|
|
Recommendations Indian Pediatrics 2001; 38: 1106-1115 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Consensus Statement on Management of Urinary Tract Infections |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Urinary tract infections (UTI) are a common bacterial infection in infants and children. The risk of developing UTI before the age of 14 years is approximately 1% in boys and 3-5% in girls(1). The incidence varies with age. During the first year of life, the male to female ratio is 3-5:1. Beyond 1-2 years, there is female preponderance with male to female ratio of 1:10. The diagnosis of UTI is often clinically missed in young children, as symptoms are minimal and often non-specific. Rapid evaluation and treatment of UTI is important to prevent renal parenchymal damage (renal scarring) that can cause hypertension and chronic renal failure later. Risk factors for renal scarring include: young age especially children less than one-year-old; delay in initiating antibacterial treatment; recurrences of UTI; and presence of moderate to severe vesicoureteric reflux (VUR)(1). Pediatricians should be aware of the clinical features, diagnosis, management and appropriate further evaluation of children with UTI. Even a single confirmed UTI should be taken seriously. Patients with recurrent UTI and those having underlying renal and urologic abnormalities should be managed in consultation with a pediatric nephrologist. An Expert Group Meeting of the Indian Pediatric Nephrology Group was held on 15 December 2000 at New Delhi to formulate recommendations for management of patients with UTI (Annexure 1). This statement refers to the diagnosis, evaluation and treatment of such patients. Definitions Infection of the urinary tract is identified by growth of a significant number of organisms of a single species in the urine, in the presence of symptoms. Certain terms are commonly used in the evaluation and manage-ment of children with UTI (Table 1). The distinction between upper and lower UTI is not always possible or even necessary. The management of UTI is determined by the clinical severity of the illness. All febrile UTI are considered to involve the upper urinary tract with potential for renal scarring. An exception may be made in case of adolescent girls who present with symptoms restricted to the lower urinary tract. Presenting Symptoms The features of UTI in infants are nonspecific; thus, a high degree of suspicion is necessary. UTI should be suspected in an infant or child presenting with unexplained fever beyond three days(2). In neonates, UTI is usually a part of septicemia and presents with fever, vomiting, lethargy, jaundice and seizures. Infants and young children may present with recurrent fever, diarrhea, vomiting, abdominal pain and poor weight gain. Older children may have burning, urgency, frequency, flank pain, turbid or foul smelling urine or a recent onset of enuresis. The risk of UTI is higher in children with protein energy malnutrition and chronic diarrhea. Diagnosis The diagnosis of UTI is based on culture of a properly collected specimen of urine. Urinalysis is helpful in providing immediate information to suspect UTI and enable initiation of treatment. Confirmation of the diagnosis on urine culture is necessary (Table II)(1-3). Collection of Specimen The specimen for urine culture should be obtained carefully to prevent contamination by periurethral flora. A clean-catch midstream urine specimen is most widely used. Contamination by periurethral and prepucial organisms can be minimized by washing the genitalia with soap and water. Antiseptic washes and forced prepucial retraction are not advised. The specimen should be directly collected in a sterile glass or plastic bottle. In neonates and infants, urine samples are preferably obtained by suprapubic aspiration or urethral catheterization. Both techniques are safe and easy to perform(3). When supra-pubic aspiration or urethral catheterization is attempted, a sterile container should be kept ready to collect urine, which may be passed per urethra because of the stimulus provided by manipulation. Prompt plating of the urine specimen, within one hour of collection, is important. If delay is anticipated, the sample can be stored in a refrigerator at 4ºC for up to 24 hours. Cultures of urine specimens collected from a bag applied to the perineum have unacceptably high false positive rates, and are not recommended. Bag specimens are, however, a useful indicator of the absence of infection if no growth or a very scanty growth of usual urinary pathogens is found(1). A urine culture should be repeated in case contamination is suspected, e.g., mixed growth of two or more pathogens, or growth of organisms that normally constitute the periurethral flora (lactobacilli in healthy girls and enterococii in infants and toddlers). The culture is also repeated in situations where UTI is strongly suspected but colony counts are equivocal. Urinalysis A careful urinalysis, on a fresh urine sample, can identify children with a high likelihood of a UTI to enable presumptive treatment while awaiting results of urine culture(3). Several rapid screening tests are commonly used. Urinalysis may show mild proteinuria, leukocyturia (>5 leukocytes/high power field in a centrifuged sample or >10 leukocytes/mm3 in an uncentrifuged sample), bacteria on Gram stain and positive leukocyte esterase and nitrite test by dipstick. For predicting a positive urine culture, the presence of bacteria in a fresh urine specimen offers the best combination of sensitivity and specificity(4). Dipsticks perform nearly as well, when both leukocyte esterase and nitrite tests are combined, but the sensitivity is low in infants who void frequently and have a less vigorous inflammatory response(4,5). These dipsticks are not easily available in our country. Microscopic examination for leukocytes is less useful, especially in infants. Simple UTI UTI with low grade fever, dysuria, frequency, urgency but none of the above symptoms. Table I - Definitions
Table II - Interpretation of Urine Culture
Initial Evaluation Once UTI is suspected, the patient is examined for complications and the risk of recurrence. In an infant and young child, the degree of toxicity, dehydration and ability to retain oral intake is assessed. The blood pressure should be recorded and history regarding bowel and bladder habits elicited. Straining during micturition, dribbling, poor urinary stream and ballooning of the prepuce suggest obstruction. The abdomen is palpated for renal lumps and the genitalia examined for phimosis, tight prepuce or fused labia. Diurnal incontinence, urgency, frequency and squatting suggest voiding dysfunction; constipation or encopresis may be associated. In such children, examination of perineal sensation, deep tendon reflexes in the lower extremities and inspection of the lower back for sacral dimpling or other abnormalities is useful. Rectal examination should be done in patients with severe constipation. Blood levels of urea and creatinine are estimated. Total and differential white cell count and blood culture is obtained in children with complicated UTI. Ultrasound examina-tion of the abdomen is not required immediately unless there is clinical evidence of urinary tract obstruction or response to treatment is slower than anticipated. Treatment Therapy should be started after obtaining a urine culture. The patient’s age, degree of toxicity, state of hydration, ability to retain oral intake and the likelihood of compliance with medication help in deciding between outpatient therapy and hospitalization. Children with complicated UTI (Table I) and infants less than 3 months of age are treated with parenteral antibiotics (Table III). A combination of ampicillin and genta- micin, or a third generation cephalosporin (cefotaxime or ceftriaxone) is preferred. Gentamicin may be administered as a single medication in infants older than 3-6 months age. Once the child shows clinical improve- ment, with resolution of fever and toxicity, antibiotics may be administered orally. Young infants (<3 months old) and children with a positive blood culture should receive parenteral antibiotics for the entire duration of treatment. Oral medications are used in children above three months of age with a simple UTI (Table III). Amoxicillin, cotrimoxazole or an oral cephalosporin is preferred. Quinolones should be avoided as first line medication; their use is guided by results of urine sensitivity. Nalidixic acid or nitrofurantoin should not be used to treat UTI since they do not achieve therapeutic concentrations in the renal parenchyma and blood stream(2,3). An abdominal ultrasound examination and repeat urine culture are necessary in patients who fail to show clinical response (reduction of fever and toxicity) within 48 h or initiation of treatment. Duration of Treatment The usual duration of therapy is 10-14 days for infants and children with complicated UTI, and 7-10 days for simple infections(2). Shorter duration treatment regimens are not recommended in children. Following the treatment of the UTI, prophylactic antibiotic therapy is initiated, in children below 2 years of age, until appropriate imaging of the urinary tract is completed (Table IV). Supportive Therapy During an episode of an acute UTI, it is important to maintain adequate hydration. This might require special attention in a sick, febrile child with poor oral intake. A liberal fluid intake is encouraged and helps to alleviate dysuria. Alkalization of the urine is not necessary. Antipyretics are used to relieve fever. Table III - Antimicrobials for Treatment of UTI
Table IV - Antimicrobials for Prophylaxis of UTI
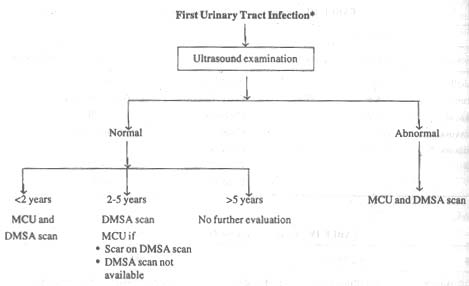
Subsequent Evaluation Imaging of the urinary tract is recommended for all children with UTI. The aim of these investigations is to identify patients at-risk of renal damage, mainly those below 5 years of age, with VUR or urinary tract obstruction. First Episode All children with the first UTI should be promptly investigated to identify those with an underlying urinary tract anomaly. Guidelines for evaluation of patients vary. Recommendations of the Expert Group are shown in Fig.1.
* Detailed evaluation with ulrasound, MCU and renal scan is recommended for all children with recurrent UTI.
Below the age of 2 years, an ultrasound and micturating cystourethrogram (MCU) are recommended. These investigations will detect most cases of reflux nephropathy or those ‘at-risk’ in this age group. Urinary tract ultrasonography will identify hydronephrosis, dilatation of ureter, bladder hypertrophy, ureterocele and post-void residual ruine. Ultrasonography should be performed within 2-4 weeks following the UTI. Children requiring ]hospitalization for complicated UTI should preferably be screened with an ultrasound before their discharge. The MCU is useful for the diagnosis and grading of VUR, and detection of posterior urethral valves, ureterocele and bladder or urethral diverticuli. MCU is usually per-formed 4-8 weeks after treatment of the UTI. Concerns that obtaining a MCU too soon after a UTI result in a false-positive study are ill founded. It is rare for reflux to be detected during UTI and then to disappear following treatment(3). In order to prevent infection following catheterization, the MCU should be done under cover of prophylactic anti-biotics(6). Amoxicillin is administered orally in a dose of 50 mg/kg, 1 h before the proce-dure and 25 mg/kg 6 h later. Alternatively, gentamicin (2-3 mg/kg intramuscular) may be given 30 minutes before the MCU. If available, renal scintigraphy using 99mTc-radioloabeled dimercaptosuccinic acid (DMSA) or glucoheptonate (GHA) should be performed in all children below two years of age. Renal scintigraphy (ideally performed 3 months after treatment of the UTI) is an excellent technique for detecting renal cortical scarring. Between the ages of 2-5 years, a MCU is not immediately required, unless the symptoms suggest an underlying obstruction. An ultrasound and a DMSA (or GHA) renal scan are done, and MCU performed only if either of the former investigations is abnormal. By pursuing this policy, the number of cystograms performed in this age group is restricted to patients having renal anomalies. In case facilities for radionuclide scans are not available, MCU should be performed as for younger children. Children over the age of 5 years can be reliably screened with ultrasonography per-formed by an expert. Imagine with MCU and renal scan are necessary only if abnormalities are found on ultrasound examination. The presence of VUR can also be demons-trated on direct radionuclide cystography (DRCG). However, grading of reflux using this method is not reliable. DRCG does not evaluate the morphology of the urethra and bladder, and is thus not useful for establishing a diagnosis of posterior urethral valves or other anomalies. This technique is therefore not suitable as the initial procedure for evaluation of the lower urinary tract. Recurrent UTI Children with more than one episode of UTI, irrespective of age, are evaluated with ultrasound and MCU. A renal cortical scan (DMSA or GHA) to detect scars is recommended. Patients showing hydronephrosis in the absence of VUR should be evaluated by diuretic renography using 99mTc-labeled diethylenetriamine-pentaacetic acid (DTPA) or mercaptoacetyl-glycine (MAG-3). These techniques provide quantitative assessment of renal function and drainage of the dilated collecting system. Additional Investigations An X-ray of the spine may be done to look for spinal dysraphism if clinically suspected. An X-ray film of the kidney and urinary bladder region may show radiopaque renal or vesical calculi. The importance of intravenous pyelography (IVP) has declined following the availability of radioisotope scans. However, an IVP may be performed to examine for renal scarring if facilities for renal scintigraphy are not available. Cystoscopy is almost never required for evaluation of patients with UTI. Urine Culture Urine cultures need not be routinely repeated at cessation of antibiotic therapy. A culture should however be obtained in patients who fail to show the expected response to the treatment or have recurrence of symptoms suggestive of a UTI. The occasional detection of significant bacteriuria in the absence of symptoms suggests the diagnosis of asympto-matic bacteriuria, which does notrequire treatment (see below). Antibiotic Prophylaxis Long-term, low dose, antibacterial prophylaxis is used to prevent recurrent febrile UTI. The ideal antibiotic used should be effective, non-toxic with few side effects and not alter the indigenous bacterial flora or induce development of bacterial resistance(7). Medications used for prophylaxis (Table IV) are given as a signal bedtime dose. Indications and Duration of Prophylaxis Antibiotic prophylaxis is recommended under the following circumstances:
The indications and duration of prophylaxis depend on the age of the child, presence of VUR and/or a renal scar on evaluation (Table V). Antibiotic prophylaxis is not recommended in patients with urinary tract obstruction (e.g., posterior urethral valves), urolithiasis or neurogenic bladder. Under these circumstances, prophylaxis can increase the chance of colonization with resistant organisms. Measures to Reduce Recurrent UTI Circumcision is not recommended routinely but may be considered for infants with recurrent UTI(7,8). Attention to under-garments and perineal hygiene, including the foreskin in boys, is explained to the parents. Plenty of fluid intake and frequent voiding ensures flushing out of the uropathogens. Constipation predisposes to recurrent UTI and improvement in bowel habits reduces the incidence of UTI(9). In children with VUR who are toilet trained, regular and volitional low pressure voiding with complete bladder emptying is encouraged. Double voiding is recommended in order to empty the bladder of post-void residual urine. Breakthrough UTI on Prophylactic Antibiotics Recurrences can occur due to infections caused by bacteria that are resistant to the antibiotic used for prophylaxis, or by sensitive bacteria (due to poor compliance, inadequate or infrequent dosing). Poor bladder emptying also predisposes to breakthrough infections. Breakthrough UTI should be treated with appropriate antibiotics. Change of the medication being used for prophylaxis is not usually required. There is no role for cyclic therapy, where the antibiotic used for prophylaxis is changed every 6-8 weeks. Patients having recurrent breakthrough infections may benefit from double prophy-laxis with cotrimoxazole and nitro-furantoin(7). Asymptomatic Bacteriuria The frequency of asymptomatic bacteri-uria is about 1% in girls and 0.05% in boys. History is taken for failure to thrive, abdominal pain, unexplained febrile episodes, voiding dysfunction or constipation to detect abnormalities that need appropriate manage-ment. Bacteriuria in the absence of symptoms is a benign condition, which does not cause renal injury. The organisms isolated in most instances are usually E. coli, which are of low virulence. Eradication of these organisms is often followed by symptomatic infection with more virulent strains. Thus, use of antibiotics to treat asymptomatic bacteriuria or antibiotic prophylaxis is not indicated(10). Vesicoureteric Reflux VUR is seen in 30-50% children and 40-50% infants with UTI. Reflux predisposes to renal infection by facilitating the transport of bacteria from the bladder to the upper urinary tract. The presence of moderate to severe VUR is an important risk factor for acute pyelonephritis and reflux nephropathy. The severity of VUR is graded using the International Study Classification from grade I to V, based on the appearance of the urinary tract on contrast MCU(3). Children with high grade reflux who acquire a UTI are at significant risk for pyelonephritis and renal scarring. Renal imaging (to assess renal scarring) can be performed using ultra-sonography, intravenous pyelography or radionuclide scans (preferred). With bladder growth and maturation, there is a tendency for reflux to resolve or improve. Lower grades of reflux (Grade I-III) are much more likely to resolve than are higher grades. Bladder Dysfunction with VUR There is increasing evidence that voiding dysfunction may be found in 50-60% of children with VUR persisting beyond 2-3 years of age(11,12). The unstable bladder is characterized by frequency, urgency, incontinence and holding maneuvers (e.g., squatting). Patients with dyscoordinated bladder show urgency, hesitancy, diurnal and nocturnal incontinence, voiding in an inter-rupted manner and recurrent UTI. Almost a third of children with bladder dysfunction have no symptoms. All patients with VUR should be assessed for bladder dysfunction. A detailed history of the voiding pattern is taken and lower back examined for spinal dysraphism. Bowel habits should be assessed. Presence of increased post-void urine in the bladder on ultra-sonography, in the absence of anatomical obstruction, suggests bladder dysfunction. If clinically suspected, flowmetry and urodyna-mic studies are necessary. Urodynamic evaluation is also recommended in all children being considered for surgical repair of VUR. The management of voiding dysfunction should be carried out in collaboration with a pediatric nephrologist. Treatment of VUR VUR is unlikely to cause renal injury in the absence of infection. Thus, the aim of management is prevention of renal injury secondary to recurrent UTI. Treatment options for VUR are conti-nuous antibiotic prophylaxis or its surgical repair. Large randomized controlled trials that compared antibiotic prophylaxis with anti-reflux surgery show similar outcome(13). The clinician should discuss the benefits and risks of these options with the parents(8,13,14). Therapeutic recommendations depend on the patient’s age at diagnosis, grade of VUR, findings on renal imaging and occurrence of breakthrough infections on follow-up (Table VI). Most children with VUR are managed on long-term antibiotic prophylaxis while awaiting spontaneous resolution of VUR. The patients are kept on close follow up for occurrence of breakthrough UTI. A DRCG scan or MCU is repeated after 12-18 months to evaluate for resolution of reflux. A DMSA renal scan is repeated, in patients having breakthrough UTI, to detect fresh renal scarring. The risk of recurrent UTI and renal scarring is low after 4-5 years of age(8,13). The Expert Group recommends that prophy-laxis be discontinued in children beyond 5 years of age with normal bowel and urinary habits, even if mild to moderate reflux persists. Grade V or bilateral grade IV VUR, which persists after one year of age, should be repaired surgically. Surgical repair should also be offered to patients with persistent VUR who have recurrent UTI, fresh renal scars, or show poor compliance and irregular follow up. Antibiotic prophylaxis is continued for 6 months after surgical correction of VUR. Endoscopic injection of various agents, in the submucosal ureteric tunnel, has been advocated for correction of milder grades of reflux. However, precise guidelines on indications for this procedure are not available(8,14). Based on current evidence, the Expert Group does not recommend endoscopic treatment for VUR. Long Term Follow up Children with renal scarring should receive continued care twice a year through adulthood. Patients are monitored for physical growth and blood pressure. Investigations include urinalysis for proteinuria every six months, and yearly estimation of blood levels of urea and creatinine. Urine should be promptly cultured in patients having features suggestive of UTI. Yearly ultrasound examinations are done to monitor renal growth. Table V - Indications and Duration for Antimicrobial Prophylaxis
Table VI - Treatment of Primary Vesicoureteric Reflux
Conclusions The recommendations that are given represent the consensus view of the Indian Pediatric Nephrology Group. They have been formulated on basis of best current practice, which is supported by studies published in peer-reviewed journals and the experience of the Expert Group. They are intended to provide pediatricians with broad guidelines for managing children with urinary infections. Annexure I Participants of the Expert Group Meeting
Compiled by:
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||