A few weeks following the peak of COVID-19 epidemic
in the US and the European Union, a novel systemic illness which
clinically overlaps with Kawasaki disease with or without shock
syndrome, macrophage activation syndrome (MAS) and toxic shock syndrome
(TSS) was reported in children. This entity was labeled as Multisystem
inflammatory syndrome in children (MIS-C) by the Centers for Disease
Control and Prevention (CDC), USA and by the World Health Organization
(WHO) [6,7]. A few cases have also been reported from India [20].
Cardiac involvement as evidenced by perturbation of
cardiac chamber size and/or function, coronary artery abnormalities
(ectasia, aneurysm) or elevated cardiac biomarkers such as troponin or
pro-BNP is not only common in children with MIS-C but can also be severe
(Web Table I). A vast majority of children
with MIS-C had been previously healthy; a few have had minor
comorbidities such as asthma and obesity. In addition to fever and
weakness/malaise, gastrointestinal symptoms have been common at
presentation. Many of these children have had marked hemodynamic
instability requiring inotropic support and intensive care at admission.
In addition, a small proportion has required extracorporeal membrane
oxygenation support; though, mortality has been low [20-27]. In contrast
to patients with typical Kawasaki disease, atypical features including a
higher incidence of cardiac involvement (60%), shock syndrome like
features (50%), MAS (50%) and need for steroids following IVIG
administration (80%) were noted in a previous study [22].
The precise mechanisms that underlie genesis of MIS-C
and its cardiac manifestations are yet unknown. However, given the fact
that a vast majority of children have presented 4-6 weeks after the peak
of the local COVID-19 epidemic, many have been SARS-CoV-2 PCR negative
but antibody positive, have had markedly elevated inflammatory markers
such as C-reactive protein, erythrocyte sedimentation rate, fibrinogen,
procalcitonin, ferritin, or interleukin 6, and have responded well to
IVIG and immunomodulators; an immune origin is likely. Genetic factors
may underlie the overall rarity of MIS-C and relative preponderance in
African Americans.
Given the multiorgan dysfunction and potential for
sudden and severe decompensation in patients with MIS-C, our practice
has been to admit these patients to PICU where they are cared for by a
team which involves specialists from pediatric rheumatology/immunology,
pediatric critical care, pediatric cardiology, pediatric infectious
diseases, and pediatric hematology. Inotropes should be initiated in
children with MIS-C if clinically indicated and ECMO should be reserved
for children with inotrope-refractory shock. In addition to clinical
markers, mixed venous oxygen saturation and plasma lactate can be used
to guide therapy. A vast majority of children with MIS-C have responded
well to IVIG (1-2 g/kg), which as per the recently proposed American
College of Rheumatology guidelines [28] should be the initial
therapeutic agent. Though the data are scarce, patients with suboptimal
clinical response (hemodynamic instability) or biochemical response
(persistent elevation in inflammatory markers) to IVIG have benefitted
from steroids (intravenous methylprednisolone 2 mg/kg/day) or
immunomodulators such as anakinra (interleukin-1 antagonist) (2-8
mg/kg/day subcutaneous injection once or twice a day, maximum dose: 100
mg twice a day) and tocilizumab (interleukin-6 antagonist). The dosing
of tocilizumab for systemic onset juvenile idiopathic arthritis is 12
mg/kg intravenous or 162 mg subcutaneous every other week for those
weighing less than 30 kg and 8 mg/kg intravenous every other week or 162
mg subcutaneous every week for those weighing >30 kg. The optimal dose
and dosing frequency for MIS-C is not known; intravenous doses of
400-800 mg and a subcutaneous dose of 162 mg has been used in adults
with COVID-19 associated cytokine release syndrome [29], and 8 mg/kg in
children [30]. Though adjunctive immune modifying therapies such as
anakinra, tocilizumab and convalescent plasma have been used in patients
with both acute COVID-19 and MIS-C, their role has not been
systematically evaluated. Given the potential risk of thrombotic
complications, we also initiate aspirin and low molecular weight heparin
at admission, both of which we discontinue upon normalization of
inflammatory markers. In addition to aspirin and low molecular weight
heparin, we have typically discharged these patients on oral steroids
which are gradually tapered as guided by their clinical status and
cardiac and inflammatory biomarkers. Cardiac imaging with a focus on
coronary arteries is obtained at regular intervals after discharge [28].
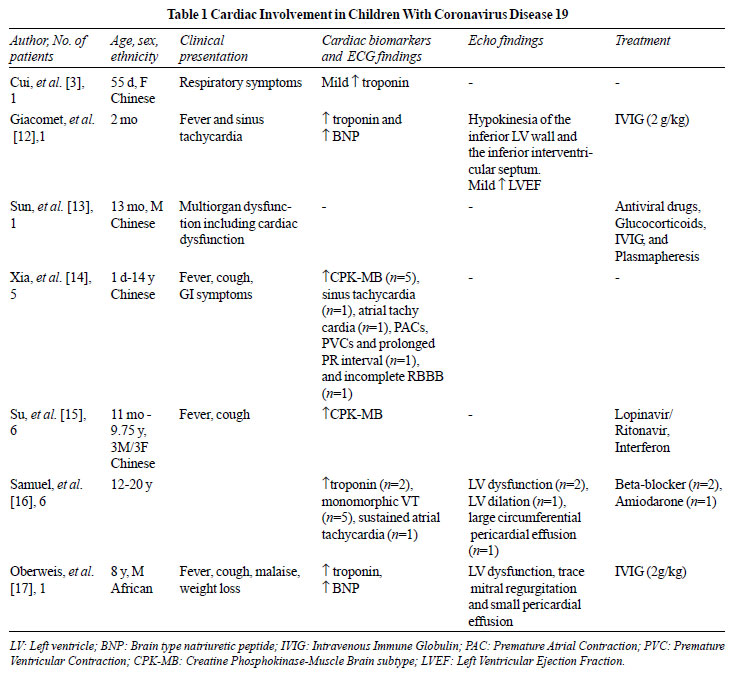
Cardiac involvement in children with COVID-19 is
uncommon; however, a handful of patients have had severe involvement
with markedly diminished ventricular function and hemodynamic
instability. These patients have benefited from IVIG. The role of
antivirals such as remdesivir, hydroxychloroquine, and adjunctive
immunomodulatory therapies in patients with COVID-19 and cardiac
involvement is unclear at this time. Cardiac involvement as evidenced by
perturbation of cardiac chamber size and/or function, coronary artery
abnor-malities (ectasia, aneurysm) or elevated cardiac bio-markers such
as troponin or pro-BNP is not only common in children with MIS-C but can
also be severe. These children have responded to IVIG and or
corticosteroids. A few have required additional immunomodulators such as
anakinra and tocilizumab.
1. Castagnoli R, Votto M, Licari A, Brambilla I,
Bruno R, Perlini S, et al. Severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) infection in children and adolescents: A
Systematic Review [published online ahead of print, 2020 Apr 22]. JAMA
Pediatr. 2020;10.1001/jamapediatrics.2020.1467.
2. Ludvigsson JF. Systematic review of COVID-19 in
children shows milder cases and a better prognosis than adults. Acta
Paediatr. 2020;109:1088-95.
3. Cui Y, Tian M, Huang D, Wang X, Huang Y, Fan Li,
et al. A 55-day-old female infant infected with 2019 novel
coronavirus disease: Presenting with pneumonia, liver injury, and heart
damage. J Infect Dis. 2020;221:1775-81.
4. Shekerdemian LS, Mahmood NR, Wolfe KK, Riggs BJ,
Ross CE, McKiernan CA, et al. Characteristics and outcomes of
children with coronavirus disease 2019 (COVID-19) infection admitted to
US and Canadian pediatric intensive care units [published online ahead
of print, 2020 May 11]. JAMA Pediatr.
2020;10.1001/jamapediatrics.2020.1948.
5. Gefen AM, Palumbo N, Nathan SK, Singer PS,
Castellanos-Reyes LJ, Sethna CB. Pediatric COVID-19-associated
rhabdomyolysis: A case report. Pediatr Nephrol. 2020;35:1517-20.
6. Centers for Disease Control and Prevention.
Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with
Coronavirus Disease 2019 (COVID-19). Available from:
https://emergency.cdc.gov/han/2020/han00432.asp. Accessed May 29,
2020
7. World Health Organization. Multisystem
inflammatory syndrome in children and adolescents temporally related to
COVID-19 Available from: https://www.who.int/news-
room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19.
Accessed May 29, 2020
8. Bansal M. Cardiovascular disease and COVID-19.
Diabetes Metab Syndr. 2020;14:247-50.
9. Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M,
Tomasoni D, et al. Cardiac involvement in a patient with
coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5:1-6.
10. Shi S, Qin M, Shen B, Cai Y, Liu T, Yang F, et
al. Association of cardiac injury with mortality in hospitalized
patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020;5:802-10.
11. Akhmerov A, Marbán E. COVID-19 and the heart.
Circ Res. 2020;126:1443 55.
12. Giacomet V, Manfredini VA, Meraviglia G, Peri CF,
Sala A, Longoni E, et al. Acute inflammation and elevated cardiac
markers in a two-month-old infant with severe acute respiratory syndrome
coronavirus 2 infection presenting with cardiac symptoms. Pediatr Infect
Dis J. 2020;39:e149-51.
13. Sun D, Li H, Lu XX, Xiao H, Ren J, Zhang F, et
al. Clinical features of severe pediatric patients with coronavirus
disease 2019 in Wuhan: A single centers observational study. World J
Pediatr. 2020;16:251-9.
14. Xia W, Shao J, Guo Y, Peng X, Li Z, Hu D.
Clinical and CT features in pediatric patients with COVID-19 infection:
Different points from adults. Pediatr Pulmonol. 2020; 55:1169 74.
15. Su L, Ma X, Yu H, Zhang Z, Bian P, Han Y, et
al. The different clinical characteristics of corona virus disease
cases between children and their families in China - the character of
children with COVID-19. Emerg Microbes Infect. 2020;9:707-13.
16. Samuel S, Friedman RA, Sharma C, Ganigara M,
Mitchell E, Schleien C, et al. Incidence of arrhythmias and
electro-cardiographic abnormalities in symptomatic pediatric patients
with PCR positive SARS-CoV-2 infection including drug induced changes in
the corrected QT interval (QTc). Heart Rhythm. 2020;S1547-5271: 30632-9.
17. Oberweis ML, Codreanu A, Boehm W, Olivier D,
Pierron C, Tsobo C, et al. Pediatric Life-threatening coronavirus
disease 2019 with myocarditis. Pediatr Infect Dis J. 2020;39:e147-e149.
18. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et
al. Epidemiology of COVID-19 among children in China. Pediatrics.
2020;e20200702.
19. Sanna G, Serrau G, Bassareo PP, Neroni P, Fanos
V, Marcialis MA. Children’s heart and COVID-19: Up-to-date evidence in
the form of a systematic review. Eur J Pediatr. 2020;179:1079-87.
20. Dhanalakshmi K, Venkataraman A, Balasubramanian
S, Madhusudan M, Amperayani S, Putilibai S, et al.
Epidemiological and clinical profile of pediatric inflammatory
multisystem syndrome - temporally associated with SARS-CoV-2 (PIMS-TS)
in Indian children [published online ahead of print, 2020 Aug 6]. Indian
Pediatr. 2020; S097475591600220.
21. Belhadjer Z, Méot M, Bajolle F, Khraiche D,
Legendre A, Abakka S, et al. Acute heart failure in multisystem
inflammatory syndrome in children (MIS-C) in the context of global
SARS-CoV-2 pandemic [published online ahead of print, 2020 May 17].
Circulation. 2020;10.1161/CIRCULATIONAHA.120.048360.
22. Verdoni L, Mazza A, Gervasoni A, Martelli L,
Ruggeri M, Ciuffreda M, et al. An outbreak of severe
Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2
epidemic: An observational cohort study. Lancet. 2020;395:1771-78.
23. Riphagen S, Gomez X, Gonzalez-Martinez C,
Wilkinson N, Theocharis P. Hyper inflammatory shock in children during
COVID-19 pandemic. Lancet. 2020;395:1607-8.
24. Chiotos K, Bassiri H, Behrens EM, Blatz AM, Chang
J, Diorio C, et al. Multisystem inflammatory syndrome in children
during the COVID-19 pandemic: A case series. J Pediatric Infect Dis Soc.
2020;9:393-8.
25. Feldstein LR, Rose EB, Horwitz SM, Collins JP,
Newhams MM, Son MBF, et al. Multisystem inflammatory syndrome in
U.S. children and adolescents. N Engl J Med. 2020;383:334-46.
26. Dufort EM, Koumans EH, Chow EJ, Rosenthal EM,
Muse A, Rawlands J, et al. Multisystem inflammatory syndrome in
children in New York State. N Engl J Med. 2020;383:347-58.
27. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones
CE, Shah P, et al. Clinical Characteristics of 58 Children With a
Pediatric Inflammatory Multisystem Syndrome Temporally Associated With
SARS-CoV-2 [published online ahead of print, 2020 Jun 8]. JAMA.
2020;e2010369.
28. American College of Rheumatology. Clinical
Guidance for Pediatric Patients with Multisystem Inflammatory Syndrome
in Children (MIS-C) Associated with SARS-CoV-2 and Hyperinflammation in
COVID-19. Available from: https://www.rheumatology.org/
Portals/0/Files/ACR-COVID-19-Clinical-Guidance-Summary-MIS-C-Hyperinflammation
.pdf. Accessed August 7, 2020.
29. Hassoun A, Thottacherry ED, Muklewicz J, Aziz QU,
Edwards J. Utilizing tocilizumab for the treatment of cytokine release
syndrome in COVID-19. J Clin Virol. 2020;128:104443.
30. Balasubramanian S, Nagendran TM, Ramachandran B,
Ramanan AV. Hyper-inflammatory syndrome in a child with COVID-19 treated
successfully with intravenous immunoglobulin and tocilizumab. Indian
Pediatr. 2020;57:681-3.