The non-medical use of chemical substances in
order to achieve alterations in psychological functioning has been
termed as substance use(1). WHO estimates that globally, 25% to 90%
of street children indulge in substance use(2). According to UNICEF,
there are more than 5,00,000 street children in India(3) who live
and work in inhuman conditions(4) and are at high risk of substance
use(4-6). Knowledge of extent of the problem and socio-demographic
risk factors is essential to devise effective preventive strategies
against substance use. The present study was designed to know the
magnitude of substance use and its risk factors among a group of
street children in Delhi.
Methods
The study was conducted in an observation home
for boys in Delhi that provides temporary shelter to children in
need of protection. These children are mainly homeless street
children.
A pilot study was conducted on 30 inmates of the
observation home in January 2002 in which the substance use rate was
found to be 50%. At 10% allowable error, the sample size was
calculated as 100. Based on the admission rate of 25 children per
month, it was estimated that about 125 boys would be available for
study in 5 months, allowing an attrition rate of 20%.
All the boys between 6-16 years who were brought
to the observation home between February to June 2002 were included.
At admission, the boys underwent psychological screening and IQ
testing whenever required by trained psychologists. The criteria for
exclusion were (a) mental retardation defined as IQ £70 (b)
inability of the subject to understand either Hindi or English.
The age of the child was taken from the official
records and was determined by the Juvenile Welfare Board at the time
of admission. The study tools consisted of a self-developed,
semi-structured questionnaire about child’s social and demographic
back-ground. This questionnaire was pretested on 30 inmates of the
observation home in January 2002 and suitably modified. The study
subjects were interviewed regarding substance use anytime before
coming to observation home and the knowledge of its harmful effects.
The informed written consent of the observation home authorities was
obtained.
Statistical Methods
For data entry, EPI-INFO version 2000 was used.
Chi-square test and Fishers’ exact test were applied to detect any
significant association. Odds ratios were also calculated.
Multivariate analysis was done using binomial logistic regression
and adjusted odds ratios were calculated using SPSS 7.5 version. P
value less than 0.05 was considered as statistically significant.
Results
Out of the 130 boys admitted to observation home
during the study period, 10 (7.7%) were excluded due to mental
retardation, (n = 4, 3.1%) and their inability to understand either
Hindi or English (n = 6, 4.6%). Of the remaining 120, five (4.2%)
refused to give consent. The final sample consisted of 115 boys aged
between 6 to 16 years.
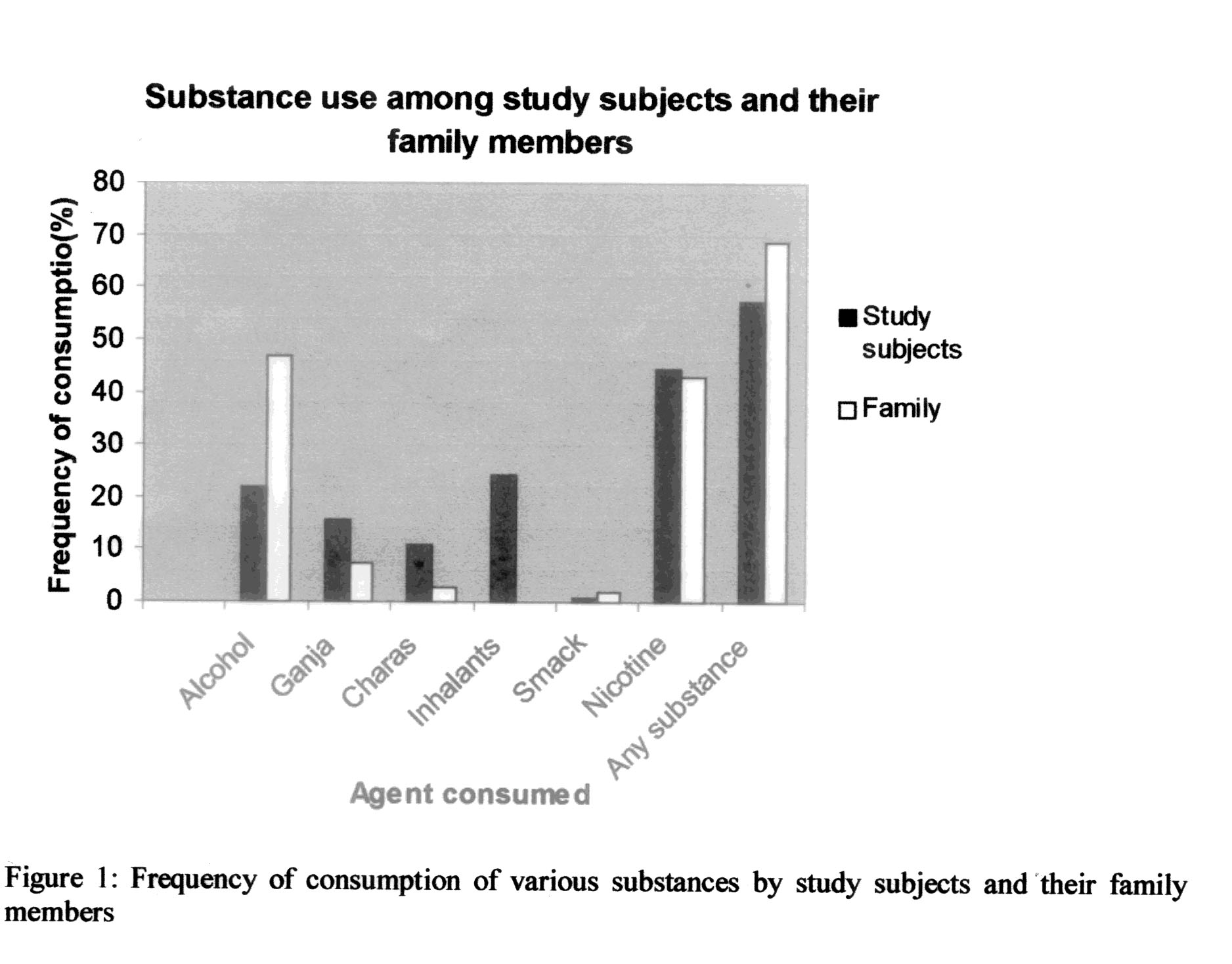
Table I shows the socio-demographic
characteristics of study subjects. Majority had runaway from homes.
The average age of leaving home was 9.1 years. A total of 68.7%
subjects reported substance use in their family (Fig. 1)
among whom 86% reported substance use by the father.
Risk factor
|
Substance use (%)
N = 155
|
Odds ratio
(95% CI)
|
P value
|
Place of origin
|
|
0.56
|
|
|
Rural
|
25 (21.7)
|
|
|
Urban
|
41 (35.7)
|
Nuclear Family
|
49(42.6)
|
2.6(1.1,6.7)
|
0.03
|
Death of father
|
12(10.4)
|
–
|
0.59
|
Death of mother
|
14(12.2)
|
|
0.85
|
Presence of step parents
|
11(9.6)
|
–
|
0.10
|
Domestic violence
|
48 (41.7)
|
2.46 (1.04, 5.87)
|
0.04
|
Maltreatment at home
|
40 (34.8)
|
4.5 (1.9, 10.7)*
|
0.0002
|
Runaway from home
|
57 (49.6)
|
3.08 (1.04, 9.4)
|
0.04
|
Substance use in family
|
50 (43.5)
|
|
0.13
|
Working children
|
60 (52.2)
|
3.7 (0.8, 19.4)
|
0.04
|
*Adjusted odds ratio = 4.7 (95% CI: 2.1, 10.4)
Substance use in children
Among the children interviewed, 57.4% (n = 66)
had indulged in substance use any time in their life. The minimum
age at starting substance use in our study was 5.5 years. The most
common substance consumed was nicotine, as cigarettes or "bidis’ and
"gutkha" (Fig. 1). Inhalant / volatile substance use in the
form of sniffing of adhesive glue, petrol, gasoline, thinner and
spirit was reported by one fourth of children. Twenty per cent of
children reported having sold cigarettes; "bidi" and "gutkha" while
2.5% had been anytime employed in preparation of "charas"
cigarettes.
The harmful effects of substance use named by
children were lung problems (28.2%) like "burning of lungs" and
tuberculosis (6%), some stomach ailment like stones, rupture and
bloody vomiting (12%), cancer (10.9%), death (10%), blackening of
teeth and rupture of cheeks (7.3%), closing of heart or kidney
stones (5%). Thirty per cent denied any knowledge about this issue.
Risk factors for substance use among study
subjects
The results of univariate analysis are shown in
Table 1. Substance use was significantly associated with
domestic violence, maltreatment of the child, nuclear families,
running away from home, and working status of the child. The rural
or urban origin, native state, age of the child and his literacy
level were not significantly associated with substance use.
Multiple logistic regression was applied taking
Substance use as dependent variable and domestic violence,
maltreatment, nuclear family, runaway status and working status as
independent covariates. After regression analysis, maltreatment of
the child was the only variable that reached significant value (Table
I).
It was noted that the knowledge of harmful
effects was more among children who had indulged in substance use
but there was no statistically significant difference. The older
children (11 to 16 years) had more knowledge than younger children
(p >0.05). Children revealed that this knowledge was based on their
own experiences and the information provided by their parents, by
peer group and during health education classes organized by some
voluntary organizations.
Discussion
A sizable proportion (over 50%) of children
coming to observation homes were found to indulge in substance use.
The fact that children had access to a large variety of intoxicating
substances, reflected ineffective implementation of the existing
legislations, namely the Narcotics and Psychotropic Substances Act,
1985 and The Delhi Anti-Smoking and Non-Smoking Health Protection
Act, 1996(7). A study on street children in Bombay, Calcutta, Delhi
and Hyderabad also revealed high rates of substance use among
runaway boys(4).
Running away exposes children to stressful life
on streets, which accompanied by lack of parental care and
supervision and easy access to intoxicating substances, creates an
atmosphere conducive for indulging in substance use. Maltreatment of
the child emerged as the only significant predictor (adjusted OR =
4.7) of substance use in the present study. The results are similar
to other studies(8-10).
The knowledge of harmful effects did not deter
children from indulging in substance use. This factor needs
consideration while devising preventive interventions against
substance use.
It was found that substance use in the family did
not increase the risk of substance use in children. This finding is
different from other studies(1,11). The most common agents consumed
were nicotine and alcohol. Other workers have also reported similar
findings(9, 12).
The present study has some limitations. The
results are based on the information given by children, who may have
underreported because of social stigma attached to consumption of
intoxicating substances. Also, information about the frequency,
regularity and duration of consumption was not available to allow
identification of physical or psychological drug dependence. The
results at best give an estimate of substance use patterns.
The observation home authorities should use the
period of detention of children to implement focused preventive
interventions against substance use. This may involve early
diagnosis, treatment and rehabilitation of substance dependants, and
counseling of parents at the time of family restoration of child
regarding long term effects of maltreatment of children.
Acknowledgements
The authors gratefully acknowledge Dr. Pranay
Bhanu, Medical officer and staff of "Prayas" observation home for
boys, New Delhi, Ms Nirmata Kureel, Mrs Govil and the interns from
the batch of 2002, Maulana Azad Medical College, for their active
support and co-operation for this research.
Contributors: DP developed the concept and
design of the study, collected the data, analyzed, interpreted the
data and wrote the draft and final paper. GSM revised the draft and
gave approval of the version to be published. MMS helped in
conceptualizing and designing the study, analysis and interpretation
of the data, drafting and revising the article. RS helped in
statistical analysis and interpretation of data.
Conflict of interest: None stated.
Funding: None.
