMT.
Our value of mean aIMT of 0.44 mm is
comparable to the data reported from India [11,12]. AGA
babies in our study had a mean aIMT of 0.36 mm which is
lower compared to most of other reported values, and SGA
babies had a mean aIMT of 0.64 mm which is higher than most
other values reported from the Western population [1,6,7].
This difference could be either due to racial variation, or
due to different nutritional and medical illness profile in
Indian mothers.
Even though, aIMT has been investigated
in newborn period, the natural history of these lesions and
possible reversibility of these lesions has never been
evaluated. Long term follow up of these babies for
confirming evolution of these lesions into atherosclerotic
plaques is needed.
Ethical clearance:
Institutional ethics committee, Apollo BGS hospital;
No. 11/2018. April 21, 2018.
Contributors: RD, VV, GG:
formulated the study, drafted the protocol and involved in
final writing of the article; RD, GG: collected and analyzed
the data; VV: did the sonographic measurement of all cases.
Funding: None; Competing interest:
None stated.
|
WHAT THIS STUDY ADDS?
A negative correlation exists
between birthweight and aortic intima-media
thickness, with small for gestational age babies
exhibiting higher values than appropriate for
gestational age counterparts
|
REFERENCES
1. Gomez-Roig MD, Mazarico E, Valladares
E, Guirado L, Fernandez-Arias M, Vela A. Aortic intima-media
thickness and aortic diameter in small for gestational age
and growth restricted fetuses. PLoS One. 2015:10: e0126842.
2. Barker DJ, Eriksson JG, Forsen T,
Osmond C. Fetal origins of adult disease: Strength of
effects and biological basis. Int J Epidemiol.
2002;31:1235-9.
3. Zanardo V, Fanelli T, Weiner G, Fanos
V, Zaninotto M, Visentin S, Cosmi E. Intrauterine growth
restriction is associated with persistent aortic wall
thickening and glomerular proteinuria during infancy. Kidney
Int. 2011;80: 119-23.
4. McCloskey K, Vuillermin P, Ponsonby
AL, Cheung M, Skilton MR, Burgner D. Aortic intima-media
thickness measured by trans-abdominal ultrasound as an early
life marker of subclinical atherosclerosis. Acta
Paediatr.2014; 103:124-30.
5. Dorota Szostak Wegierek, Katarzyna
Szamotulska, Arkadiusz Maj, Relationship between carotid
intima media thickness, atherosclerosis risk factors and
birth weight in young males. Kardiol Pol 2011;69:673-8.
6. Stergiotou F, Crispi B, Valenzuela-Alcaraz
M, Cruz-Lemini B, Bijnens, Gratacos E. Aortic and carotid
intima-media thickness in term Small-for-gestational-age
newborns and relationship with prenatal signs of severity.
Ultrasound Obstet Gynecol. 2014;43:625-31.
7. Skilton MR, Evans N, Griffiths KS,
Harmer J, Celermajer DS. Aortic wall thickness in newborns
with intrauterine growth restriction. Lancet. 2005;
365:1484-86.
8. Alfarizi AB, Nova R, Tasli JM,
Theodorus. Relationship between small for gestational age
and aortic intima-media thickness in newborns. Paediatr
Indones. 2014;54:57-1.
9. Cheikh Ismail L, Puglia FA, Ohuma EO,
Ash ST, Bishop DC, Carew RM, et al. Precision of
recumbent crown-heel length when using an infantometer. BMC
Pediatr. 2016 16:186.
10. Stirnemann J, Villar J, Salomon LJ,
Ohuma E, Ruyan P, Altman DG, et al. International
estimated fetal weight standards of the Intergrowth-21st
project. Ultrasound Obstet Gynecol. 2017;49:478-486.
11. Hondappanavar A, Sodhi KS, Dutta S,
Saxena AK, Khandelwal N. Quantitative ultrasound measurement
of intima-media thickness of abdominal aorta and common
carotid arteries in normal term newborns. Pediatr Cardiol.
2013;34:364-9.
12. Sodhi KS, Hondappanavar A, Saxena AK, Dutta S,
Khandelwal N. Intima-media complex thickness: Preliminary
workup of comparative evaluation of abdominal aorta and
carotid artery of small-for-gestation-age term newborns and
normal size term newborns. Acta Cardiol. 2015;70:351-7.
|
|
|
 |
|
