|
|
|
Indian Pediatr 2017;54: 514-515 |
 |
Hepatitis A with Superadded Salmonella
paratyphi A Infection Presenting with Exudative Pleural
Effusion and Acalculous Cholecystitis
|
|
*Aniruddha Ghosh and Pavel Kundu
Department of Pediatric Medicine, Institute of Child
Health, Kolkata, India.
Email: [email protected]
|
|
Both hepatitis A and enteric fever are major public health problems in
developing countries [1,2]. Transudative pleural effusion and ascites
have been reported in hepatitis A but rare in enteric fever [3-5].
A 4-year-old girl presented to us with fever for 15
days along with jaundice, cough and dyspnea. Since day-8 of fever, child
had multiple petechial rashes all over the body. There was no history of
blood transfusion, intravenous drug use, tick bite, or contact with
tuberculosis. There was no history of MMR, Hepatitis A, Hepatitis B or
Typhoid vaccination. Chest examination revealed stony dull percussion
note anteriorly over right side of chest starting from 2 nd
intercostal space downwards in mid clavicular line with absent breath
sounds. Abdomen was distended, and there was tender hepatomegaly and
mild splenogmegaly. Other system examination was normal.
Investigation showed anemia (Hb 8.3 g/dL), elevated
C-reative protein (36.1 mg/L), and deranged liver function tests (total
bilirubin 5.6 mg/dL, direct bilirubin 5.5 mg/dL, alanine
aminotransferase 366 U/L, aspartate aminotransferase 256 U/L, gamma
glutamyl transferase- 359 U/L, Alkaline phosphatase 787 U/L); child also
had coagulopathy (INR = 1.92).
 |
|
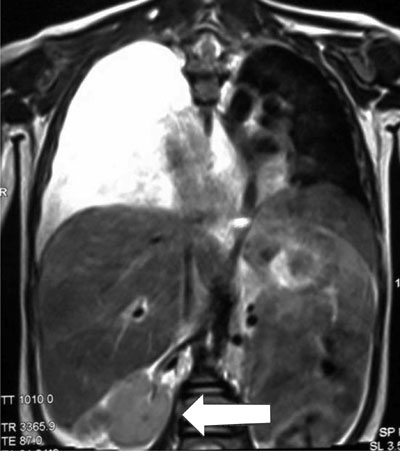
Fig.1 Magnetic resonance imaging
coronal view showing massive right sided pleural effusion and
hyperintensity in gall bladder area with thickened wall (arrow)
indicative of acalculous cholecystitis.
|
Chest radiograph revealed opacity involving lower and
middle zone of right lung with a sharp convex upper border without
mediastinal shift. MRI of chest and abdomen (Fig. 1) showed
massive pleural effusion with collapsed lobes of right lung,
hepatosplenomegaly and hyperintense gall bladder with thickened wall
suggestive of acalculous cholecystitis. IgM for Hepatitis A was
reactive. Tests for other hepatotropic organisms and tuberculosis
yielded negative results. Intravenous vitamin K was administered. A
diagnostic pleurocentesis revealed exudative pleural effusion; culture
did not reveal any growth. Widal test was positive ((T(O) 1:160,
A(H)-1:320)) and blood culture demonstrated Salmonella paratyphi
A. Intravenous cefotaxime (200 mg/kg/day) was administered, and after 3
days, the patient became afebrile; distress also decreased considerably
and before discharge, repeat LFT showed improvement. Child was
discharged with oral cefixime (20 mg/kg/day). Chest X-ray showed
clearance of fluid during one week follow-up. The patient was doing well
after a follow-up of two months.
Exudative pleural effusion in viral hepatitis should
be investigated to rule out other coinfections.
References
1. Hunter PR, MacDonald AM, Carter RC. Water supply
and health. PLoS Med. 2010;7:e1000361.
2. Prüss A, Kay D, Fewtrell L, Bartram J. Estimating
the burden of disease from water, sanitation, and hygiene at a global
level. Environ Health Perspect. 2002;110:537-42.
3. Tesovic G, Vukelic D, Vukovic B, Benic B,
Bozinovic D. Pleural effusion associated with acute hepatitis A
infection. Pediatr Infect Dis J. 2000;19:585-6.
4. Erdem E, Urgancý N, Ceylan Y, Kara N, Ozcelik G,
Gulec SG. Hepatitis A with pleural effusion, ascites and acalculous
cholecystitis. Iran J Pediatr. 2010;20:479-82.
5. Huang DB, DuPont HL. Problem pathogens:
Extra-intestinal complications of Salmonella enterica serotype
Typhi infection. Lancet Infect Dis. 2005;5:341-8.
|
|
|
 |
|
