T
he American Heart
Association (AHA) 2020 guidelines with their changes for
pediatric basic and advanced life support were issued recently
[1]. We have discussed the changes made under three headings –
pre-arrest, intra-arrest and post arrest care. This will make it
convenient to compare these with the 2015 document, wherein a
similar division was presented.
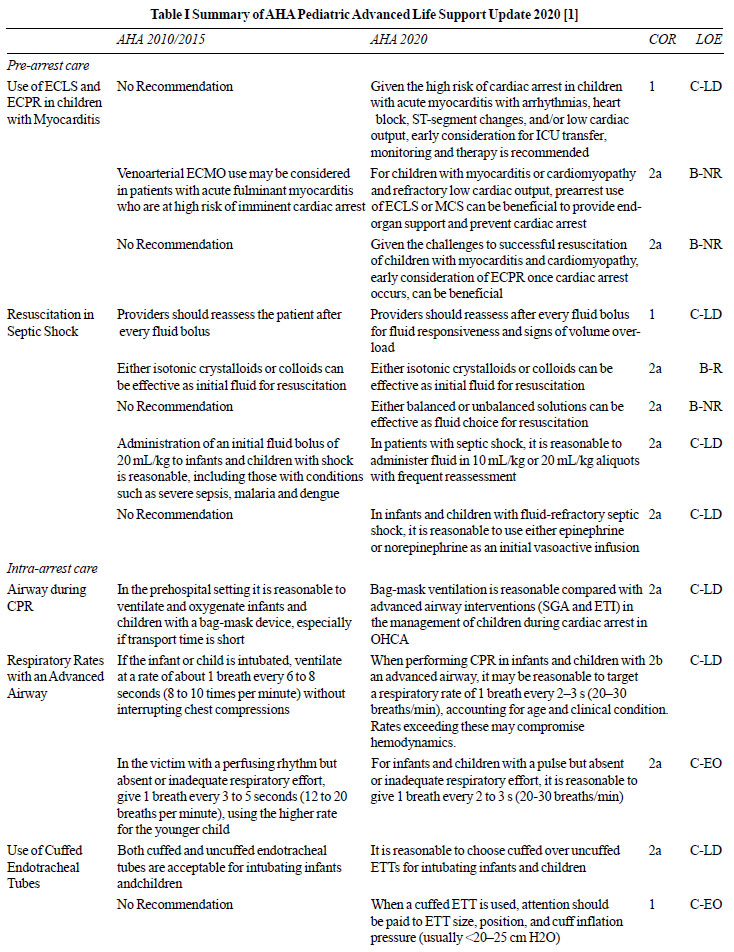
PRE-ARREST CARE
The updated guidelines reaffirm the
importance of prevention and preparedness for a cardiac arrest
in children as the first component in the chain of survival.
ECLS and ECPR in Children With Myocarditis
Newer evidence that has emerged since the
last guidelines, shows that pre-arrest use of Extra Corporeal
Life Support (ECLS) or Mechanical Circulatory Support (MCS) in
patients with myocarditis may lead to better organ support and
prevention of cardiac arrest. The survival to hospital discharge
in patients with structurally normal hearts, receiving
Extracorporeal Cardiopulmo-nary Resuscitation (ECPR) was 32% in
adults. Myocarditis was a favorable prognostic marker for the
use of ECPR in this study. Children with acute fulminant
myocarditis had a 75% survival after ECLS/MCS either with
recovery of native function (43.8%) or post cardiac transplant
(31.3%) [2]. Retrospective analysis of the Extracorporeal Life
Support Organization (ELSO) database showed a 61% survival to
hospital discharge, 3% of these with heart transplantation. A
recent German prospective registry showed weaning rates of 42%
in children with myocarditis who received ECLS. Early transfer
to ICU is also recommended for monitoring and initiation of
therapy.
Resuscitation in Septic Shock
Type of fluid: The newer
guidelines have jumped into the raging debate between balanced
and unbalanced crystalloids as initial fluid of choice in septic
shock. Balanced crystalloids, with a composition closer to that
of normal human plasma, were postulated to reduce the incidence
of hyperchloremic metabolic acidosis and acute kidney injury
(AKI). A retrospective matched analysis showed better survival
at 72 hours and lower rates of AKI with balanced crystalloids
although another similar analysis showed no difference [3,4]. A
pilot RCT, that failed to demonstrate any difference, however,
established the feasibility of further research in this area.
While the physiological rationale for using balanced over
unbalanced crystalloids seems sound, one cannot be recommended
over the other, based on the current evidence.
Volume of fluid: The updated guidelines
suggest that it is reasonable to administer fluids in smaller
aliquots of 10-20 mL/kg with careful reassessment for both fluid
responsiveness and overload after each bolus to titrate further
therapy. There is a growing inventory of evidence beginning with
the FEAST Trial, warning against the perils of overzealous fluid
administration in septic shock. The last AHA update in 2015 had
recommended cautious fluid resuscitation in setups with limited
access to intensive care resources. The current 2020 update,
however, recommends it uniformly, irrespective of availability
of intensive care resources. On the contrary, the Survival
Sepsis Campaign (SSC) Guidelines 2020 recommend smaller volume
boluses of 10-20 ml/kg, upto 40-60 mL/kg in the first hour of
resuscitation, where intensive care resources are available. In
settings with a lack of access to intensive care, SSC
recommendations differ; in the absence of hypotension
(compensated shock), fluid boluses are not recommended but if
hypotension is present, 10-20 mL/kg bolus may be administered
with close monitoring and utmost caution [5].
Inotropes during septic shock: It is
reasonable to use either epinephrine or norepinephrine as a
vasoactive infusion in septic shock. This is the first time the
AHA has made such a recommendation for use of inotropes,
specifically for septic shock. This is based on two important
trials demonstrating superiority of epinephrine over dopamine in
pediatric septic shock. The American College of Critical Care
Medicine recommended use of either epinephrine or norepinephrine
in septic shock depending on its ‘cold’ or ‘warm’ nature [6].
The distinctions into warm and cold shock have since been
abandoned by newer guidelines [5]. Norepinephrine, however, has
been found to be safe and effective as a first line agent in
pediatric septic shock.
INTRA-ARREST CARE
Advanced Airway During CPR
It has been seen in one prospective and 2
retrospective studies that endotracheal intubation and bag-mask
ventilation (BMV) have comparable outcomes in out-of-hospital
cardiac arrest (OHCA) in children [7]. Similar comparative data
is however not available for in-hospital cardiac arrest (IHCA).
Respiratory Rates with an Advanced Airway
While formulating the previous guidelines,
there was lack of evidence to support the use of respiratory
rates different from those recommended in adults. Since then,
newer evidence has emerged that higher respiratory rates may
improve survival in children undergoing CPR, with a rider that
overventilation may lead to hypotension [8]. Thus, rescue
breaths should now be given at the rate of one breath every 2-3s
(20-30/min) when an advanced airway is in place and while
performing chest compressions.
Cuffed Endotracheal Tubes (ETT)
The guidelines suggest that it may be
reasonable to use cuffed over uncuffed ETT in infants and
children. This is based on evidence that cuffed tubes improve
ventilation and reduce the incidence of ETT changes, leading to
lesser trauma [9]. Care should be given towards choosing the
appropriate size and maintaining cuff pressures <20-25 cm H2O.
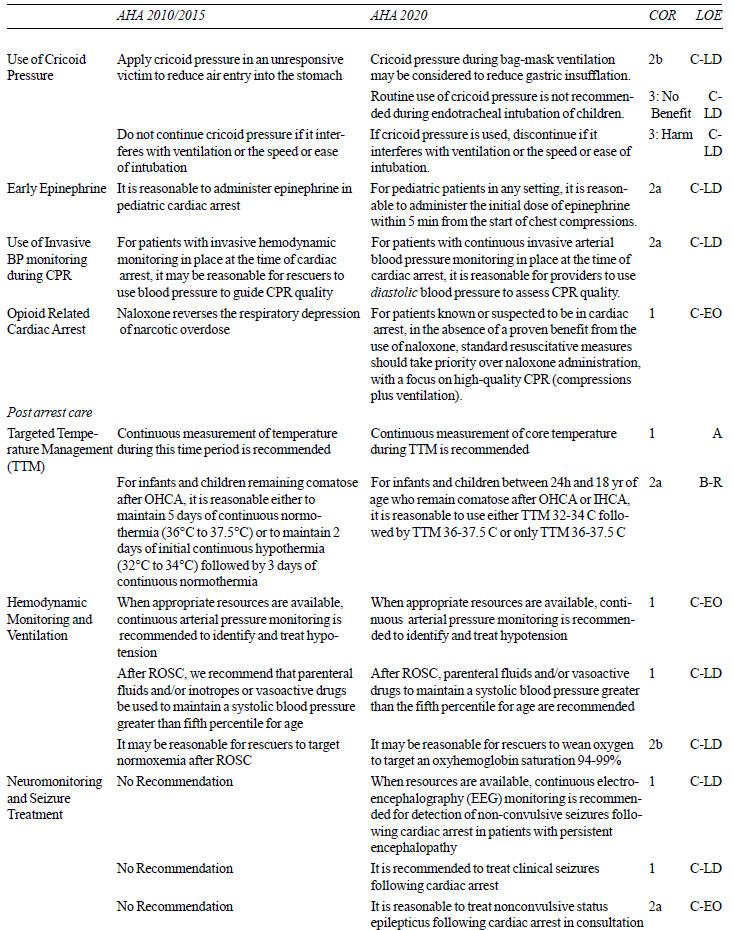
Cricoid Pressure
Contrary to the previous guidelines, which
recommended routine use of cricoid pressure (unless the maneuver
interferes with ventilation) in unresponsive children, the
current guidelines recommend it in select cases primarily to
prevent stomach insufflation. Routine use can hamper
visualization during laryngoscopy and BMV. Newer data has shown
that cricoid pressure during intubation and ventilation did not
result in lower rates of regurgitation while decreasing success
rates for first-attempt intubation.
Early Epinephrine
It has been established in past guidelines
that epinephrine has an important role in improving coronary and
cerebral perfusion during CPR. The newer guidelines put a
renewed emphasis on the timing of administration of epinephrine.
Early (<5 min) administration of epinephrine from the start of
chest compressions in pediatric cardiac arrest was associated
with improved outcomes in multiple recent multicenter data
[10,11].
Use of Invasive BP monitoring during CPR
It has been suggested that in patients with
invasive arterial BP monitoring lines in place, it is reasonable
to use diastolic BP as a guide for quality of CPR. This
recommendation stems from the evidence that a DBP >25 mmHg in
infants and >30 mm Hg in children during CPR was associated with
greater chances of survival to hospital discharge and better
neurological outcome.
Opioid Related Cardiac Arrest
Updated guidelines emphasize the importance
of routine CPR protocol over naloxone use in opioid related
cardiac arrest. This arises from lack of evidence for benefit of
naloxone in opioid related cardiac arrest. Once CPR has been
initiated as per protocol, it is reasonable to administer
naloxone in suspected or confirmed opioid related cardiac
arrests.
POST-ARREST CARE
Achieving Return of Spontaneous Circulation
(ROSC) is just the beginning for the healthcare providers.
Following ROSC, the patient moves into the "Post Cardiac Arrest
Syndrome" which includes ischemia and reperfusion injury to
organs along with persisting pathophysiological derangement
related to inciting trigger.
Targeted Temperature Management (TTM)
The guidelines bring into the main fold, the
focused update issued in 2019 about TTM. Continuous core
temperature management is recommended for post cardiac arrest
patients (Both IHCA and OHCA). Hyperthermia should be strictly
prevented. Either hypothermia followed by normothermia or only
normothermia had similar outcomes at 1 year in 2 pediatric RCTs
[12,13] and hence either may be used.
Hemodynamic Monitoring and Ventilation
The guidelines strongly advocate use of
invasive arterial BP for post cardiac arrest monitoring when
available and to maintain SBP >5
th
percentile for age. The recommendation comes from the fact that
BP is labile in the period following ROSC and intermittent NIBP
may be unreliable. While ventilating patients post ROSC, it has
been re-emphasized that normoxemia and normocarbia should be
maintained. Hyperoxemia (Spo2 100%) was not associated with
better outcomes and therefore targeting SpO2 of 94-99% may be
more prudent.
Neuromonitoring and Seizure Treatment
When available, continuous EEG monitoring is
recommended following ROSC as evidence has shown that non
convulsive status epilepticus (NCSE) is common in these
children. It has also been seen that children with clinical or
non-convulsive seizures following ROSC have worse outcomes.
However, no recommendation has been made regarding prophylactic
use of AEDs in children without clinical or non-convulsive
seizures.
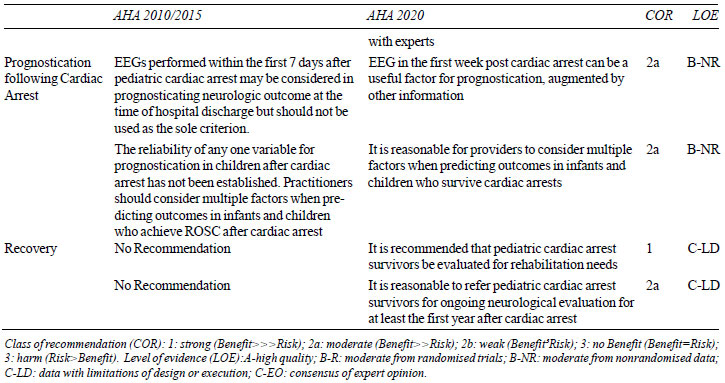
Prognostication Following Cardiac Arrest
Certain EEG patterns have been seen to be
associated with favorable (Sleep spindles, normal background,
reactivity) and poor (burst suppression, flat/attenuated)
outcomes but the sensitivity and specificity are not high enough
to recommend use of isolated EEG for prognostication [14].
Multiple factors including but not limited to EEG, neuroimaging
and biomarkers should be taken into account for prognostication.
In the absence of robust data, one should avoid being dogmatic
while predicting outcomes following cardiac arrest.
Recovery – A New Addition to the Chain of
Survival
One of the major changes in the new
guidelines is the updated chain of survival. It has been
recognized that IHCA and OHCA have very different outcomes and
different chains of survival have been formed for them. Both
these chains now have a new sixth component which is ‘recovery’.
Cognitive, neuropsychological and physical impairments continue
post discharge [15]. Ongoing assessment and support following
hospital discharge is essential for improving long term outcomes
in these children.
Contributors: MSR,VCR: drafted the
manuscript; MJ: editing, review and final approval. All authors
approved the final version of manuscript, and are accountable
for all aspects related to the study.
Funding: None; Competing
Interest: None stated.
REFERENCES
1. Topjian AA, Tia RT, Atkins D, et al. Part
4: Pediatric Basic and Advanced Life Support: 2020 American
Heart Association guidelines for cardiopulmonary resuscitation
and emergency cardiovascular care. Circulation.
2020;142:S469-523.
2. Wilmot I, Morales DLS, Price JF, et al.
Effectiveness of mechanical circulatory support in children with
acute fulminant and persistent myocarditis. J Card Fail.
2011;17:487-94.
3. Emrath ET, Fortenberry JD, Travers C,
McCracken CE, Hebbar KB. Resuscitation with balanced fluids is
associated with improved survival in pediatric severe sepsis.
Crit Care Med. 2017;45:1177-83.
4. Weiss SL, Keele L, Balamuth F, et al.
Crystalloid fluid choice and clinical outcomes in pediatric
sepsis: a matched retrospective cohort study. J Pediatr.
Elsevier; 2017;182:304-310.e10.
5. Weiss SL, Peters MJ, Alhazzani W, et al.
Surviving sepsis campaign international guidelines for the
management of septic shock and sepsis-associated organ
dysfunction in children. Pediatr Crit Care Med. 2020;21:e52.
6. Davis AL, Carcillo JA, Aneja RK, et al.
American college of critical care medicine clinical practice
parameters for hemodynamic support of pediatric and neonatal
septic shock. Crit Care Med. 2017;45:1061-93.
7. Hansen ML, Lin A, Eriksson C, et al. A
comparison of pediatric airway management techniques during
out-of-hospital cardiac arrest using the CARES database.
Resuscitation. 2017;120:51-6.
8. Sutton RM, Reeder RW, Landis WP, et al.
Ventilation rates and pediatric in-hospital cardiac arrest
survival outcomes. Crit Care Med. 2019;47:1627-36.
9. De Orange FA, Andrade RG, Lemos A, et al.
Cuffed versus uncuffed endotracheal tubes for general
anaesthesia in children aged eight years and under. Cochrane
Database Syst Rev 2017. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC6486166/.
Accessed on October 31, 2020.
10. Hansen M, Schmicker RH, Newgard CD, et
al. Time to epinephrine administration and survival from
nonshockable out-of-hospital cardiac arrest among children and
adults. Circulation. 2018;137:2032-40.
11. Andersen LW, Berg KM, Saindon BZ, et al.
Time to epinephrine and survival after pediatric in-hospital
cardiac arrest. JAMA. 2015;314:802-10.
12. Moler FW, Silverstein FS, Holubkov R,
Slomine BS, Christensen JR, Nadkarni VM, et al. Therapeutic
hypothermia after out-of-hospital cardiac arrest in Children. N
Engl J Med. Massachusetts Medical Society; 2015;372:1898–908.
13. Moler FW, Silverstein FS, Holubkov R, et
al. Therapeutic hypothermia after in-hospital cardiac arrest in
children. N Engl J Med. Massachusetts Medical Society;
2017;376:318-29.
14. Topjian AA, Sánchez SM, Shults J, et al.
Early EEG Background features predict outcomes in children
resuscitated from cardiac arrest. Pediatr Crit Care Med J Soc
Crit Care Med World Fed Pediatr Intensive Crit Care Soc.
2016;17:547-57.
15. van Zellem L, Utens EM, Madderom M, et
al. Cardiac arrest in infants, children, and adolescents:
long-term emotional and behavioral functioning. Eur J Pediatr.
2016;175:977-86.