|
Fetus in Fetu (FIF) is an entity where one
vertebrate underdeveloped twin develops inside the other normal host
twin. Till date only about 100 cases have been reported. Most of the
case reports describe a single FIF. We report a case of double FIF
in a six-week-old infant.
Case report
A 6 weeks old infant presented to us with an
abdominal lump and vomiting. The infant was born full term by normal
vaginal delivery with a birthweight of 2500g. The baby was well till
2 weeks of life when the mother noticed an abdominal lump, which
gradually increased in size leading to abdominal distention. The
infant also started vomiting after feeds but continued to pass
normal stools. On presentation to our hospital, the child weighed
3500g and his vitals were maintained. On abdominal examination there
was distension and there was a well defined firm, round, non-tender
mass in the right upper abdomen, occupying the right hypochondrium
and lumbar region extending a little into the iliac fossa. The bowel
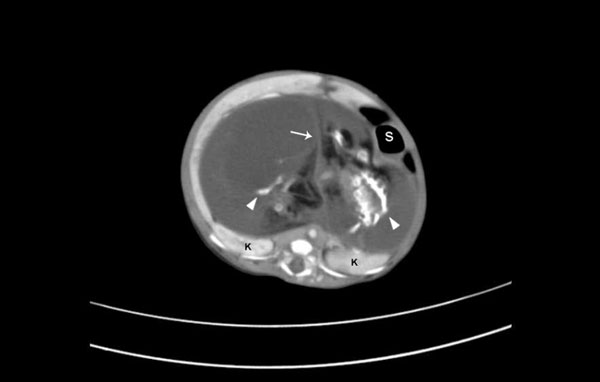
sounds were normal. CT abdomen revealed a heterogenous well
encapsulated mass in the upper abdomen displacing the liver, bowel
and stomach anteriorly (Fig. 1). The mass was divided
by thin septa into two compartments. Both the compartments contained
two separate soft tissue shadows with separate sets of ossific
elements resembling a vertebral column with a rudimentary rib cage.
A provisional diagnosis of double or twin fetus in fetu was made and
the infant was taken up for surgery. During surgery, a large cystic
retroperitoneal mass was visible pushing the liver upwards and the
rest of the abdominal contents to the left. The liver was mobilized
and after further dissection and removing the peritoneum, the cystic
mass was exposed. An attempt was made to remove the whole cystic
mass as such but to prevent injury to the portal structures the
capsule had to be incised. This revealed two fetuses lying in a pool
of amniotic fluid. The blood supply to the sac was derived from the
abdominal aorta of the baby and the venous drainage was to the
inferior vena cava. The mass was resected. The post-operative period
went uneventful and the infant was discharged on the 10 th
postoperative day. The child is doing well on follow up.
 |
|
Fig. 1 (a) Axial contrast enhanced
CT showing a cystic mass divided by a septa (arrow) containing
two sets of ossific elements (arrow heads). The mass has
pushed the kideys (K) posteriorly and the stomach (S)
anteriorly. |
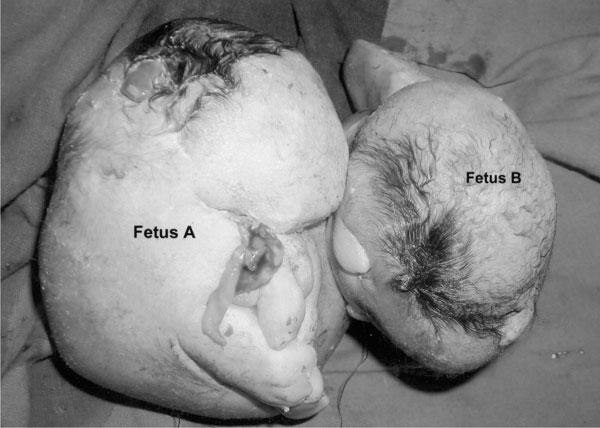
On examination, one of the fetuses weighed 250g
(fetus A) and the other one weighed 180g (fetus B) (Fig. 2).
On gross examination fetus A showed scalp hair, optic pits,
rudimentary auricles, primitive fore and hind appendages. There was
no digit formation. On dissection a complete vertebral column was
seen. Stomach and small intestine were developed. Rudimentary liver
and left kidney was visible. The cranial cavity was filled with
clear fluid and was devoid of any brain tissue. A malformed heart
with no defined chambers was seen lying in the cervical region.
Fetus B was less developed than its twin. It also had scalp hair but
only a single rudimentary forelimb and the caudal end was not
differentiated. On dissection the vertebral column was seen along
with the stomach. No other abdominal organs were differentiated.
 |
|
Fig. 2 Photograph of the twin fetuses
in fetu. |
Discussion
Fetus in fetu (FIF) is a very rare cause of an
abdominal mass in an infant. Multiple fetuses in fetu are still
rarer [1-3]. FIF has been believed to arise from inclusion of one
monozygotic- diamniotic twin into the other twin. There have been
reports of FIF being detected as early as in the newborn period or
even as late as adulthood [4]. Few cases of FIF have been detected
antenatally as a cystic intra-abdominal mass growing inside the
fetus [5]. The most common site is the retroperitoneum but FIF have
been reported at various sites right from the cranial cavity to the
scrotal sac [6,7]. The monozygosity of the twins can be confirmed by
presence of identical sex karyotype, histocompatibility types and
blood groups.
There has been a controversy regarding the
differentiation between a teratoma and FIF. Some even consider them
to be the two ends of a spectrum, FIF being a highly organized form
of a teratoma [8]. Differentiation criteria between the two were
suggested [9]. Teratomas are considered to arise from pluripotent
cells but do not demonstrate vertebrae or systemic organogenesis.
The commonest site for a teratoma is the sacrococcygeal region and
they have a definite malignant potential. In contrast, the FIF are
usually retroperitoneal, have a vertebral skeleton, are benign and
usually have variably differentiated organ system and limbs.
In our patient, the diagnosis of FIF was
suggested by presence of a vertebral column in the mass on an
abdominal X-ray. CT imaging gives a more accurate diagnosis
and defines the relation of the mass with the other intra-abdominal
structures [10]. The twin fetuses in fetu in our case fulfilled the
criteria for being FIF and not a teratoma. Identification of a
vertebral column indicates development of the parasite twin at least
up to the stage of notochord from which the vertebral column arises.
Symptoms of FIF are primarily due to its mass effect such as
abdominal distention, feeding difficulty, emesis, jaundice or
pressure effects on the renal or gastrointestinal system. Complete
excision as was done in our patient ensures definitive cure .
Contributions: RR and DA were involved in
case management and writing the manuscript. DKS was involved in
drafting the manuscript and searching the literature. PK provided
expert radiological opinion and critically reviewed the manuscript.
Funding: None.
Competing interests: None stated.
References
1. Pourang H, Sarmadi S, Mireskandari SM,
Soleimani M, Mollaeian M, Alizadeh H, et al. Twin fetus in
fetu with immature teratoma: A case report and review of the
literature. Arch Iranian Med. 2009;12:507-10.
2. Daga BV, Chaudhary VA, Ingle AS, Dhamangaokar
VB, Jadhav DP, Kulkarni PA. Double fetus-in-fetu: CT scan diagnosis
in an adult. Indian J Radiol Imaging. 2009;19:216-8.
3. Gangopadhyay AN, Srivastava A, Srivastava P,
Gupta DK, Sharma SP, Kumar V. Twin fetus in fetu in a child: a case
report and review of the literature. J Med Case Reports. 2010;4:96.
4. Dagradi AD, Mangiante GL, Serio GE, Musajo FG,
Menestrina FV. Fetus-in-fetu removal in a 47-year-old man. Surgery.
1992;112:598-602.
5. Mills P, Bornick PW, Morales WJ. Ultrasound
prenatal diagnosis of fetus in fetu. Ultrasound Obstet Gynaecol.
2001;18:69-71.
6. Afshar F, King TT, Berry CL. Intraventricular
fetus-in-fetu. J Neurosurg. 1982;56:845-9.
7. Kakizoe T, Tahara M. Fetus in fetu located in
the scrotal sac of the newborn infant. J Urol. 1972;107:506-8.
8. Potter EL. Pathology of the fetus and the
newborn. In: Potter EL, eds. Pathology of the fetus and
newborn. 2nd ed. Chicago, III: Year book, 1961. p. 183-7.
9. Willis RA. The borderland of embryology and
pathology. Bull N Y Acad Med. 1950;26:440-60.
10. Iyer KV, Vinayak K, Haller JO, Maximin S,
Barrerras J, Velchek F. Multiple fetuses in fetu: Imaging findings.
Pediatr Radiol. 2003;33:53-5.
|


