This year has been a year of firsts for the Indian Academy of
Pediatrics (IAP). It started two years ago, when you all elected
me as the President elect of our mother organization IAP,
unopposed – first time in the history of IAP in last four
decades. This shows the faith and affection you all have for me,
and honestly, that has left me greatly humbled. It motivated me
to go the extra mile to achieve the best for our mother
organization IAP. I had a vision which would change the way that
our medical fraternity works, and benefit our many fellow
pediatricians who are generally practicing in the remote
locations and rural areas. The dIAP platform – a technology
driven academy – was established for the first time. With dIAP
we reached the unreached, taking whatever the IAP has to offer
to every corner of our country and beyond.
None of us were prepared
for what happened next. COVID-19 struck – an epidemic of global
proportions! Before the financial year ended, India was forced
into a lock-down situation. Academics became a secondary
require-ment – survival was of utmost importance. We, the
Doctors and the healthcare industry started working overtime,
trying to prevent the spread and find a cure, to help people
survive. This was the time for IAP to come to the rescue of
members and community to continue its academics, social and
community activities. No one knew what to do. Desperate times
called for desperate measures. We had to start thinking of
different ways and so called ‘new norms’. Physical distancing,
the necessity to use masks, and avoidance of close contact led
many to search for ‘work from home’ options. Likewise, students
in various disciplines are being taught by dedicated teachers
using the online platform. Medical students, both undergraduates
and postgraduates are allowed limited or no bedside learning
time to avoid unnecessary exposure. Apart from the routine work
done by postgraduates in wards, where they learn practical
skills, formal teaching activity has mainly remained restricted.
Grand rounds, combined teaching from faculty, and bedside case
presentations have come to a halt. Seminars with PowerPoint
presentations involving large gathe-rings in the departments
have also been suspended.
Worldwide, it has been recognized that while it is important to
provide patient care, it is also necessary to ensure adequate
training and teaching of medical students who are future
physicians. But the logical and practical concerns of patient
safety remain, as these students may act as asymptomatic
carriers of SARS-CoV-2 (Severe acute respiratory syndrome –
Coronavirus 2). Technology has come to our rescue to continue
edu-cation through the digital platform. Medical education has
transformed through the use of online media for virtual team
meetings, clinical skills learning, and even for conducting
examinations. Many medical colleges have converted their usual
classroom teaching to the e-learning platform using various
applications available for online classes and webinars. As most
of the teaching hospitals cater to a massive burden of patients
and most of the teaching staff is involved in clinical work, it
allows them lesser time to dedicate for teaching. Also, the
senior faculty is actively involved in administrative issues
like ensuring preparedness for managing the pandemic efficiently
on a large scale.
Keeping these points in mind, the Indian Academy of Pediatrics
has rightly introduced digital lectures, by the name of
Digital-IAP (dIAP), to facilitate e-learning in all spheres of
pediatrics. The dIAP team was already working quite hard. As the
pandemic spread, they needed to pull up their socks and ensure
that they could deliver well before the expected timeline. I am
happy to say that IAP was amongst the first organizations to
start the webinar concept on such a large scale. It was and
still is hugely popular. People across the country have started
viewing and absorbing the knowledge shared in these webinars.
Knowledge was not only limited to COVID-19 and other academic
topics, but rather a holistic approach was taken to ensure the
best interests of our members requirements like teleconsultation
solution, health and death insurance, medicolegal support,
COVID-19 guidelines, connecting with government, charitable and
social responsibilities, and so on. These sessions are being
conducted daily, including topics from all sub-specialties and
cover the curriculum of postgraduate teaching. dIAP is freely
accessible to all, and daily reminders are sent to IAP members
via social media and registered email IDs. Apart from live
streaming, an option to view the recorded version has been made
available in the archives. Webcast attendees may actively
participate in these sessions, ask queries, and share opinions
using the chat box or direct communication in personal meetings.
IAP has conducted 422 online sessions from March 16, 2020 to
August 31, 2020, with an overwhelming response in each of these
sessions from all over India (Fig. 1).
Twenty-three (5%) sessions were conducted during the morning
hours (9 AM to 12 PM), 278 (66%) sessions in the afternoon (1 PM
to 4 PM), and 121 (29%) sessions in the evening (4 PM onwards).
A total of 7,71,375 views with an average of 1886 views per
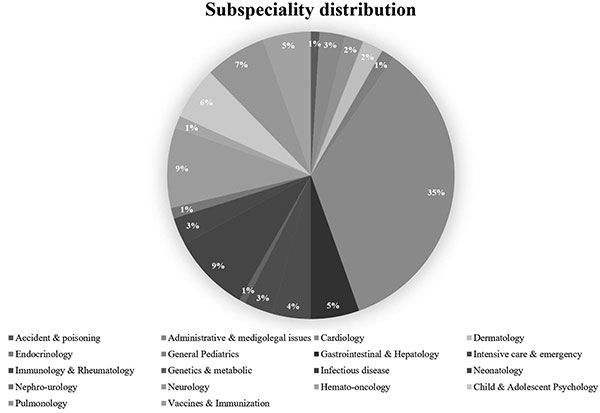
session have been documented. The specialty-wise distribution is
shown in Fig. 2. Twenty-three (5%) of these
sessions were directly or indirectly related to COVID-19, and
the postgraduate clinics on Thursdays constituted 20 (4.7%) of
these sessions. The Pediatric Intensive Care Chapter of IAP has
begun the PICU e-Gurukul program, in which weekly lectures are
taken by stalwarts in the field of critical care. They have also
started P2P PICU Febinar (Peer-to-Peer PICU Fellows’ Webinar),
providing a national platform for the pediatric intensive care
fellows to present, teach and learn from each other. It is a
program ‘Of the Fellows, By the Fellows, For the Fellows.’ The
IAP respiratory chapter has started ‘Respinars’ for pulmonology
teaching, in which the experts of the field take lectures.
 |
|
Fig.1 Trend of
webinar numbers over the weeks. |
 |
|
Fig. 2
Sub-specialty distribution of online teaching sessions
on the dIAP platform. |
Similarly, each zone/state wing of IAP has also formulated their
teaching/academic sessions online. dIAP has also partnered with
the NHS UK through the Alder Hey academy global pediatric
lecture series (GPLS), thereby allowing an opportunity for
Indian students and pediatricians to participate in
distinguished lectures overseas. IAP has also come up with the
unique concept of conducting online conferences through dIAP.
The zonal meetings of IAP are being conducted by the name of
‘PediWeek’. Each zone was given one week, and this activity was
a huge hit and has been appreciated by one and all. It was a mix
of scientific and cultural activities. All pediatricians and
members of IAP had actively participated in these PediWeeks.
The dIAP sessions have helped in reaching students, private
practitioners, and pediatricians at various hos-pitals, who have
benefitted from these classes. The online learning archives
could form a database for teaching in the future. There have
been some sessions involving parents where they join hands with
the pediatricians for the wellbeing of the children. dIAP has
brought the teaching to your homes; it is eco-friendly,
paperless, saves travel and a lot of time. Moreover, all the
sessions are recorded, and one can watch them at their
convenience.
 |
|
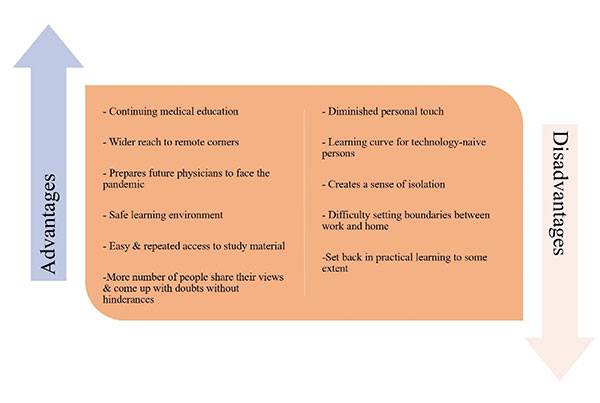
Fig. 3
Features of an online platform. |
However, it also has a
few disadvantages inherent to the online platform (Fig.
3). Literature on the impact of the pandemic on online
medical education has flagged communication and student
assessment problems, technology-related issues, and difficulties
in time management in these sessions. Despite these challenges
and technophobia, a majority have been able to achieve the
expertise quickly to conduct digital classes. Another drawback
is that it has decreased the personal touch and warmth, which
was there during the physical meetings. To overcome the various
problems, IAP has come up with specific solutions like
facilitating 24-hour teaching modules with feedback for
practical learning. The BLS (Basic life support) and ALS
(Advanced Life Support) modules have been remodeled to suit
e-learning. dIAP is also planning to include the live answers
from the audience during the lectures through the e-notepad.
With this software, the audience can easily select one of the
options given by the speaker. This year of the pandemic will
culminate with the highlight activity of IAP, i.e., the
National PediWeek – dIAP will be conducting a virtual national
conference which will take virtual teaching to a different
level.
Charles Darwin said, “it
is not the most intellectual of the species that survives; it is
not the strongest that survives, but the species that survives
is the one that is able best to adapt and adjust to the changing
environment in which it finds itself.” Online learning is
the new way of life that we must adapt to in the days and weeks
to come, which has been put into action by IAP.
I would like to
personally thank Dr. Arun Bansal, Dr G V Basavaraj and Dr Namita
Ravikumar who have spent their valuable time and effort to come
up with the facts and figures pertaining to the different
aspects in this document, making it an interesting and
informative read. I also hope that we can achieve even greater
heights by having a common goal – to enhance childcare in our
country and ensure that IAP becomes a well-known organization,
not just across the country, but rather across the entire world.
Let us strive to make the best of these trying times and ensure
the best for our mother organization.
Jai Hind! Jai IAP!


