The controversy about what fluids to use in critically
ill children to prevent hyponatraemia is ongoing. We congratulate Singhi
and Jayashree for their contribution to this debate(1). There is however
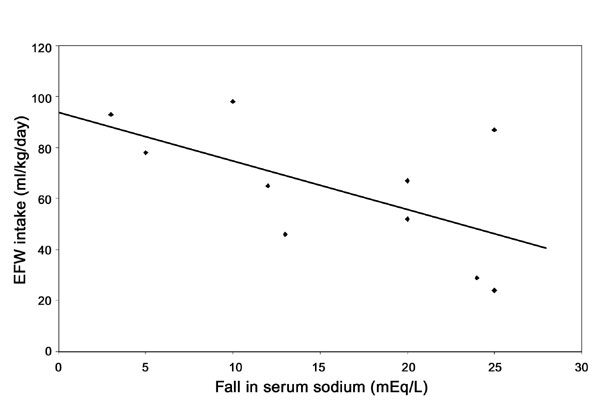
one point in their paper that needs clarification. In Fig.1,
a line showing electrolyte free water (EFW) intake and expected fall in
serum sodium has been drawn. It runs diagonally across the figure
suggesting that a linear relationship between the two is expected. The
data source for this assumption has not been provided.
 |
|
Fig.1 Electrolyte free water (EFW) and fall
in sodium. |
Interestingly, in their data on children who developed
hyponatraemia, the biggest falls in serum sodium were seen in the patients
who received less EFW (r = – 0.57). The message can be best
conveyed by drawing the regression line. We have scanned in their figure
and have drawn the regression line in the attached figure. This graph
depicts data on the relationship of EFW and fall in sodium in patients who
developed hyponatraemia. It will be crucial to know whether this trend is
seen in the other patients also (those who did not develop significant
hyponatraemia), to test the hypothesis that fall in sodium is inversely
related to EFW. It may be possible to understand whether the group that
developed hyponatraemia is different from those who did not develop
hyponatraemia and we can then ‘focus on the inherent properties of the
patient’s physiology, rather than the inherent properties of the fluid
being used’ as suggested by Choong in the accompanying editorial(2).
References
1. Singhi S, Jayashree M. Free water excess is not the
main cause for hyponatremia in critically ill children receiving
conventional maintenance fluids. Indian Pediatr 2009; 46: 577–583.
2. Choong K. Should we add more salt, or less water. Indian Pediatr
2009; 46: 573-574.


