|
|
Recommendations Indian Pediatrics 2004; 41:559-575 |
|||||||
|
IAP National Task Force for Childhood Prevention of Adult Diseases: Childhood Obesity |
|||||||
|
Department of Pediatrics, KEM Hospital, Pune 411 011, India. Correspondence: *Dr. Sheila Bhave, Consultant in Pediatric Research, Department of Pediatrics, KEM Hospital, Pune 411 011, India. Email : [email protected] **Associate Consultant , Pediatric Gastroenterology. *** Research Associate.
Table I Consequences of Childhood Obesity(1-7).
Several elegant reviews and recom-mendations by expert committees have been published for prevention and treatment of childhood obesity in the developed countries(6,7). The aim of this paper is to highlight some of the unique features of obesity in India, and to suggest interventions based on the prevailing health and social infrastructure systems in our country. 2.1 Obesity is a global epidemic(8) According to WHO (2000) atleast 50% of adults and 20% of children in U.K. and U.S.A. are currently overweight. Prevalence of overweight amongst Australian children has increased from 11% in 1985 to 20% in 1995(8). Childhood obesity has tripled in Canada in last 20 years. It has been estimated that, in 1995, the direct costs of treatment of obesity in USA accounted for $70 billion with far greater indirect costs(9). Obesity does not seem to have spared developing countries either. Thailand, Iran, Nigeria and Brazil have all reported unprecedented levels of obesity with trends that are substantially rising every year(2). The calculated global prevalence of overweight (including obesity) in children aged 5-17 years is estimated by the International Obesity Task Force (IOTF) to be approximately 10%, but this is ‘unequally distributed’ with prevalence ranging from over 30% in Americas to <2% in sub Saharan Africa(2). 2.2 India is fattening too In a recent study by Reddy, et al., more than 28% of adult males and 47% of adult females in urban Delhi were overweight by WHO standards(9). In the same study the corresponding figures for overweight in a neighbouring Haryana rural area were 7% in males and 9% in females. Conversely, as many as 38% of males and 36% of females in the rural area were actually ‘underweight’ by BMI standards. Such an ‘urban, rural divide’ has been documented in other Indian studies too(10). In children, the difference between the rich and the poor is fairly evident in recently conducted urban studies. Ramachandran, et al. studied children from six schools in Chennai, two each from high, middle and lower income groups(11). The prevalence of overweight (including obese) adolescents ranged from 22% in better off schools to 4.5% in lower income group schools. In a Delhi school with tution fees more than Rs. 2,500 per month, the prevalence of overweight was 31%, of which 7.5% were frankly obese(12). In Pune the figures for overweight children are 24% in a well off school and 6% in a ‘corporation’ school (unpublished data). 3. What is obesity and how do we measure it? Obesity is defined as a condition of abnormal or excessive fat accumulation in adipose tissue, to the extent that health may be impaired (WHO consultation on obesity, 2000)(8). It has to be pointed out that the terms overweight and obese are often used some-what loosely and interchangeably. However, standardization is necessary for international and secular comparisons. 3.1 Measurement of obesity Body weight is reasonably correlated with body fat, but is also highly correlated with height. Therefore, weight adjusted for height squared [body mass index (BMI in kg/m2)] is a useful index to assess overweight and is a fairly reliable surrogate for adiposity. It is calculated easily from weight and height and it correlates with other measures of body fatness in children and adolescents. BMI also cor-relates with markers of secondary complica-tions of obesity, including current blood pressures, blood lipids and with long-term mortality(13). A limitation of BMI however is that it cannot differentiate an obese individual from a muscular one. It also cannot locate the site of fat e.g., people with ‘central obesity’ may have normal BMIs. Inspite of several limitations, BMI as of now appears to be the most practical way of measuring and comparing obesity for clinical and epidemio-logical purposes. As per WHO classification (for adults) BMI >25 = overweight and BMI >30 = obesity However, as these WHO criteria may underestimate obesity in Asians, the Inter-national Obesity Task Force (IOTF) has proposed the standards for adult obesity in Asia and India as follows(14). BMI >23 = overweight and BMI >25 = obesity. 3.2 Reference charts for children BMI values for adults, are age independent and same for both sexes. However in children, BMI changes physiologically (substantially) with age and sex. At birth the median BMI is as low as 13 kg/m2, increasing to 17 kg/m2 at age 1, decreasing to 15.5 kg/m2 at age 6, then increasing to 21 kg/m2 at age 20. Many countries have published BMI-for-age charts for their populations, and some have also defined cut-off points on these charts to define overweight and obesity. A recent Indian study by Agarwal, et al. has described indices including BMI and skinfolds for affluent Indian school children(15). However, the sample size of the study is probably not large enough to generate internationally accepted standards. The two BMI charts that can be used as a reference, for Indian children, as of now, therefore are: (1) The NCHS/CDC charts from USA(16). The American Obesity Association uses the 85th percentile of BMI for age and sex as a reference point for overweight and the 95th percentile for obesity in children. These charts can be readily downloaded from the internet sites, but are however, based on well off populations from USA. (2) Recently, new BMI standards in children using a large internationally represen-tative sample from six different countries (not India), with widely differing prevalence rates for obesity have been published(17). Age- and sex-specific BMI cut-off points for defining overweight and obesity in children have been derived by identifying percentiles in children analogous to adult BMIs of 25 kg/m2 and 30 kg/m2, respectively. These are referred to as IOTF cutoff points and are now recommended as standards for international comparison of data(2). 3.3 Other markers of obesity Other markers and measures of obesity are summarised in Table II. Table II Other Markers of Obesity and Comments.
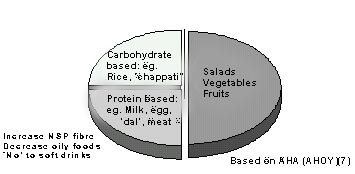
All these markers have their individual advantages (e.g., waist circumference for central obesity, DEXA for actual fat percentage) but none are really standardized as yet for children. 4. Epidemiology 4.1 Determinants of obesity and its persistence Atleast 30% of obesity begins in childhood. Conversely 50 to 80% of obese, children become obese adults(1). Many longitudinal studies have demonstrated convincingly, the substantially higher risks of child onset obesity(18,19). In the Harvard study, morbidity from cardiovascular disease, diabetes, obesity related cancers and arthritis was 50 -100% higher in obese individuals who were also obese as children and generally the cardiovascular mortality in such individuals was doubled(20). The crucial periods for persistence of obesity appear to be (i) gestational period (ii) adiposity rebound age (5-7yrs) and (iii) adolescence. A number of studies have shown that high birthweight is positively related to subsequent fatness(21) but higher prevalence of obesity is also seen in lower birthweights–the U or J shaped relationship(22). The tendency for indicators of adiposity such as BMI to fall around the age of one year, and then increase again by around 5th year is referred to as ‘adiposity rebound’. It is now evident, that earlier the rebound the greater the risk of subsequent obesity, although what drives the timing of adiposity rebound remains obscure(23). However, the most important predictor of adult obesity appears to be adolescent weight and changes of BMI during this time(24). The older a child is, when he or she remains overweight, the greater the likelihood that overweight will remain in adulthood. 4.2 Indians at high risk; our special concerns The prevalence of diabetes, CHD and other life style disorders is increasing alarmingly in India, and is affecting much younger populations than in the West. A large pool of young Indians demonstrate ‘prediabetics’ (i.e., insulin resistance and or glucose intolerance)(25). Gestational diabetes is common in mothers. The association of these problems with high BMIs and importantly central obesity is now well accepted(26). In transitional economies such as in India obesity and malnutrition often coexist (‘double burden of disease’) causing confusion in health messages(8). Infact, frank obesity may not be as high in India as in the west, but the body composition and metabolism of Indians (and Asians in general) make them especially prone to adiposity and its consequences(27). South Asians have atleast 3 to 5% higher body fat for the same BMI as compared to Caucasians(28). The fat is typically located centrally, and around visceral organs where it is meta-bolically more dangerous than peripheral fat. Recent Pune studies have demonstrated the ‘thin fat Indian Phenotype’ with evidence of hyperinsulinemia even at birth(29). Moreover, recent longitudinal studies in India have highlighted the deleterious effect of acce-lerated weight gain in childhood ‘crossing of centiles’ especially in LBW babies(30,31). Indices of insulin resistance and cardio-vascular risk factors were found to be highest in those that were born ‘small’ but were big by 8 years in the Pune study, even though they were not obese in absolute terms. The recent Delhi study in young adults showed that an increase of BMI of 1 SD from 2 to 12 years of age, increased the odds ratio for disease by 1.36(31). Further, continuing cohort studies in Pune suggest that accelerated growth in childhood is associated with early maturation and greater risk of obesity (unpublished results). It is now evident that our traditional understanding of concepts of ‘catch up growth’, weight gain in pregnancy and birth weight may need redefining. 5. Causes of the epidemic (in India) In India there is a tremendous ‘Urban/Rural’ and ‘Rich / Poor’ divide, prevalence in the urban rich being much higher than in rural areas and poor communities. The causes include: 5.1 Changes in life style (‘urbanisation’) With improving standards of living, and availability of food in plenty, the upper class societies of India in recent years have urbanized to western levels. The components of life style changes are: • Unhealthy eating patterns, wrong choices of food: Traditional micronutrient rich foods are being replaced by energy dense highly processed, micronutrient poor foods with greatly increased portions ‘Dil Mange More’. High calorie snacks, junk food revolution, cool cola (‘thanda matlab’) colonisation, and food as rewards or demonstration of love are all part of new life styles. All celebrations and festivals seem to be centered around rich foods. • Sedentary pursuits: TV and movie watching, video games, internet gazing and telephone gossip sessions are now important activities of children. TV also affects by heavy marketing of colas and other fatty foods. The number of TV sets and telephone connections are touted as indices of development! • ‘Obesogenic schools’ and Tution classes: An important factor for obesity in India is the intense competition for admissions to schools and colleges with flourishing tuition classes right from nursery levels ! Children are forced to use their play time for additional studies. Games or physical training sessions are restricted or non existent in many schools. Some schools do not have any playgrounds at all. • Inadequate play areas: Due to unsafe roads (traffic, crime) children are dis-couraged form walking or cycling to school. Motorized vehicles are popular and they are perceived to be quicker and safer for transport. Erosion of open spaces for exercise and lack of parental time to supervise play are all part of new obesogenic lifestyles. As against food as rewards, ironically exercise is meted out as a punishment - ‘100 sit ups,’ ‘run round the field.’ 5.2 Genetic ‘Constitutional’ pre-disposition The factors responsible could be: • Modern environment may have unmasked previously silent obesogenic genes ‘thrifty genotypes’(32). • Programming of previously malnourished populations to accumulate fat more intensely in an attempt to store for future starvation (‘early life origins’)(33,34). • Stunting in childhood (short height for age) may increase the risk of central obesity especially in transitional economies(35). • High rate of gestational diabetes in pregnant women causing higher birth weights in babies leading to inter-generational effects of obesity in childhood and its attendants problem(36). • Familial pattern of eating, exercise and behavior. 5.3 Other factors • Prolonged and exclusive breast feeding is associated with a significantly lower rate of obesity and hypertension in later life(37). It is not clear if early introduction of energy dense supplements in infancy has contributed to childhood obesity in India. • The high glycemic index of our predominantly carbohydrate diet may be responsible for hyperinsulinism, weight gain and eventual type 2 diabetes(38). • Yet other factors controlling body weight regulation such as `low body metabolic rate (BMR)' and probably governed by hypothalamus - these factors as of now are all speculative(1,2). 6. How can we control this epidemic? 6.1 Primary prevention of childhood Obesity: Public health approach Atleast 1 in 10 urban middle class children in India is overweight. If we allow this epidemic to continue we will top the world in Diabetes and CHD earlier than estimated. The cost of treating diabetes mellitus and associated disorders alone will consume a major chunk of our resources which we can ill afford. Only community based approaches can address such large numbers of affected children. Further, results of treating estab-lished obesity at clinics are dis-appointing, though on a positive note children do better than adults(6). Obesogenic lifestyle behaviors are less well developed in children and therefore more amenable to change. An overwhelming body of evidence now indicates that prevention must begin in childhood to reduce the burden and cost of obesity in society(2,8). In India, Public health efforts so far, have been directed towards improving nutrition (and thereby implied weights of newborns, infants, children and mothers). Obesity prevention campaigns will have to be carefully worded to avoid conflicting messages and deleterious results! However the only way to cut short the escalating epidemic appears to be prevention of obesity and other lifestyle problems in childhood itself. The control of this epidemic is a challenge and requires strong social and political will in addition to medical management. A concerted public health approach will be required for effective prevention. The whole family, indeed the whole society must be targeted for the health of the future generation. 6.2 Do interventions/preventive methods work? In India, we have just about started reporting high prevalence of obesity in children. Obviously then, no intervention studies have been carried out as yet. But a number of studies have been carried out and reported from the western countries(2,39,40). Some reports from developing countries have started to emerge(41). By and large recent studies in children (as against adult studies) have shown some positive short term and long term results with programs that target the whole life style of children. The CATCH study (Child and adolescent trial for cardiovascular health) in multi racial American school children and the ‘Go Girls’ community based study in African American girls showed that children can be taught to eat less fat and exercise more!(40,42). Larger numbers and longer time inputs could have shown positive influence on prevalence of obesity too. An important UK school based study (APPLES) which targeted whole community reported successful imple-mentation of the program but unsuccessful result (in fact the study group had reduced activity and no weight loss!)(43). Obviously more time or different approaches will have to be tried to improve outcome. Perhaps the most optimistic results have come from Singapore; an 8 year school based campaign with government support (Health Promotion Board) was successful in implementation as well as reduction in prevalence of obesity (from a high of 16.6% in early 90s to less than 14.6% in 1998)(44). This study however was targeted at obese children only, and the possibility of causing psychosocial stigmas by such an approach must be considered. In Brazil, an ambitious programme to promote physical activity in children was launched in 1997, in Sau Paulo, and because of its impact has now been adopted throughout the country - ‘Agita Brasil’(41). The Brazil programme has highlighted psychosocial and educational benefits as well as physical benefits but, is yet to be assessed in terms of obesity prevalence. Obviously many lessons can be learnt from the successful and the not so successful programs in other countries. The following strategies suggested specifically for our country, are based not only on the above evidence, but on observational data and also on logic. 6.3 Strategies and Aims: Public Health Approch(2,7,8,45) As a Public Health Approach, essentially all children, adolescents and families should benefit from counseling to prevent excess weight gain and obesity. • Life style approach (i) Healthy eating patterns: Emphasis should be on nutrition rather than ‘dieting’. It is important to maintain healthy components of traditional diets (i.e., micronutrient rich food such as fruits, vegetables and whole grain cereals) and guard against heavily marketed energy dense fatty and salty foods (e.g., pre-packaged snacks, ice-creams and chocolates) and the sugary cold drinks. The strategy should be to recognise and eliminate risk features of high calorie intake such as frequent snacking (samosas, potato chips, chiwdas), eating out frequently (burgers, dosas), celebrating with food (cake, chocolates) and drinks (colas, beers). Healthier alternatives can be suggested. Habits attained early have more chance of remaining throughout life. A simple Indianised message based on recommendations of AHA(7) could be–"think of a day’s food composition as a ‘Thali’ wherein 50% (half) is full of vegetables, salads and fruits. A quarter (25%) should be made up of cereals such as rice and/or chapattis and the remaining quarter should be protein based (dal/milk/egg/animal protein)". Fried, snacks and ‘sweet dishes’ are only for a very few special occasions ! (Fig. 1).
(ii) Increase physical activity levels: Children should be encouraged to be active not only for weight control but for general well being. Many adolescents/pre adolescents find defined physical exercises (aerobics, tread-mills) boring and punitive and are more likely to continue activity if it is incorporated into their daily routines, e.g., walking or cycling to school and playing with friends in the grounds. The WHO recommends atleast 30 minutes of cumulative moderate exercise (equivalent to walking briskly) for all ages; plus for children, an additional 20 minutes of vigorous exercise (equivalent to running), three times a week(46). These recommendations are basically for prevention of CHD; prevention of obesity may require more physical exertion. In general, moderate to vigorous activities for a period of atleast one hour a day may be a more practical recommendation for all school going children. (iii) Decrease sedentary behavior: Perhaps even more important is decreasing sedentary behavior. In our country, chief sedentary behaviors are television (should be restricted to no more than 2 hours a day), computers, telephone conversations and importantly tution classes (restriction may not be possible!). • Avoid Overfeeding Stunted Populations. Assess stature, and prevent feeding excess calories to children with low weight for age but normal weight for height i.e., ‘stunted children’. Most PEM prevention programs (school mid day meals) use food supplements that provide ample energy and protein but may be deficient in micronutrients. Such programs may induce weight gain in underweight children while length deficit may not be reversed, thereby creating a risk for obesity(47). Quality of foods provided in ‘feeding programs’ is crucial–fruits and vegetables should be included and energy excess should be avoided(47). • ‘Target’ populations most in need of interventions; in India this would probably mean urban children from higher and mid socio economic status. Targeting avoids confusing messaging directed towards opposite segments of society. • ‘Tailor the interventions’ to suit the specific needs of the community. Use culture appropriate messages e.g., urban Indians need to know that ‘chubby’ or fat infants are not equal to ‘healthy’ babies ! • Address ‘Behavior’ Change. Behavior is culture based. Consider socio-cultural and ethnic issues–these would be important in suggesting diets and activity. For example, adolescent girls from conservative families are often discouraged from playing outdoor games but can be encouraged to perform physical household chores. • Focus on involvement of entire family (parents, grandparents) indeed the entire community for better results. Average Indian families have poor knowledge of ‘healthy eating’. • Confront vested interests e.g., advertising of colas. • Build supportive infrastructure e.g., safe play grounds, transport and town planning. 6.4 Special strategies to target specific age groups(8) Infants and Young Children • Mothers should prevent excess weight gain in pregnancy; control diabetes or impaired glucose tolerance in pregnancy. • Promote exclusive breast feeding for six months. • Avoid adding sugars, starches or oils to feeding formulas. • Assure appropriate micronutrient intake especially of iron, calcium and vitamins. • Monitor growth with weight for height and BMI. Discourage ‘accelerated crossing of centiles’. • Make clear differentiation of ‘catch up growth’ from accelerated weight gain. Catch up growth should be associated with gain in height proportional to weight gain. • Instruct mothers to accept the child's appetite and not to force feed. • Instruct families that ‘fat infants make fat adults’. Children and adolescents The fat rebound age (5-8years) and adolescence are particularly high risk periods for accumulating fat. Strategies for prevention include • Promote active lifestyles including at least one hour of vigorous ‘play’ per day. Limit TV and other sedentary activities to <2 hr/day. Physical activity is as important, if not more than didactic lessons. • Promote sensible eating–increase fruit and vegetables and restrict energy dense sweets and soft drinks. Impart health education skills to make healthy food choices e.g., early home cooked dinners to avoid TV snacking. Substitute soups/salads/baked foods for wafers, chocolates /fried foods. • Modify environments to promote physical activity e.g., safe roads for cycling, jogging. • Celebration should be in the form of outdoor play/picnics rather than fast food joint parties. • Educate about the evils of alcohol/tobacco to adolescents. 6.5 Channels of interventions / health education School Based Programs Schools are probably the ideal medium of intervention as they are central to children’s lives and information can be relatively quickly dissipated through this channel. Aspects to be considered are: • Training of teachers in lifestyles, nutrition and activity. • Introduction of ideal school meals or provision of canteens offering only healthy options based on Indian foods. • Introduction of ‘nutrition and physical education’ in school curriculum. These activities should become compulsory and /or a ‘scoring subject’ with marks to be added to total grades. Only then will parents/students give the required attention and time to this in this competitive world of academics! • After school games (supervised/unsupervised) to be encouraged. Opening up of school playgrounds on weekends and holidays. • Obese children should not be teased, targeted or bullied or isolated. • Involve parent associations. • School health check ups should monitor BMI along with height and weight annually. Media involvement Another powerful channel especially for upper and middle class societies is media coverage. Regular columns and supplements have already started making a mark. Health centers/Doctors/Other Professionals • It is important for doctors and other health professionals to think ‘prevention of obesity’ at all visits and incorporate relevant health education. The success of this channel in recent years with ORS, immunizations, breast feeding and prevention of malnutrition makes this an optimistic channel for such a campaign. • Incorporate BMI charts / IOTF cut offs and waist circumference (in addition to height, weight and head circumference) in routine health records. Monitor BMI every year, particularly for children from high risk families. • Identify children with BMI >75th centile (and with accelerated crossing of centiles) for frequent monitoring and ‘life style’ interventions. • Discourage parent's obsession with food intake and pleas for tonics. Governmental authorities Both health and infrastructural authorities should be responsible for • Devising national strategies • Encouraging food outlets/restaurants to serve healthy choices • Providing safe exercise opportunities. • Regulate advertisements aimed at children and insist on food labelling. • Consider taxation on ‘fatty food’ or alternatively reduce taxation/promote production of fresh food and vegetables. As said earlier this sort of a Public Health Approach requires strong social and political will with concurrent medical motivation and management. 7. Management of established obesity Whereas the public health campaign is to be targeted to the society as a whole, individual or clinic based approach is necessary for the treatment of the obviously obese child. A guideline for assessment by pediatricians in their clinic based practice is provided in the accompanying Table III. Principles of therapy are outlined in the following section. Please click here to view 7.1 Management of obesity–clinic / individual approach Management of established obesity in children needs a concerted and a sustained effort from a team of experienced health professionals. Treatment is more likely to be successful in children than adults. Western guidelines by and large apply to our clinics and are outlined below(2,6,48). Goals of therapy: Approach to therapy Medical Goal: Medical goal should be resolution of complications and co-morbidites such as hypertension and hyperlipidemias. Behavioral Goal: Achievement of healthy eating and activity patterns rather than achievement of ideal body weight . Weight Goal: Weight maintenance rather than weight loss (unless moribund obesity) in young children–‘Let the child grow into his weight’. Prolonged weight maintenance will allow a gradual decline in the BMI as the child grows in height. 7.2 General Approach to Therapy(1,6,38) • Institute small, gradual and permanent changes, not short-term diets or exercise programs aimed at rapid weight loss. • Involve the family and all care givers in the treatment program. • Intervention should begin early (later than age 3 yrs but earlier than adolescence). • Clinicians should encourage and empa-thize and not criticise. 7.3 Principles of therapy (Table III) Theoretically, obesity management is energy balance (eat less and exercise more). However, in practice the treatment can be challenging and frustrating because of frequent relapses. The principles of therapy are generally same as in prevention viz.: (a) Reduced calorie intake; (b) Increased activity levels; (c) Decreased sedentary behavior; (d) Family involvement; (e) Behavioral changes. Limiting energy intake of growing children can result in decreased linear growth velocity in obese children and is therefore risky(45). Dieting could also increase prevalence of inadequate nutrients, such as iron, calcium, zinc and vitamins A, C and E. High degrees of parental dietary control may infact have adverse psychobehavioral effects on young children with treatment failures(49). Hence the aim should be provision of well balanced healthy meals with a healthy approach to eating. Several different dietary studies have shown successful reduction of calorie intake and improved eating behaviors(45). The advise usually centres around reducing calories from fat, saturated fats, cholesterol and sugars (high density foods) while increasing fruits, vegetables and whole grain cereals (lower density foods). Counting of calories can be tedious and inaccurate and it is more advantageous to supply indigenous versions of Food Guide Pyramids or Epstein’s traffic light diets(50). Trials of hypocaloric diets, protein modified fasts, fibre supplementation and anorectic drugs have been shown to be by and large, ineffective in children in the long range(48). Addition of physical activity and reduction in sedentary behavior, both (supervised and unsupervised) improves long term outcome(48). The important components of behavioral therapy include treatment of families as a whole, identification of problem behaviors and their modifications, and `tailor' made advise and support component. Parenting skills recommended in treatment plans are praising the child's behavior, never using food as reward, establishing firm daily family meal and snack times, providing only healthy options, removing temptations and being a good role model(51). 7.4 Intensive therapy Yanovski (2001) reviewed the limited data on intensive therapies that have been proposed and tried in children(52). These include (a) severe energy restriction below 1000 kcal / day (b) drugs-fenfluramine, metformin, sibu-tramine, leptin, octreotide and (c) bariatric surgery such as gastric bypass and gastric stapling. Although initial weight loss can be dramatic, most of these approaches are fraught with significant adverse consequences and need constant long term monitoring. These are therefore, to be considered only in the rare gross cases with potential life threatening complications. None of the treatment modalities can be successful without positive behavioral changes.
Members of the Task Force
| |||||||
|
![]()