We read with interest the article by Mahajan, et al. [1] on the
use of telemedicine during the severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) pandemic. The authors have well summarized
the pros and cons of tele-health service. We would like to share our
experience with telemedicine used with forward triaging that helps
mitigate some of its major limitations and protects healthcare workers
(HCWs) from potential exposure.
The guidelines for telemedicine have been eased to
enable continued care of non-COVID illnesses [2]. However, it is the
chronic illnesses that require holistic care by an entire team,which
have taken a backseat in the current scenario. Telehealth needs to be
part of routine practice, and not just during emergencies [3]. This
focuses on creating a more sustainable model of care, and a telehealth-ready
workforce, incorporating telemedicine training even in the medical
curriculum [3].While many countries are using telemedicine to triage
COVID suspects, we planned to develop it into a system of care even in
the post-pandemic phase [4,5].
Following our initial experience with use of
telephonic consults, a new platform that incorporated telemedicine into
the existing Hospital Information system (HIS) was launched on 8 June,
2020. A teleconsultation was provided as per schedule, once a
telemedicine appointment was taken by the patient, using a simple
feature phone, any video calls or images are shared through WhatsApp
(Business). Referral to other specialties was also possible to ensure
comprehensive care. The prescription was sent to the patient as a PDF
document. After a telemedicine consultation, in case the physician felt
the need of an in-person visit, the same is again indicated in the
online system and patient is allowed physical entry into the OPD after
screening on the appointed date and time.
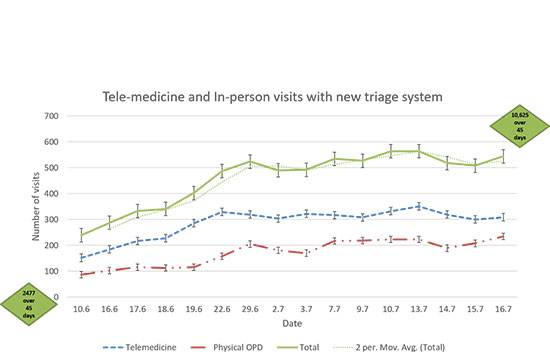
In our hospital, telephonic-only consults were
provided to 2477 patients over a period of 45 days (21 April to 7 June,
2020) while the new system has enabled provision of care to 10,625
patients over the same time span (8 June to 16 July, 2020) (Fig.
1). Physical consultations constituted only 29% of the consultations
in this period. This also reflects the proportionate reduction in
exposure of healthcare staff to potential SARS-CoV-2 carriers.
 |
|
Fig. 1 Line diagram showing the
number of patients seen through new OPD system. The red
line indicates the number of patients provided in-person visit
after telemedicine triage. The green diamonds shows the number
of patients cared for- 2477 patients were provided tele-consult
before the launch of new platform over 45 days which increased
to more than 10000 patients in next 45 days.
|
The system mitigated the limitation of telemedicine
by allowing physical examination after adequate triaging in selected
patients. Although, rural India is poor in individual digital literacy,
there is a wide network of e-mitra kiosks, ASHA workers and teachers who
have come forward to help navigate the system and move through the
process. The benefit arising out of limited physical visits to the
hospital for patient are already described but restricting the exposure
of doctors and patients to someone who is potentially infected is of
vital importance.
For a major impact to be seen, an operational
telehealth network is required, and infrastructure needs to be scaled
up. It also requires a behavior change of not just an individual or an
institute but an entire health system as well as patients. We have tried
to curtail these limitations and made a beginning while making use of
the COVID-19 crises as an opportunity to introduce the system that will
stay for future.
Acknowledgements: Prof Kuldeep Singh, Dean
Academics and Prof Sanjeev Misra, Director, AIIMS, Jodhpur for
conceptua-lizing the idea and facilitating the development of the
software.
1. Mahajan V, Singh T, Azad C. Using telemedicine
during the COVID-19 pandemic. Indian Pediatr. 2020;57:652-7.
2. Ministry of Health and Family welfare, Government
of India. Telemedicine Practice Guidelines Enabling Registered Medical
Practitioners to Provide Healthcare Using Tele-medicine. New Delhi.
Available at https://www.mohfw.gov. in/pdf/Telemedicine.pdf.
Accessed on April 03, 2020
3. Smith AC, Thomas E, Snoswell CL, et al.
Telehealth for global emergencies: Implications for coronavirus disease
2019 (COVID-19) [published online ahead of print, 2020 Mar 20]. J
Telemed Telecare. 2020;1357633X20916567.
4. Tolone S, Gambardella C, Brusciano L, G del Genio,
Lucido FS, Docimo L. Telephonic triage before surgical ward admission
and telemedicine during COVID-19 outbreak in Italy. Effective and easy
procedures to reduce in-hospital positivity. Int J Surg. 2020; 78:123-25
5. Hollander JE, Carr BG. Virtually perfect? Telemedicine


