Critical Appraisal
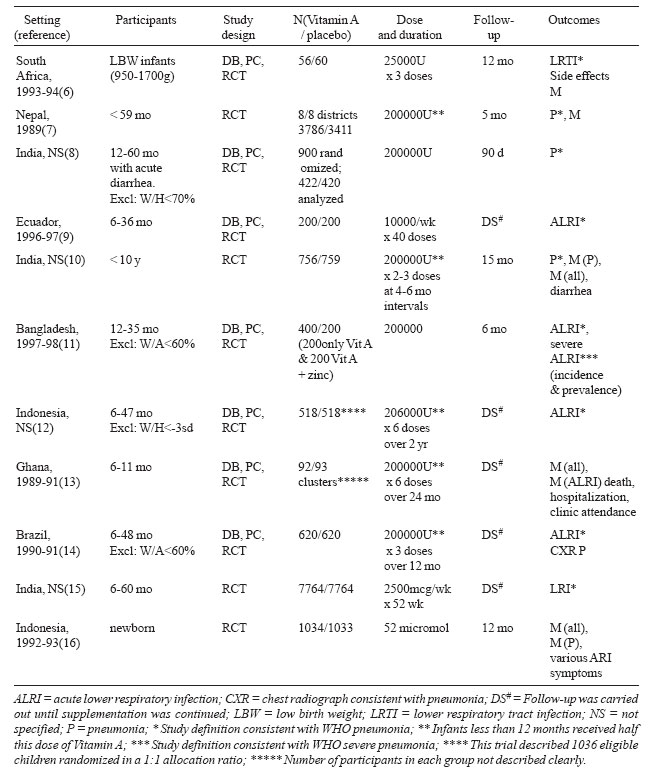
The 20 trials included in the two
components of this systematic review comprise
current best evidence from published literature.
However, only 1 of the 9 prophylaxis trials could be
classified as having low risk of bias(11), while
6(6,7,10,14,15,16) had high risk of bias owing to
inadequacies in two or more of the following
components: randomization, allocation concealment,
blinding, incomplete outcome reporting, and
selective outcome reporting. Five trials used serial
doses of vitamin A/ placebo, but did not carry out
follow-up beyond the period of
supplementation(9,12-15). Two trials did not specify
the sample size, necessitating indirect
calculations(12,13). Two trials did not use
definitions of pneumonia consistent with the WHO
definition, but contributed data on
mortality(13,16).
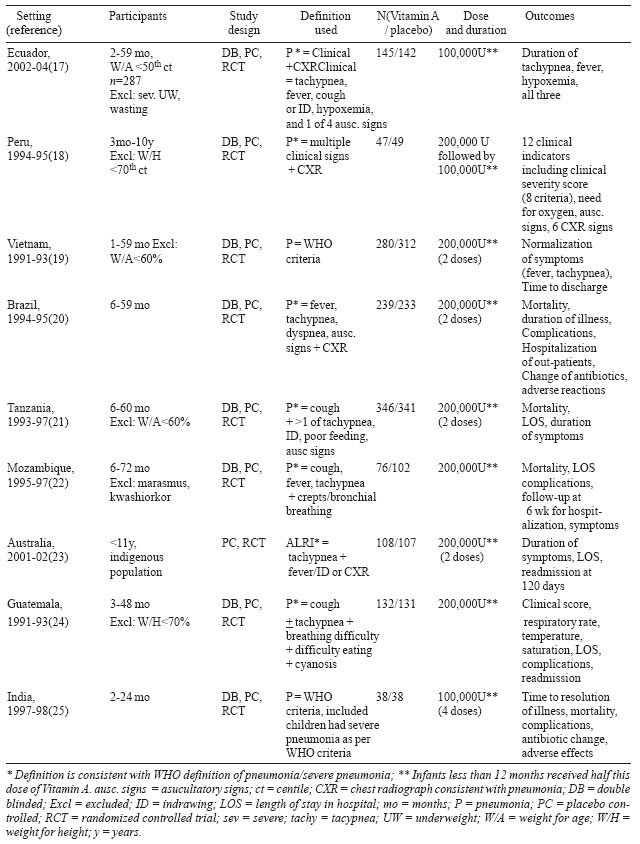
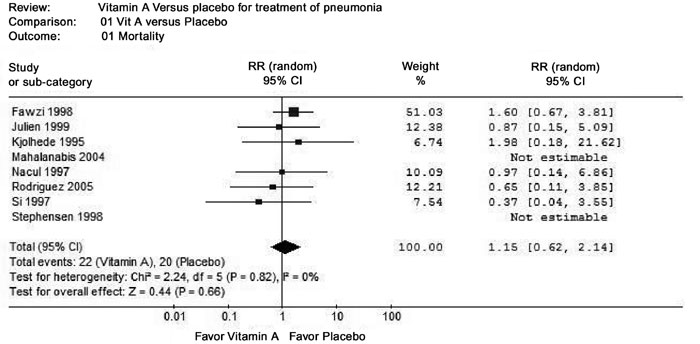
Seven of the nine therapy trials
could be categorized as having low risk of
bias(18-20,22, 24-25); two trials(17,21) had missing
components affecting the quality grading. A variety
of outcomes were measured in these trials, from
which some data could be extracted for
meta-analysis.
Some trials undertaking post-hoc
sub-group analysis suggest that vitamin A could be
beneficial in children with pre-existing vitamin A
deficiency (determined by low serum retinol) and/or
severe malnourished status. There is also data
suggesting that supplementation could harm those
with adequate baseline levels of serum retinol. This
coupled with the fact that children with biochemical
deficiency cannot be identified clinically; suggest
that the first observation has little practical
application. Since only 4 of 11 prophylaxis trials
and 2 of 9 therapy trials did not exclude severely
malnourished children, data on the second
observation is too limited to draw definite
conclusions. Therefore, neither issue has been
explored further in this EURECA.
Extendibility
All the included trials were
conducted in developing country populations; the
lone developed country trial included Australian
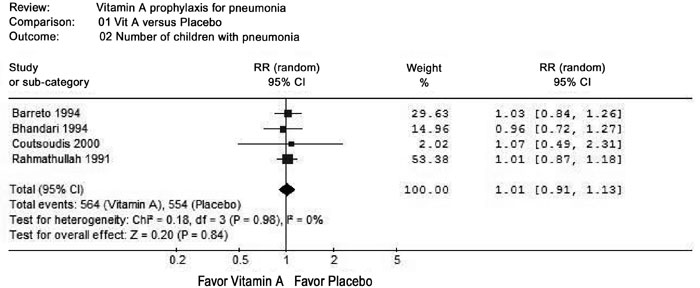
indigenous children. The fact that 5 prophylaxis
trials and 1 therapy trial were conducted in the
Indian sub-continent strengthens confidence in
extendibility and applicability of the findings that
vitamin A supplementation has no role from the
perspective of childhood pneumonia.
Funding: None.
1. Bhutta ZA, Ahmed T, Black RE,
Cousens S, Dewey K, Giugliani E, et al. What
works? Interventions for maternal and child
undernutrition and survival. Lancet 2008; 371:
417-440.
2. de Benoist B, Martines J,
Goodman T. Vitamin A supplementation and the control
of vitamin A deficiency: Conclusions. http://www.who.int/nutrition/publications/micronutrients/FNBvol22N3sep01.
pdf accessed on 27 January, 2010.
3. No authors listed. WHO
Guideline Development: Effects and Safety of Vitamin
A Supplementation in Populations. http://www.who.int/nutrition/events/guideline_dev_vas/en/.
Accessed on 19 January 2010.
4. Chen H, Zhuo Q, Yuan W, Wang
J, Wu T. Vitamin A for preventing acute lower
respiratory tract infections in children up to seven
years of age. Cochrane Database Syst Rev 2008; 1:
CD006090
5. Ni J, Wei J, Wu T. Vitamin A
for non-measles pneumonia in children. Cochrane
Database Syst Rev 2005; 3: CD003700
6. Coutsoudis A, Adhikari M,
Pillay K, Kuhn L, Coovadia HM. Effect of vitamin A
supplementation on morbidity of low-birth-weight
neonates. S Afr Med J 2000; 90: 730-736.
7. Daulaire NM, Starbuck ES,
Houston RM, Church MS, Stukel TA, Pandey MR.
Childhood mortality after a high dose of vitamin A
in a high risk population. BMJ 1992; 304: 207-210.
8. Bhandari N, Bhan MK, Sazawal
S. Impact of massive dose of vitamin A given to
preschool children with acute diarrhoea on
subsequent respiratory and diarrhoeal morbidity. BMJ
1994; 309: 1404-1407.
9. Sempértegui F, Estrella B,
Camaniero V, Betancourt V, Izurieta R, Ortiz W, et
al. The beneficial effects of weekly low-dose
vitamin A supplementation on acute lower respiratory
infections and diarrhea in Ecuadorian children.
Pediatrics 1999; 104: e1-e7.
10. Chowdhury S, Kumar R, Ganguly
NK, Kumar L, Walia BN. Effect of vitamin A
supplementation on childhood morbidity and
mortality. Indian J Med Sci 2002; 56: 259-264.
11. Rahman MM, Vermund SH, Wahed
MA, Fuchs GJ, Baqui AH, Alvarez JO. Simultaneous
zinc and vitamin A supplementation in Bangladeshi
children: randomised double blind controlled trial.
BMJ 2001; 323: 314-318.
12. Dibley MJ, Sadjimin T,
Kjolhede CL, Moulton LH. Vitamin A supplementation
fails to reduce incidence of acute respiratory
illness and diarrhea in preschool-age Indonesian
children. J Nutr 1996; 126: 434-442
13. Ghana VAST Study Team.
Vitamin A supplementation in northern Ghana: effects
on clinic attendances, hospital admissions, and
child mortality. Lancet 1993; 342: 7-12.
14. Barreto ML, Santos LM, Assis
AM, Araújo MP, Farenzena GG, Santos PA, et al.
Effect of vitamin A supplementation on diarrhoea and
acute lower-respiratory-tract infections in young
children in Brazil. Lancet 1994; 344: 228-231.
15. Rahmathullah L, Underwood BA,
Thulasiraj RD, Milton RC. Diarrhea, respiratory
infections, and growth are not affected by a weekly
low-dose vitamin A supplement: a masked, controlled
field trial in children in southern India. Am J Clin
Nutr 1991; 54: 568-577.
16. Humphrey JH, Agoestina T, Wu
L, Usman A, Nurachim M, Subardja D, et al.
Impact of neonatal vitamin A supplementation on
infant morbidity and mortality. J Pediatr 1996; 128:
489-496.
17. Rodríguez A, Hamer DH, Rivera
J, Acosta M, Salgado G, Gordillo M, et al.
Effects of moderate doses of vitamin A as an adjunct
to the treatment of pneumonia in underweight and
normal-weight children: a randomized, double-blind,
placebo-controlled trial. Am J Clin Nutr 2005; 82:
1090-1096.
18. Stephensen CB, Franchi LM,
Hernandez H, Campos M, Gilman RH, Alvarez JO.
Adverse effects of high-dose vitamin A supplements
in children hospitalized with pneumonia. Pediatrics
1998; 101: E3-E10.
19. Si NV, Grytter C, Vy NN, Hue
NB, Pedersen FK. High dose vitamin A supplementation
in the course of pneumonia in Vietnamese children.
Acta Paediatr 1997; 86: 1052-1055.
20. Nacul LC, Kirkwood BR, Arthur
P, Morris SS, Magalhães M, Fink MC. Randomised,
double blind, placebo controlled clinical trial of
efficacy of vitamin A treatment in non-measles
childhood pneumonia. BMJ 1997; 315: 505-510.
21. Fawzi WW, Mbise RL, Fataki MR,
Herrera MG, Kawau F, Hertzmark E, et al.
Vitamin A supplementation and severity of pneumonia
in children admitted to the hospital in Dar es
Salaam, Tanzania. Am J Clin Nutr 1998; 68: 187-192.
22. Julien MR, Gomes A, Varandas
L, Rodrigues P, Malveiro F, Aguiar P, et al.
A randomized, double-blind, placebo-controlled
clinical trial of vitamin A in Mozambican children
hospitalized with nonmeasles acute lower respiratory
tract infections. Trop Med Int Health 1999; 4:
794-800.
23. Chang AB, Torzillo PJ, Boyce
NC, White AV, Stewart PM, Wheaton GR, et al.
Zinc and vitamin A supplementation in Indigenous
Australian children hospitalised with lower
respiratory tract infection: a randomised controlled
trial. Med J Aust 2006; 184: 107-112.
24. Kjolhede CL, Chew FJ,
Gadomski AM, Marroquin DP. Clinical trial of vitamin
A as adjuvant treatment for lower respiratory tract
infections. J Pediatr 1995; 126: 807-812.