|
|
|
Indian Pediatr 2012;49: 831-833
|
 |
Rituximab Followed by Mycophenolate Mofetil in
Children With IgM Nephropathy
|
|
Jin’ai Gu, Yonghui Xia, Jianhua Mao, Haidong Fu and
Ai’min Liu
From the Department of Nephrology, The Children’s
Hospital of Zhejiang University School of Medicine, Hangzhou 310003,
China.
Correspondence to: Dr Jianhua Mao, Department of
Nephro-logy, The Children’s Hospital of Zhejiang University School of
Medicine; Key Laboratory of Reproductive Genetics, Ministry of
Education; Zhejiang Key Laboratory for Diagnosis and Therapy of Neonatal
Diseases, Hangzhou 310006, Zhejiang Province, China.
Received: March 16, 2012;
Initial review: April 09, 2012;
Accepted: June 09,2012.
|
IgM nephropathy presents with refractory nephrotic syndrome and its
treatment is a significant challenge for pediatricians. We present two
patients with IgM nephropathy and frequently relapsing nephrotic
syndrome treated with rituximab and subsequently mycophenolate mofetil.
Both showed complete remission, which 24 to 30 months later, was still
maintained. The role of mycophenolate mofetil therapy in maintaining
remission after successful treatment of rituximab in IgM nephropathy
needs to be examined.
Key Words: IgM nephropathy, Management, Mycophenolate mofetil,
Rituximab.
|
|
Immunoglobulin M nephropathy often presents
with refractory nephrotic syndrome which may respond to steroid
treatment [1,2], though long-term remission of proteinuria was
achieved in only 14% patients, indicating the need for a more
effective treatment [1,3]. Rituximab, a chimeric monoclonal antibody
directed against the CD20 cell surface receptor expressed on B
cells, is successful for treatment of refractory idiopathic
nephrotic syndrome [4]. We report two patients with IgM nephropathy
and frequently relapsing nephrotic syndrome who responded to the
combination therapy of reduced-dose rituximab followed by
mycophenolate mofetil.
Case Reports
Case 1: This 14-month-old boy was
hospitalized for steroid sensitive nephrotic syndrome with but
frequentrelapse. Complete remission was achieved 12-days after
cyclosporine A therapy and maintained for the next 10 months. The
proteinuria recurred after an episode of pneumonia. The patient
later showed seven relapses within one year, associated with
hypertension, hirsutism and gingival hyperplasia. Renal biopsy
showed mesangial proliferation and IgM deposits in the mesangium.
Therapy with cyclosporine was stopped and he was
administered two doses of rituximab (375 mg/m 2/week
for 2 weeks). Complete remission was sustained and peripheral CD19
cell count dropped from 277/mm3
to 20/mm3,
but increased to 458/mm3
four months later. At that time, mycophenolate mofetil (20
mg/kg/day) was given as maintenance therapy. The patient has been on
remission for more than 2 years. CD19 positive lymphocyte count has
ranged between 863~1037/mm3
recently. At last follow-up, his serum creatinine was 0.39 mg/dL,
and 24-hr urinary protein was 98.5 mg.
Case 2: This 3-year-old had frequent
relapses in the first year of onset. The kidney biopsy revealed
mesangial proliferation with IgM mesengial deposits on
immunofluorescence examination and deposits electron dense deposits
on electron microscopy. She was administered tacrolimus at a dose of
87 µg/kg/day, and had complete remission after 15 days, which was
maintained for 15 months. The trough level of tacrolimus ranged from
4.5 to 8.1 ng/mL. Following stoppage of tacrolimus she had two
relapses despite low-dose prednisone (0.5 mg/kg/day).
We administered two dose of rituximab (375 mg/m 2/week
for 2 weeks). Complete remission was sustained two weeks later when
CD19/20 positive B lymphocytes were no longer detected.
Mycophenolate mofetil (17.5 mg/kg/day) was added 6 months after
rituximab administration when CD19 count recovered to 52/mm3.
Two years after the last dose of rituximab, complete remission was
maintained and no adverse events were observed during follow-up. The
patient had abdominal discomfort for three days during the initial
stage of mycophenolate mofetil therapy, but disappeared thereafter.
At last follow-up, her serum creatinine was 0.46mg/dL and 24-hr
urinary protein was 112.7 mg.
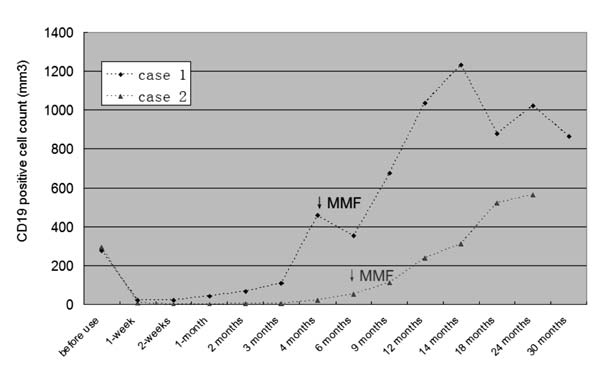
The variation of CD19 positive cell count and the
time for mycophenolate mofetil administration in both patients is
shown in Fig. 1. The research was approved by the
Ethics Committee of the University.
 |
|
Fig. 1 Variation of CD 19 positive
B cells in the two patients during follow-up. The time of
initiation of therapy with mycophenolate mofetil (MMF) is
shown by vertical arrows.
|
Discussion
IgM nephropathy is shown to have a unsatisfactory
response to steroids and more frequent relapses than minimal change
disease. [1] Betjes, et al. [5] described a recurred IgM
nephropathy patient after kidney transplantation, in whom two doses
of rituximab lead to complete and long-term remission.
The optimal dose of rituximab in idiopathic
nephrotic syndrome is not established. The standard protocol
consists of 4-doses of 375 mg/m 2
administered at weekly interval. This multi-dose regimen, however,
may cause hypersensitivity reactions and is expensive [6]. Several
prospective studies have reported that lower doses also lead to
CD19+ cell depletion and remission of proteinuria in idiopathic
nephrotic syndrome [7-8]. Gulati, et al. [9] reported 24
patients with steroid dependence who received 2 infusions of
rituximab. Remission was sustained in 20 (83.3%) patient at 12
months follow-up. Both of the present patients had favorable
response to two dose infusion of rituximab, and no further doses was
administered.
Rituximab has a significant steroid-sparing
effect in idiopathic nephrotic syndrome, however, patients are
likely to relapse with recovery of CD20+ cells. It is proposed that
additional therapy with mycophenolate mofetil sustains remission,
without the need to administer repeat dose of rituximab. Ito, et
al. [10] reported, in prospective cohort study, the efficacy of
combined therapy of rituximab followed by mycophenolate mofetil.
During 1-yr follow-up, 6 of nine patients did not relapse, implying
that maintenance therapy with mycophenolate mofetil is useful in
sustaining for remission. Similar results were seen in the two
patients in the present study.
Meanwhile, it is possible that the clinical
remission in many idiopathic nephrotic syndrome patients can
continue for a long time after the recurrence of B-cells. Kamei,
et al. [11] reported that B cell recovery need not result in
relapses. In the present study, remission was sustained despite
recovery of B cells after rituximab therapy. This study suggests
that rituximab may be a therapeutic option for the treatment of
patient with IgM nephropathy. The potential role of mycophenolate
mofetil therapy in maintaining remission after successful treatment
with rituximab needs to be prospectively examined.
Contributors: JG, HF and AL were involved in
management of patient and YX in interpreting the renal history. JM
designed the study and prepared the manuscript and shall act as the
guarantor.
Funding: Supported by National Natural
Science Foundation of China (Grant No. 30971365, 81070561 &
81170664), Zhejiang Provincial Healthy Science Foundation of China
(WKJ2010-2-014), Zhejiang Provincial Program for the Cultivation of
High-level Innovative Health talents and Zhejiang Provincial Natural
Science Foundation of China (Y12H050037);
Competing interests: None stated.
|
What This Report Adds?
• Combined therapy with rituximab and
mycophenolate mofetil is effective in sustaining remission
in patients with IgM nephropathy.
• Recovery of B-cells is not associated with relapse of
nephrotic syndrome.
|
References
1. Myllymaki J, Saha H, Mustonen J, Helin H,
Pasternack A. IgM nephropathy: clinical picture and long-term
prognosis. Am J Kidney Dis. 2003;41:343-50.
2. Westphal S, Hansson S, Mjornstedt L, Molne J,
Swerkersson S, Friman S. Early recurrence of nephrotic syndrome
(immunoglobulin M nephropathy) after renal transplantation
successfully treated with combinations of plasma exchanges,
immunoglobulin, and rituximab. Transplant Proc. 2006;38:2659-60.
3. Little MA, Dorman A, Gill D, Walshe JJ.
Mesangioproliferative glomerulonephritis with IgM deposition:
clinical characteristics and outcome. Ren Fail. 2000;22:445-57.
4. Gilbert RD, Hulse E, Rigden S. Rituximab
therapy for steroid-dependent minimal change nephrotic syndrome.
Pediatr Nephrol. 2006;21:1698-1700.
5. Betjes MGH, Roodnat JI. Resolution of IgM
Nephropathy After Rituximab Treatment. Am J Kidney Dis.
2009;53:1059-62.
6. Remuzzi G, Chiurchiu C, Abbate M, Brusegan V,
Bontempelli M, Ruggenenti P. Rituximab for idiopathic membranous
nephropathy. Lancet. 2002;360:923-4.
7. Kamei K, Ito S, Nozu K, Fujinaga S, Nakayama
M, Sako M, et al. Single dose of rituximab for refractory
steroid-dependent nephrotic syndrome in children. Pediatr Nephrol.
2009;24:1321-8.
8. Sugiura H, Takei T, Itabashi M, Tsukada M,
Moriyama T, Kojima C, et al. Effect of single-dose rituximab
on primary glomerular diseases. Nephron Clin Pract.
2011;117:c98-c105.
9. Gulati A, Sinha A, Jordan SC, Hari P, Dinda
AK, Sharma S, et al. Efficacy and safety of treatment with
rituximab for difficult steroid-resistant and -dependent nephrotic
syndrome: multicentric report. Clin J Am Soc Nephrol. 2010;5:
2207-12.
10. Ito S, Kamei K, Ogura M, Sato M, Fujimaru T,
Ishikawa T, et al. Maintenance therapy with mycophenolate
mofetil after rituximab in pediatric patients with steroid-dependent
nephrotic syndrome. Pediatr Nephrol. 2011;26:1823-8.
|
|
|
 |
|
