|
|
|
Indian Pediatr 2014;51: 463 -467 |
 |
Trier Social Stress Test in Indian
Adolescents
|
|
GV Krishnaveni, SR Veena, *A
Jones, #DS Bhat,
MP Malathi, $D
Hellhammer, **K
Srinivasan, H Upadya,
**AV
Kurpad, ##CHD
Fall
From Epidemiology Research Unit, CSI Holdsworth Memorial Hospital,
Mysore, India; *Centre for Cardiovascular Imaging, UCL Institute of
Child Health, London, UK; #Diabetes Unit, KEM Hospital
Research Centre, Pune, India;$Department of Psychology,
University of Trier, Germany; **St. John’s Research
Institute, Bangalore, India; and ##MRC Lifecourse
Epidemiology Unit, Southampton General Hospital, Southampton, UK.
Correspondence to: Dr GV Krishnaveni, Epidemiology Research Unit, CSI
Holdsworth Memorial Hospital, PO Box 38, Mandi Mohalla, Mysore 570 021,
India.
Email:
[email protected]
Received: September 27, 2013;
Initial review: November 19, 2013;
Accepted: March 20, 2014.
|
Objective: To test the Trier Social Stress Test for children
(TSST-C) in a cohort of Indian adolescents.
Design: Cohort study
Setting: Holdsworth Memorial Hospital, Mysore,
India.
Participants: Adolescent children (N=273,
134 males; mean age 13.6 yrs) selected from an ongoing birth cohort; 269
completed the test.
Intervention: Performance of 5-minutes each of
public- speaking and mental arithmetic tasks in front of two unfamiliar
‘evaluators’.
Outcome measures: Salivary cortisol
concentrations were measured at baseline and at regular intervals after
the TSST-C. Continuous measurements of heart rate, finger blood
pressure, stroke volume, cardiac output and systemic vascular resistance
were carried out before, during and for 10 minutes after the TSST-C
using a finger cuff.
Results: Cortisol concentrations [mean increment
(SD): 6.1 (6.9) ng/mL], heart rate [4.6 (10.1) bpm], systolic [24.2
(11.6) mmHg] and diastolic blood pressure [16.5 (7.3) mmHg], cardiac
output [0.6 (0.7) L/min], stroke volume [4.0 (5.6) mL] and systemic
vascular resistance [225 (282) dyn.s/cm5] increased
significantly (P<0.001) from baseline after inducing stress.
Conclusions: The TSST-C produces stress-responses
in Indian adolescents of a sufficient magnitude to be a useful tool for
examining stress physiology and its relationships to disease outcomes in
this population.
Keywords: Cortisol, Stress, Validation studies.
|
|
Repeated exposure to psychological stress may result
in adult-onset chronic diseases [1,2]. A deranged
hypothalamic-pituitary-adrenal axis (HPAA) response to stress, leading
to altered release of cortisol, and altered autonomic nervous system
activity resulting in cardiac-sympathetic dysfunction, are the major
factors determining this association. Individuals vary in
stress-responses, and, thus, in their risk susceptibility [2,3]. Higher
HPAA sensitivity in Indians may contribute to their high chronic disease
risk [4]. Studying stress-responses in relation to disease risk,
especially in younger individuals, may help to understand the underlying
mechanisms and to intervene early in the lifecourse. However, the
utility of the existing experimental psychological stressors in this
population is unknown.
The Trier Social Stress Test for children (TSST-C),
developed in Germany for European populations, is commonly used to study
stress-responses in children [5]. We aimed to determine whether TSST-C,
modified to suit local purposes, is useful for studying the HPAA and
cardiovascular stress-responses in Indian children.
Methods
Adolescent children were recruited from the Parthenon
birth cohort [6], which was established to study the effect of maternal
and developmental factors on offspring risk factors. 663 women attending
the antenatal clinic of Holdsworth Memorial Hospital (HMH), Mysore,
India delivered normal singleton babies during 1997-1998. At 13.5 years
of age, 273 of the 545 children available for follow-up were selected
from those living within Mysore (N=354) to achieve equal
representation from four birth weight categories (134 boys). Willing
families were approached in the chronological order of the children’s
date of birth until the target number was achieved.
Protocol (Web Fig. 1): The
robustness of a stress-module is assessed by its ability to induce
strong cortisol reactivity [7,8]. The TSST-C involves 5-minutes each of
public speaking and mental arithmetic tasks performed in front of an
evaluative panel. A perception of negative assessment of the
participants’ self image by others (social evaluative threat) has been
shown to trigger strong cortisol response [7-9].
We invited the cohort children for these tests as
part of a routine cardiovascular assessment. The details were given
before they confirmed participation. On the test morning, the children
underwent detailed anthropometry. The tests were conducted between 2.00
PM and 3.30 PM. A standard lunch was provided approximately 1½ hours
before the test to avoid postprandial variations in cortisol secretion.
Subsequently, they spent a relaxed time with their family. A baseline
(pre-test) salivary sample was collected 10 minutes before the test,
after they watched a calming video for 5 minutes in a standing position.
The children were tested individually. The
investigator explained the procedure to the child and gave 10 minutes to
prepare an imaginative story following a lead. The lead was modified
from the original to make it locally more identifiable (Web
Table I). He/she was then accompanied to the test room which
they had not seen previously, and was asked to stand in front of a
microphone, facing a video camera. A male and a female staff member,
previously unknown to the children, acted as ‘judges’. They indicated
that the child’s performance will be evaluated for its quality, and will
be video-recorded. The judges remained neutral throughout the test, and
did not give positive feedback or encouragement, by words or by gesture,
which was crucial to increase the stress-response.
First task consisted of public speaking (story). The
male judge asked the child to complete the story in free speech, lasting
5 minutes. If they spoke uninterruptedly, the judge tried to make the
situation more difficult (Web Fig. 1). If they remained
speechless, the judge gave prompts and hints to continue, as
disengagement from the task was likely to decrease the stress-response
[9]. Second task involved mental arithmetic (maths). The female
judge asked the child to serially subtract ‘3’ from ‘501’ as fast and
accurately as possible, for 5 minutes. Our pilot trials had shown that
this series enabled the children to give enough right answers to sustain
their interest, as well as having the scope for frequent errors. If they
made a mistake, they were asked to start again from the beginning. The
difficulty of the task was reduced or increased depending on the child’s
performance (Web Fig. 1,
Web Table I). It was
ensured that they looked at the panel continuously during these tasks,
by prompting if necessary. Tests were stopped immediately if the
children seemed upset.
Systolic and diastolic blood pressure (BP), cardiac
output, stroke volume, heart rate and systemic vascular resistance (SVR)
were measured continuously before, during and for 10 minutes after the
TSST-C by a non-invasive, portable hemodynamic monitoring system using
appropriately sized finger cuffs (Nexfin, BMeye, Amsterdam,
Netherlands). The beat-to-beat values were averaged over 5 minutes for
the pre-test video-viewing (baseline), story, maths, and immediate
post-stressor periods.
A salivary sample was collected at the end of the
tasks. The judges commended the children for their performance. Children
joined their family members in a separate room subsequently, but there
was no contact with the untested children or their companions. Further
samples were taken at 10, 20, 30 and 60 minutes after the TSST-C to
measure the cortisol response. Another calming video was played before
the final salivary sample was collected. The samples were then
transferred to a –20 0 C
freezer. The children remained standing for 10 minutes after the TSST-C
and during post-test video-viewing to make the conditions uniform with
the test period.
All participants returned the next day for detailed
cardiometabolic investigations, including blood sampling. The pubertal
status was assessed using Tanner’s method [10], and was classified as
the stage of breast development (girls) or genital development (boys).
The socio-economic status (SES) of the family was determined using the
Standard of Living Index designed by the National Family Health Survey-2
[11].
The HMH ethics committee approved the study; informed
written consent from parents and assent from children were obtained.
Cortisol assay: Salivary samples were thawed and
centrifuged at the end of the study. The supernatant liquid was stored
at -20 0 C before sending it
for analysis at KEM Hospital Research Centre, Pune, on dry ice. The
samples were thawed and centrifuged again and the supernatant was
transferred to new vials in Pune before assaying. Cortisol
concentrations were measured using an ELISA method (Alpco Diagnostics,
Salem, NH) as per the manufacturer’s instructions. All samples from a
child were analyzed in the same batch. Standard curves were established
for each run, based on the calibrators provided by the manufacturer
(range:1-100 ng/mL). High and low controls were included with each run
to ensure quality control. The assay sensitivity was 1 ng/mL; inter- and
intra-assay coefficients of variation were 10% and 6.6%, respectively.
Statistical methods: Salivary cortisol
concentrations were log-normalized for analyses. The cortisol
stress-response was calculated by subtracting the pre-test value from
the post-stress values. The cardiovascular stress-response was
calculated as the difference between the pre-test and the TSST-C
averages. Differences between boys and girls in cortisol and
cardiovascular parameters was analyzed using independent t-tests. Paired
t-tests were used to analyze the difference between baseline and the
post-stressor values.
Results
Two children refused to perform in front of the
judges and the test was stopped in two other children as they were
upset; the TSST-C was completed in 269 children. Adequate pre- and
post-test salivary samples were available for 266 children and complete
cardiovascular responses were available in 249 children. None of the
participants reported negative after-effects of stress, and all returned
for blood sampling the next day.
In general, girls were heavier than boys, and had
higher heart rate, while boys had greater stroke volume at baseline (Table
I). There was no difference in baseline cortisol concentrations
between boys and girls.
TABLE I General Characteristics, and Cortisol and Cardiovascular Profile in The Study Subjects
|
All (N=273)** |
Boys (n=134) |
Girls (n=139) |
P# |
|
Age (yr) |
13.6 (0.2) |
13. 6 (0.2) |
13.6 (0.1) |
0.5 |
|
Height (cm) |
154.2 (7.0) |
154.7 (8.2) |
153. 7 (5.7) |
0.2 |
|
BMI (kg/m2) |
17.8 (2.9) |
17.0 (2.4) |
18.6 (3.1) |
<0.001 |
|
Pubertal stage (N) 2 |
22 (8.0%) |
3 (2.3%) |
19 (13.9%) |
|
|
3 |
109 (41.0%) |
33 (25.6%) |
76 (55.5%) |
|
|
4 and 5 |
135 (50.8%) |
93 (72.1%) |
42 (30.7%) |
<0.001 |
|
Obesity/overweight (N) |
34 (12.5%) |
10 (7.5%) |
24 (17.3%) |
0.01 |
|
Baseline |
|
Cortisol concentrations (ng/mL)* |
6.6 (4.9,9.0) |
6.8 (4.7,8.9) |
6.6 (5.2,9.1) |
0.97 |
|
Systolic BP (mmHg) |
100.7 (11.7) |
101. 3 (11.7) |
100.1 (11.6) |
0.4 |
|
Diastolic BP (mmHg) |
69.3 (7.7) |
70.3 (8.2) |
68.5 (7.2) |
0.07 |
|
Heart rate (bpm) |
106.4 (12.2) |
104.4 (11.2) |
108.7 (12.8) |
0.005 |
|
Cardiac output (L/min) |
4.6 (0.8) |
4.6 (0.8) |
4.5 (0.8) |
0.2 |
|
Stroke volume (mL) |
43.6 (7.9) |
45.0 (7.4) |
42.1 (8.2) |
0.004 |
|
SVR ( dyn.s/cm5) |
1492 (225) |
1486 (233) |
1499 (218) |
0.7 |
|
Post-stress cortisol concentrations (ng/mL)*$
|
|
0-min
|
9.0 (5.9,14.1) |
9.2 (5.9,14.5) |
8.8 (5.9,14.0) |
0.6 |
|
10-min
|
12.2 (7.9,18.9) |
12. 0 (7.9,19.6) |
12.4 (8.2,18.5) |
0.6 |
|
20-min
|
12.9 (8.3,20.7) |
13.4 (8.2,21.2) |
12.5 (8.7,20.7) |
0.7 |
|
30-min
|
11.9 (8.1,18.8) |
11.9 (7.7,18.7) |
12.0 (8.1,19.2) |
0.6 |
|
60-min
|
8.7 (6.2,12.3) |
9.1 (6.4,12.9) |
8.3 (6.1,12.0) |
0.5 |
|
TSST-C cardiovascular parameters-story$ |
|
Systolic BP (mmHg) |
125.0 (15.9) |
123.4 (16.5) |
126.7 (15.2) |
0.1 |
|
Diastolic BP (mmHg) |
85.9 (9.7) |
85.8 (10.2) |
86.1 (9.2) |
0.8 |
|
Heart rate (bpm) |
109.8 (14.3) |
104.7 (11.5) |
115.0 (15.1) |
<0.001 |
|
Cardiac output (L/min) |
5.2 (0.9) |
5.0 (0.9) |
5.4 (0.9) |
<0.001 |
|
Stroke volume (mL) |
47.8 (8.4) |
47.8 (8.1) |
47.7 (8.8) |
0.9 |
|
SVR (dyn.s/cm5) |
1748 (393) |
1829 (426) |
1666 (338) |
0.001 |
|
TSST-C cardiovascular parameters-Maths$ |
|
Systolic BP (mmHg) |
124.8 (16.0) |
124.0 (16.5) |
125.6 (15.5) |
0.4 |
|
Diastolic BP (mmHg) |
85.7 (10.4) |
86.2 (10.8) |
85.2 (10.0) |
0.5 |
|
Heart rate (bpm) |
112.3 (14.5) |
108.0 (12.1) |
116.8 (15.5) |
<0.001 |
|
Cardiac output (L/min) |
5.3 (0.9) |
5.1 (0.9) |
5.4 (0.9) |
0.004 |
|
Stroke volume (mL) |
47.5 (8.6) |
47.6 (8.1) |
47.3 (9.0) |
0.8 |
|
SVR (dyn.s/cm5) |
1682 (359) |
1760 (402) |
1604 (290) |
0.001 |
|
Values given are mean (SD) or *geometric mean (IQR); SVR:
Systemic Vascular Resistance; #P value for the
difference between boys and girls using independent t-tests;
$P<0.001 for differences between baseline and
post-test values in all children using paired-t tests. **
n= 266 for pubertal stage, and baseline and past-stress cortisol
concentrations; N=249 for all TSST – C parameters. |
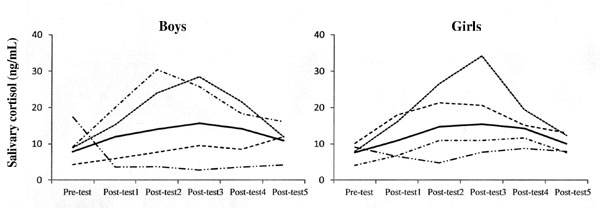
Cortisol concentrations increased consistently after
inducing stress in all, except in 13 children in whom the concentrations
decreased (Fig. 1). The mean (SD) increment from baseline
was statistically significant [6.1 (6.9) ng/mL; Table I].
Cortisol responses were similar in boys and girls (P=0.5). More
advanced puberty was associated with lower responses in girls (P=0.04),
but not in boys (P=0.8). Girls who had attained menarche had
significantly lower cortisol response than pre-menarchal girls (5.6
vs 9.9 ng/mL, P=0.02).
 |
|
Time of sampling relative to stressor
Solid line: mean cortisol response in all
children; dashed lines: individual responses in selected
children to show variability in stress-response
Fig. 1 Stress-induced cortisol
response in the study subjects.
|
Mean values for cardiovascular parameters increased
significantly from baseline during story and mental arithmetic tasks (Table
I). The responses were greater in girls than boys for systolic BP,
heart rate, cardiac output and stroke volume and less for SVR. In both
sexes, more advanced puberty was associated with lower heart rate and
cardiac output during TSST-C (P<0.05). The menarchal status in
girls was not associated with cardiovascular responses.
There was no association between SES and cortisol and
cardiac responses to stress. The stress-responses were similar in
obese/overweight children and those with normal BMI.
Discussion
This study, conducted to test the effectiveness of
using a well-known European stress test in Indian adolescents, showed
that both endocrine and cardiovascular stress responses of a similar
magnitude to those seen in other populations can be stimulated in Indian
conditions. There were no residual negative psychological effects of the
stressor.
A major limitation was that our study was conducted
only in urban children. As the cognitive performance was better in our
urban children cohort than rural children [12], their orientation
towards a stressful situation may also have differed. Thus, our findings
may not be applicable to the rural population. Another limitation was
that we did not know about any background stresses in the children’s
lives, which may have influenced their stress-responses.
This is the first time that the TSST-C has been used
to study stress-responses in India. The children tolerated the test well
and all, including those who did not complete the test, returned the
next day for an invasive investigative procedure. This suggests minimal
or no residual effect of their stressful experience. In common with
other studies [7,13], we modified the TSST-C protocol to suit our
population, in which it also elicited strong stress-responses. These
were highly variable suggesting that the test could be used to identify
children vulnerable to the effects of stress. Our findings in relation
to gender and pubertal status, especially in girls, are consistent with
earlier studies [14,15].
A number of biological and environmental factors
determine individual variations in stress-reactivity [3]. A test that
identifies individual differences in physiological stress-responses,
particularly HPAA response, is a vital requirement for research aimed to
study stress physiology [8]. The TSST-C, in which a combination of
public speaking and mental arithmetic tasks maximises participant
motivation by increased uncontrollability (eg. forced to make repeated
errors) and social evaluative threat, has been shown to stimulate
reliable cortisol response in children and adolescents [7,8,13]. Though
other modules such as isolated public speaking tasks, situations that
trigger negative emotions and threat of social separation/rejection,
exposure to novel situations and induction of mild physical pain also
trigger cortisol responses in adolescents, the TSST-C produces them more
consistently [7]. Our experience suggests that it is very crucial that
the protocol is followed exactly, and that the ‘judges’ are trained and
monitored during the study to ensure that they remain impassive and do
not give in to the normal human desire to encourage or reassure the
children.
We conclude that a modified TSST-C is a useful test
to examine stress-responses in Indian adolescents. This method can be
used effectively to establish the links between stress-responsiveness
and markers of disease development in Indian children.
Acknowledgements: The director of HMH, Kiran KN,
the staff of Epidemiology Research Unit and MRC Lifecourse Epidemiology
Unit, Fogarty International Center and the Eunice Kennedy Shriver
National Institute of Child Health and Human Development at the National
Institutes of Health.
Contributors: GVK, SRV, AJ, DH, CHDF: conceived
and designed the study; GVK, SRV, MPM, HU acquired the data; GVK, CHDF
drafted the article; GVK, AJ, DS, KS, AVK, CHDF: analyzed and
interpreted data. All authors revised the manuscript critically for
important intellectual content, and approved the final version to be
published. GVK will act as the guarantor of the study.
Funding: Parthenon Trust, Switzerland, Wellcome
Trust, UK, Medical Research Council, UK.
Competing interests: None stated.
|
What is Already Known?
• TSST-C is a valid test for eliciting
cortisol responses to stress in European children.
What This Study Adds?
• TSST-C is a useful test to examine cortisol
and cardiovascular stress-responses in Indian children.
|
References
1. Chrousos GP. Stress and disorders of the stress
system. Nat Rev Endocrinol. 2009;5:374-81.
2. McEwen BS. Protective and damaging effects of
stress mediators. N Engl J Med. 1998;338:171-9.
3. Kudielka BM, Hellhammer DH, Wust S. Why do we
respond so differently? Reviewing determinants of human salivary
cortisol responses to challenge. Psychoneuro-endocrinology.
2009;34:2-18.
4. Ward AM, Fall CH, Stein CE, Kumaran K, Veena SR,
Wood PJ, et al. Cortisol and the metabolic syndrome in south
Asians. Clin Endocrinol (oxf). 2003;58:500-5.
5. Buske-Kirschbaum A, Jobst S, Wustmans A,
Kirschbaum C, Rauh W, Hellhammer D. Attenuated free cortisol response to
psychosocial stress in children with atopic dermatitis. Psychosom Med.
1997;59:419-26.
6. Krishnaveni GV, Veena SR, Hill JC, Kehoe S, Karat
SC, Fall CH. Intra-uterine exposure to maternal diabetes is associated
with higher adiposity and insulin resistance and clustering of
cardiovascular risk markers in Indian children. Diabetes Care.
2010;33:402-4.
7. Gunnar MR, Talge NM, Herrera A. Stressor paradigms
in developmental studies: What does and does not work to produce mean
increases in salivary cortisol. Psychoneuro-endocrinology.
2009;34:953-67.
8. Dickerson SS, Kemeny ME. Acute stressors and
cortisol responses: a theoretical integration and synthesis of
laboratory research. Psychol Bull. 2004;130:355-91.
9. Pilgrim K, Marin M, Lupien SJ. Attentional
orienting toward social stress stimuli predicts increased cortisol
responsivity to psychosocial stress irrespective of the early
socioeconomic status. Psychoneuroendocrinology. 2010;35:588-95.
10. Tanner JM. Growth in adolescence. 2nd edition,
Oxford: Blackwell Scientific Publications, 1962.
11. International Institute for Population Sciences
(IIPS) and Operations Research Centre (ORC) Macro 2001. National Family
Health Survey (NFHS-2), India 1998-1999. IIPS: Mumbai.
12. Veena SR, Krishnaveni GV, Wills AK, Kurpad AV,
Muthayya S, Hill JC, et al. Association of birth weight and head
circumference at birth to cognitive performance in 9- to 10-year-old
children in South India: prospective birth cohort study. Pediatr Res.
2010;67:424-9.
13. Jones A, Godfrey KM, Wood P, Osmond C, Goulden P,
Philips DIW. Fetal growth and the adrenocortical response to
psychological stress. J Clin Endocrinol Metab. 2006;9:1868-71.
14. Jones A, Beda A, Osmond C, Godfrey KM, Simpson
DM, Phillips DIW. Sex-specific programming of cardiovascular physiology
in children. Eur Heart J. 2008;29:2164-70.
15. Gunnar MR, Wewerka S, Frenn K, Long JD, Griggs C.
Developmental changes in hypothalamus-pituitary-adrenal activity over
the transition to adolescence: Normative changes and associations with
puberty. Dev Psychopathol. 2009;21:69-85.
|
|
|
 |
|
