|
|
Original Articles Indian Pediatrics 2003; 40:518-531 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Safety of Oral Use of Nimesulide in Children: Systematic Review of Randomized Controlled Trials |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Piyush Gupta and H.P.S. Sachdev* From the Departments of Pediatrics, University College of Medical Sciences, Delhi 110 095 and *Maulana Azad Medical College, New Delhi 110 002, India. Correspondence to: Prof. H.P.S. Sachdev, E-6/12
Vasant Vihar, New Delhi 110 057, India. Manuscript received: February 10, 2003, Initial
review completed: February 27, 2003, Nimesulide has been widely used to treat fever in children. Due to reports of adverse drug reactions, discontinuation or modification of its use has been suggested. Objective: To evaluate the safety of oral use of nimesulide in children. Design: Systematic review of published randomized controlled trials. Search strategy: Electronic searches of databases (PubMed, Cochrane, Toxnet) for relevant trials upto January 2003 using specified key words. The studies were also identified by searching the references of available meta-analyses and review articles, and bibliography of pertinent references. Inclusion criteria: Randomized controlled trials in children (£ 18 years of age) comparing the use of oral nimesulide with placebo or other antipyretic, anti-inflammatory or analgesic agents. Outcome: The primary outcome variable included the commonly encountered adverse effects of nimesulide therapy, i.e., hypothermia, abdominal symptoms, gastrointestinal bleeding, and elevated liver enzymes. Data collection and analysis: One of the authors developed a questionnaire and independently extracted data on methods, type of participants, interventions and outcomes. The meta-analysis was conducted using pooled relative risk with 95% confidence intervals, with random effects model assumption. Results: We identified 16 trials that fulfilled the inclusion criteria. These included 1254 subjects, with mean age between 22 –140 months. Nimesulide was primarily used for its antipyretic (10 trials) or anti-inflammatory and analgesic activity (4 trials). One study each evaluated the symptomatic improvement in ARI and bronchial asthma. The control group included administration of placebo (3 studies), paracetamol (9 studies), and ketoprofen, naproxen, mefanemic acid and aspirin in one study each. The pooled effect sizes of various adverse events as compared between nimesulide and different control groups were: hypothermia (RR: 1.055; 95% CI: 0.184 – 6.047; P = 0.952), abdominal symptoms (RR: 0.464; 95% CI: 0.264 – 0.816; P = 0.008), gastrointestinal bleeding (RR: 0.914; 95% CI: 0.236 – 3.543; P = 0.896), and asymptomatic liver enzyme elevation (RR: 2.678; 95% CI, 0.558–12.853; P = 0.218). Cutaneous and renal adverse effects were not seen in any of the included studies. Conclusions: Oral nimesulide is as ‘safe’ or ‘unsafe’ as other analgesics-antipyretics for short-term use (£ 10 d) in children. The drug is best avoided in known or suspected liver disease; caution is warranted while prescribing nimesulide concomitantly with other hepatotoxic drugs. There is limited data for drawing concrete inferences below the age of six months. Adverse effects, Analgesic, Antipyretic, Meta-analysis, Nimesulide Non-steroidal anti-inflammatory drugs (NSAIDs) are one of the most frequently prescribed medications in pediatric practice(1). Nimesulide (4-nitro-2-phenoxy-methanesulphonamide) is a relatively new NSAID, which can be given orally or rectally on a twice daily basis to reduce fever, pain and inflammatory symptoms in various disease states(2-4). This drug has been projected as an efficacious and useful alternative to other NSAIDs(5,6). Reports of safety and tolerability of nimesulide are available as descriptive reviews(1,3,7-10), case reports(11-22) and post marketing surveillance (PMS) trials(23-25). While most of the reviews and PMS trials have been conducted by the drug manu-facturers the case reports are docu-mented by individual researchers. The epidemiological analyses of data from subjects treated with nimesulide in clinical and PMS studies demonstrate that this drug is generally well tolerated(7,24-27). Contrary to these studies, individual reports have focused on serious hepatic(12,18,20,28), renal (11,16,21,29) and other adverse effects (15,25,27,30-32) following administration of nimesulide. Probably that is why, few countries have discontinued the sale and prescription of this drug(33,34). Other countries (USA, UK, Canada, Australia, New Zealand) have not licensed nimesulide for use in the first place(35,36). Notwithstanding this, the drug has been aggressively marketed in India. Recently, a controversy related to nimesulide use in children has surfaced in the Indian Press as well as in the various foras and meetings of Indian Academy of Pediatrics (IAP). Opinions have varied from the "need to ban this drug" to a "totally safe prescription"(35,37). We attempted to address this controversy on a voluntary basis and in an evidence-based manner through a systematic review of randomized controlled trials. Our primary objective was to determine whether oral use of nimesulide in pediatric population has an increased risk of adverse effects as compared to placebo or other drugs in the same class. Subjects and Methods Inclusion Criteria Studies with following pre-determined criteria were included: (i) randomized trials with oral nimesulide and a control group, receiving any other analgesic, anti-inflammatory, antipyretic agent or placebo; studies employing a rectal route were not eligible; (ii) trials restricted to children £ 18 years of age; and (iii) must have evaluated one or more adverse effects as an outcome measure. Search strategy We selected electronic bibliographic databases, including PubMed (1966 to Jan 2003), Cochrane Controlled Trials Register, and Toxnet, using specified keywords. Various combinations of keywords were used for the search from among the following: nimesulide, adverse events, side effects, toxicity, randomized controlled trials, clinical trials, case report, review, meta-analysis, and children. We also reviewed reference lists of identified articles and hand searched reviews. We did not search for any unpublished trial. All the trials identified by the above methods were listed. The title and abstract of the studies identified in the computerized search were scanned to exclude studies that did not meet our inclusion criteria. In case, the title and abstract did not yield the desired information, full text of the study was extracted to verify its suitability for inclusion in this systematic review. Retrieval and abstracting Full text of the articles thus identified, was retrieved. This was followed by final identification of the studies that fulfilled the inclusion criteria. A preformed questionnaire was used to abstract the data. Adverse effects were as defined by the respective authors of various trials. Trial Quality Quality of trials was assessed using recommended criteria(38). Concealment of allocation was classified as adequate, unclear or inadequate. Blinding was classified as double blind, single blind, and no blinding. The completeness of follow up was ascertained by calculating the percentage of participants excluded: (A) <3% of partici-pants excluded; (B) 3 to 9.9% of participants excluded; (C) 10% or more participants excluded. Statistical Analysis The pooled estimates of relative risk were calculated by Statsdirect statistical soft-ware(39) using both fixed effects and random effects model assumption(40). This program also computes the formal test of homogeneity, the statistic Q. We report primarily random effect estimates (conclu-sions were identical with both models) even though all the pooled results obtained were statistically homogenous. A value of 0.25 was substituted for zero (no side effect observed) since the computations do not accept zero in the numerator. For comparing hepatic enzyme elevations, only the studies that had specifically commented upon this facet and provided exact numbers were included for computation, while excluding those with a general mention of no adverse effect in serum biochemistry like liver function tests. Results Using the specified search words in different combinations (limited to "Humans" only), the citation yield was as follows: nimesulide and adverse events – 24; nimesulide and side effects – 173; nimesulide and toxicity – 22; nimesulide and clinical trials – 33; nimesulide and randomized controlled trials – 3; nimesulide and children – 55; nimesulide and review – 61; nimesulide and case report - 43; and nimesulide and meta analysis – 2. Many articles were common in different searches. All the articles clipped together, with each article cited only once, provided us with a final list of 246 reports, which were subjected to further scrutiny. We could identify a total of 19 trials relevant to the review question(36,41-58). Two of these were further excluded as they were concerned with rectal administration of nimesulide(41,42). Another one was not a randomized trial; hence not considered for further analysis(43). Thus, a total of 16 studies, meeting the inclusion criteria, were evaluated in this systematic review(36,44-58). Baseline Characteristics of the Studies Table I details the essential baseline characteristics of the included studies. A total number of 1254 subjects (mean age 22 to 140 months) were enrolled in these trials. Duration of administration and total number of doses of nimesulide ranged from 1-10 days and 1-30 doses, respectively. TABLE 1 Baseline Characteristics of the Included Trials (n=16)
ARI-acute respiratory infections; ADR: adverse drug reaction; BP-blood pressure; CRP: c reactive protein; ESR: erythrocyte sedimentation rate; HR-heart rate; LFT-liver function tests; KFT-kidney function tests; PT-prothrombin time; PTT=partial thromboplastin time; Tc-total leucocyte count; Dc-differential leucocyte count; RR-respiratory rate
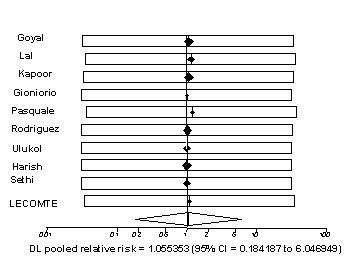
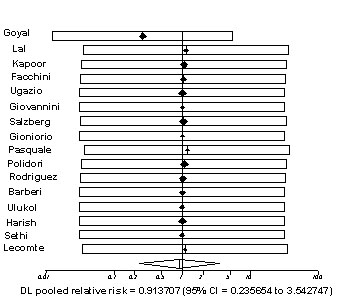
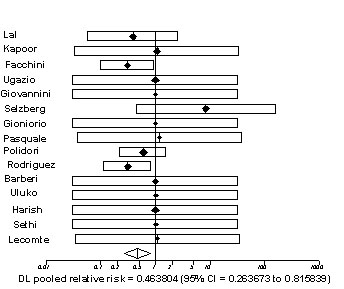
Eight trials were from Italy, 5 from India and one each from Belgium, Turkey and Switzerland. Nine trials employed paraceta-mol as the control group while placebo was used in 3 studies. Acetyl salicylic acid, ketoprofen, naproxen, and mefenamic acid constituted the control group in 1 trial each. Majority of the subjects (12 trials; 75%) had medical morbidities (usually respiratory; one study solely in severe asthma). Two trials were conducted on post-operative patients and one trial each on children with fractures and soft tissue injury. Nine trials were double blind, 3 were single blinded; and the rest were open. Allocation concealment was clearly adequate in 4 and uncertain in 8 trials. The loss to follow up was <3% in 10 (63%) studies. The status of funding of the trials was as follows: (i) total funding by the nimesulide manufacturer – 4 (25%)(44,56-58); (ii) only drug supplied by the nimesulide manufacturer – 2 (13%)(36,54); (iii) no funding by nimesulide manufacturer – 1 (6%)(55); (iv) source not mentioned – 9 (56%). Pooled Estimates The pooled estimates for the evaluated side effects are summarized in Table II and the related Forest plots in Figs. 1-4. All the pooled results were statistically homogenous. The relative risks for developing hypothermia, gastrointestinal bleeding, and hepatic enzyme elevation with nimesulide were comparable to the controls. The relative risk of developing epigastric pain, vomiting or diarrhea was significantly (P <0.01) lower (roughly half) with nimesulide. However, when only trials with a control group of either paracetamol or placebo were considered, the risks of these adverse effects were comparable in the two groups. Table II Nimesulide in Comparison to Controls.
The pooled estimates for the hepatic enzyme elevation are based on sample sizes of 177 subjects in the nimesulide group and 189 cases in the paracetamol group (all such studies had paracetamol as the control drug). In all the cases, the hepatic enzyme elevations were asymptomatic (only biochemical abnormality). In one trial(50), nimesulide was evaluated for relief of post-adenoidectomy pain and the study subjects had received volatile anesthetics that can also result in hepatic enzyme elevation. Transient elevation of liver enzymes was noticed in four children in this trial; this could also be attributed to the effect of anesthetics.
Fig. 1. Forest plot for relative risk of hypothermia. There is no
significant difference (P = 0.952) in
Fig. 2. Forest plot for relative risk of gastrointestinal bleeding.
There is no significant
Fig. 3. Forest plot for relative risk of epigastric pain, vomiting,
and diarrhea.
Fig. 4. Forest plot for relative risk of elevation of liver enzymes.
There is no significant Discussion The results indicate that the risk of hypo-thermia, gastrointestinal bleeding, epigastric pain, vomiting, diarrhea and transient asymptomatic liver enzyme elevation did not increase significantly with nimesulide administration as compared to other anti inflammatory analgesics or placebo. The pooled results were statistically homogenous and represent synthesis of randomized controlled trials which are considered the "best" evidence(59) epidemiologically. It would be useful to examine the potential limitations of this systematic review for evaluation of their impact on the validity of inferences: Firstly, we included only those trials that have been published in indexed peer reviewed journals. This raises the possibility of publication bias. However, there was no suggestion of bias from a scrutiny of the funnel plots. Exclusion of papers presented at conferences, symposia and data on files of drug manufacturers or developers may represent an advantage; "poor quality" and "commercially useful" data could be filtered out. Helsinn, the developers of nimesulide, published a review of data from 151 trials on nimesulide comprising of 4945 subjects(60). The incidence of adverse events was 7.1% and included those related to the digestive system, body as a whole, skin and nervous system. The incidence and nature of adverse events observed for nimesulide treated patients were similar to those of the placebo group. However, these trials are not published anywhere and are available only on the files of the Company! Inclusion of papers appearing in peer reviewed indexed journals ensures the author integrity as well as transparency and validity of the results obtained. Secondly, there is a possibility of competing interests pertaining to the publications included in this review. Out of 16 studies, 4 were totally funded by the manufacturers of nimesulide(44,56-58). In three studies(44,56,58), at least one of the authors was employee of the nimesulide manufacturers. Nine trials(45-53) appeared in the form of a symposium in a single issue of a Journal, that was sponsored by the industry. However, this appears inevitable for a newer drug, when no other independent source would be willing to invest in such studies. Declaration of source of funding in some of the included studies can be viewed as an attempt at transparency. Lastly, the pooled sample sizes may not be adequate for comparing rare adverse effects of nimesulide. A comparison of the findings of this systematic review with earlier literature on the subject would be pertinent. It has been suggested that nimesulide, a selective Cox-2 inhibitor, is less likely to induce gastrointestinal damage than seen with the other commonly used analgesic-antipyretic drugs(7,61,62). Spontaneous reporting data from Italy, where nimesulide is the most frequently used NSAID, has suggested that nimesulide carries the most favorable gastrointestinal (GI) tolerability profile of the NSAIDs investigated; there were few reports of severe GI reactions(26). Similar findings were observed as per our analysis. However, the pooled relative risk of GI adverse effects of nimesulide was not lesser than a control group including only paracetamol and placebo. This implied that reporting of GI symptoms is as common with nimesulide as paracetamol and/or placebo. The incidence of GI side effects is reported to be less with nimesulide as compared to ibuprofen, naproxen or aspirin(26,63,64). Recently, concerns have been raised regarding potential hepatotoxicity of nimesu-lide, especially in children(12,65). At least two deaths due to fulminant hepatic failure have been attributed to this drug(66). Nime-sulide has been associated with idiosyncratic hepatotoxicity in susceptible patients. The damage is probably mediated through oxida-tive stress and mitochondrial injury(8,67). The incidence of nimesulide-induced liver injury has been low (approximately 0.1 per 100,000 patients treated) and is comparable to that of other NSAIDs(8). Another fact is that the time of onset of liver reactions has varied from several days to almost 1 year, thus suggesting that rare cases of liver injury may be caused by a metabolic idiosyncrasy(67). Probably, there are multiple individual host factors that influence the toxic potential of nimesulide. On the basis of literature report(68), the following features of nimesulide-associated hepatotoxicity were identified: female sex (84% of cases), age (mean age 62 years), jaundice as a primary manifestation (90%) and the absence of peripheral blood eosinophilia. The average duration of therapy of published cases has been 62 d (range 7-180 days). Therefore, administration of nimesulide for a short period of time in childhood may not be an important risk factor for significant hepatotoxicity. The findings of our systematic review in relation to hepatic enzyme elevation support this inference. Renal adverse effects of nimesulide were investigated in a large database from Italy, containing all the spontaneous reports filed between 1988-1997(10). Of the 120 reports associated with oral nimesulide, 11 referred to suspected renal adverse reactions. In India, 3 cases of gross hematuria associated with nimesulide were reported in children(69); the resolution was complete following withdrawal of the drug. A countrywide post marketing surveillance of nimesulide suspension reported the incidence of hematuria in children to be 0.1% of all ADRs(23). This surveillance was based on 4097 report forms from 430 pediatricians. Hematuria and other reported side effects of nimesulide such as hypoglycemia, periorbital puffiness, photo-dermatitis, urticaria, etc. were not observed in any of the studies included for this systematic review. To conclude, on the basis of this meta-analysis, it appears that for short-term use (£ 10 days) in children, nimesulide is as ‘safe’ or ‘unsafe’ as other analgesics-antipyretics. In view of slight elevation of liver enzymes in the nimesulide group, though statistically insignificant, the drug is best avoided in known or suspected liver disease, and caution is warranted while prescribing nimesulide concomitantly with other hepatotoxic drugs. There is limited data for drawing concrete inferences below the age of six months. Contributors: HPSS conceived the paper and suggested the plan of action. PG searched, extracted, reviewed and abstracted the available literature. HPSS performed the metanalysis. PG drafted the manuscript, which was edited and improvised by HPSS. Both the authors approved the final version. HPSS and PG, both shall stand guarantors for the study. Funding: None. Competing interest: None stated. The review was purely voluntary and non-funded effort, aimed at resolving the controversy in an evidence-based manner.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()