|
|
Case Reports Indian Pediatrics 2007;44:226-228 |
||
|
Hepatic Abscess in a Preterm Neonate |
||
|
Shailesh Sharma
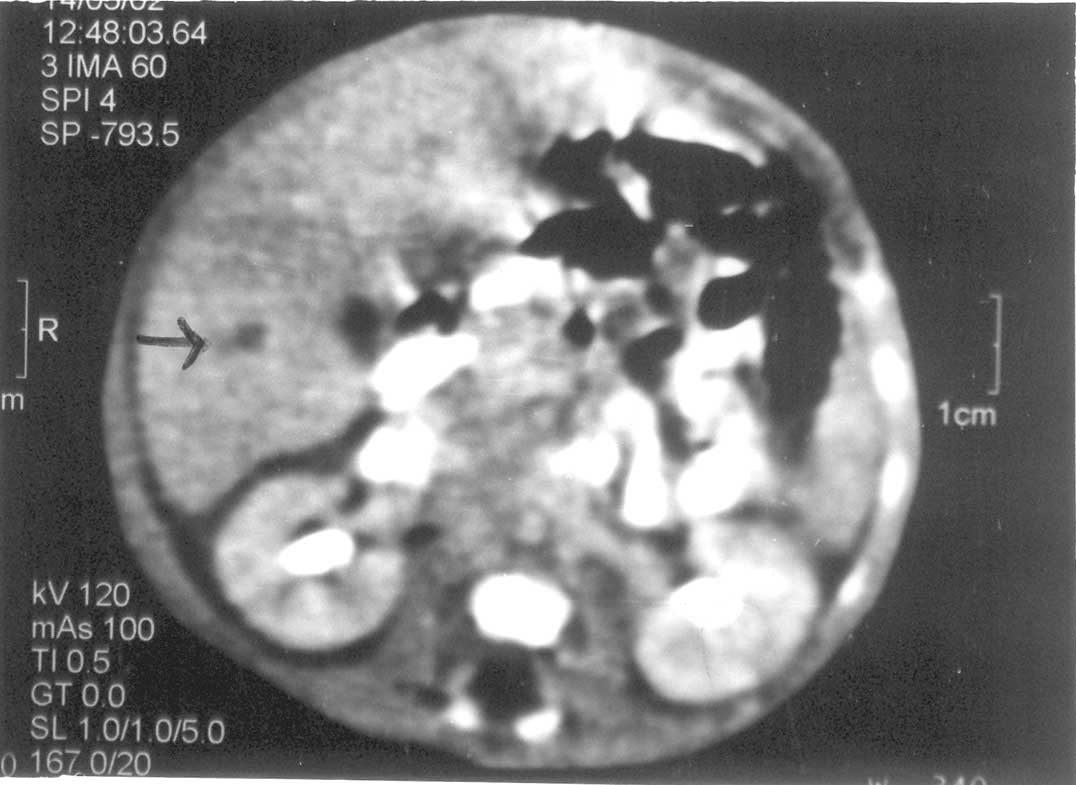
Abstract: Key words: Hepatic abscess, Klebsiella, Neonate. Hepatic abscess is rare in the neonatal period, and usually not taken into consideration in the differential diagnosis of obscure masses in the upper abdomen. Case Report A preterm, 32 weeks, appropriate for gestational age baby with birth weight of 1300 g was delivered vaginally to a primigravida. Apgar scores at 1 and 5 minutes were 8 and 9 respectively. The mother had leaking per vaginum for more than 12 hrs prior to delivery. The neonate was referred to our hospital at 36 hours of life in a stable state. Initial investigations including septic work up were normal. Nasogastric feeding was introduced on day 4 of life and increased over the subsequent days. The child developed abdominal distension with bilious aspirates and decreased bowel sounds on day 9. Enteral feeding was discontinued. The liver was enlarged, 3 cm below costal margin, firm, smooth surface with well defined margins. Another lump was palpated in the right hypochondrium 5 × 6 cm, firm, smooth, immobile and was felt separately from the liver. Investigations revealed Hb = 10.8 g/dL, TLC=11,900 mm3, platelet count = 58,000 per mm3; micro ESR=10 mm, peripheral smear revealed toxic granules, arterial blood gas analysis was normal and blood culture showed a pure growth of Klebsiella species sensitive to cipro-floxacin and amikacin. Amebic serology was non reactive. Ultrasonography was inconclusive about the character of the lump; CT of the abdomen revealed a cystic mass in the liver (Fig.1). The character of the lump outside the liver could not be commented but revealed leakage of the dye from the terminal ileum. On day 12, exploratory laprotomy under general anesthesia was done. At surgery, small bowel was seen to be adherent to the under surface of right lobe of liver. On separation, a perforation of 7mm size was seen in terminal ileum. Right lobe of liver had a large abscess filled with organized pus that was evacuated. There was no bilious leak from the raw surface of abscess cavity. Rest of the abdomen was normal without any evidence of peritonitis. Bowel perforation was closed and abscess cavity was drained. The infant was put on injection vancomycin, ceftriaxone and metro-nidazole, which were changed to ciprofloxacin and amikacin after the culture reports. The post operative period was uneventful. Serial USG of the abdomen after 7 days showed that the size of the abscess had reduced to 1.7 × 1.9 × 1.6 cm. The child was discharged after 6 week.
Discussion The first review of liver abscess appeared in 1936 by Kutsunak(1) who reported 2 infants with fatal peritonitis with solitary liver abscess at necropsy. Since then, about 50 cases of solitary neonatal liver abscess have been reported(2). Of the the 18 cases reviewed by Doerr, et al.(3) nine patients survived. Four of the survivors were preterm and low birth weight and had a history of umbilical venous catheterization. One of the survivors, 2.2 kg, 34 wks, developed solitary hepatic abscess as a delayed complication of neonatal bacteremia(4). Another 6 cases of neo-natal liver abscess were reported by Tan, et al(5). Infection of the liver in the neonate differs from that in the older children in that opportunistic and parastic infections are unusual. Congenital tuberculosis, congenital syphilis, and listeriosis have been reported as etiological causes(1). The hepatic abscess can be either multiple or solitary. Multiple liver abscess as the name suggests are multiple, small in size, not drainable, usually not due to umbilical infection and have a fulminant course. Whereas, solitary liver abscess are larger, well localized, can be drained by surgical methods, usually due to multiple infection and have a subacute course. There can be multiple routes of infection to liver(6). It can be direct invasion via contagious structure or hepatic artery through systemic circulation or portal vein via umbilical vein, mesenteric or splenic vein. Lymph channels along with umbilical vessels can also contribute. Major risk factors for hepatic abscess are sepsis, umbilical catheterization and omphalitis(7). Minor risk factors include necrotizing enterocolitis, abdominal surgery, maternal infections, infant of diabetic mother, gastroschisis requiring surgery, exchange transfusion, VP shunt and asphyxia neonatorum. The classical presentation of liver abscess with fever, hepatomegaly and right upper abdominal pain is generally not present in neonates. The diagnosis of liver abscess in the neonate cannot be established from the clinical picture alone. The signs and symptoms are nonspecific and are essentially those of sepsis(6). In one of the reports, out of the 24 reported case of neonates with solitary hepatic abscess the diagnosis was made at necropsy in 75%(1,7). Both the rarity of solitary hepatic abscess in the neonate and its indolent course require a high index of suspicion for early diagnosis(4). In our case also, the correct diagnosis was delayed until an exploratory laprotomy was performed. Abdominal ultrasonography, CT scan, liver scan with technetium are all useful studies to visualise a possible hepatic abscess(6). However, in our patient abdominal USG and CT scan were inconclusive and revealed just the leakage of dye from terminal ileum. Staphylococcus aureus, Streptococcus pyogenes and E. coli are the most common organisms isolated from solitary hepatic abscess in neonates(8). However, Klebsiella, Pseudomonas, Corynebacterium acnes, anaerobes and even Candida have been reported(9). Polymicrobial infection is found in up to 50% of infants(3). Early surgical exploration, adequate drainage and adjunctive antimicrobial therapy led to a favorable outcome in this preterm, VLBW neonate. Contributors: All authors contributed to case management, review of literature and drafting of the article. Funding: None. Competing interests: None stated. | ||
|
References | ||
|
|
![]()