|
|
|
Indian Pediatr 2016;53: 77 |
 |
Massive Idiopathic Prepubertal Gigantomastia
|
|
#Andrés de Jesús Barragán-Morteo and *Mario
Aurelio Martínez-Jiménez
Department of #Plastic and Reconstructive Surgery, Hospital
Central Dr. Ignacio Morones-Prieto, and *Facultad de Medicina,
Universidad Autónoma de San Luis Potosí; México.
Email: [email protected]
|
|
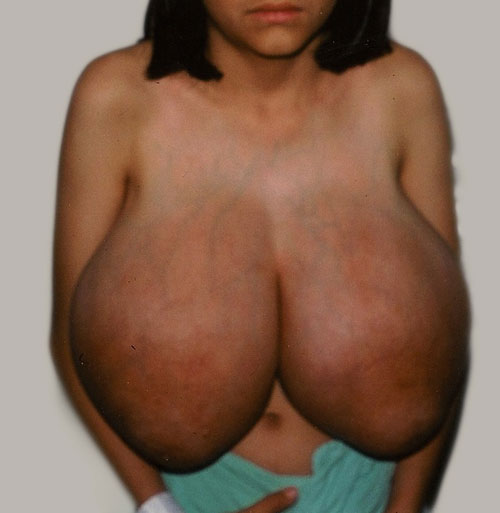
Gigantomastia is rare, and the majority of cases are reported after
puberty. In some cases, it can be due to an exaggerated response of
breast parenchyma to estrogen [1-2]. We present the case of an
11-year-old Mexican girl, with progressive, bilateral, and symmetric
breast enlargement (Fig. 1). It started before menarche,
and caused postural problems and back ache. The patient did not have any
illness or a family history of gigantomastia. She was not receiving any
drugs. The patient weighed 37.7 kg, and height was 139 cm (BMI 19.5);
external genitalia were Tanner I. On examination, breasts were massively
enlarged (35 cm from the sternal notch to nipple areola complex). The
breasts were ptotic, and the superficial veins were prominent and
dilated, without ulceration of the skin. The areola were immature
without any discharge or hyperpigmentation. No breast masses could be
palpated. There was no axillary lymphadenophaty. Hormonal assays were
within the normal range. Ultrasonography of the breast and pelvis was
normal. No evidence of any tumor was found on magnetic resonance imaging
of the brain.
 |
|
Fig. 1. Excessive breast growth in
gigantomastia.
|
She underwent a reduction mammoplasty with the
inferior pedicle technique, with preservation of the nipples areola
complex. Weight of each breast was 4000 g, comprising about 20% of the
total body weight. The histological examination showed hyperplastic
terminal duct lobular units with edematous stroma. Breast tissue
estrogen and progesterone receptors were negative. Post-operatively, the
measurement of the sternal notch to nipple areola complex was 16 cm.
Four years later, she underwent a breast augmentation with mammary
implants. After 10 years, there was no recurrence, and she had an
acceptable physical appearance.
In idiopathic prepubertal gigantomastia, reduction mammaplasty
is usually the first treatment option, with or without hormonal therapy,
because of preservation of lactation. Recurrence may occur in many cases
[3-5].
References
1. Dancey A, Kham M, Dawson J, Peart F. Gigantomastia –a
classification and review of the literature. J Plast Reconstr Aesthet Surg.
2008;61:493-502.
2. Skillman J, Beechey-Newman N, Hamed H.
Gigantomastia unrelated to pregnancy or puberty: a case report. Breast.
2002;11:179-80.
3. Pryor LS, Lehman JA Jr, Workman MC. Disorders of
the female breast in the pediatric age group. Plast Reconstr Surg.
2009;124:50e-60e.
4. Dafydd H, Roehl KR, Phillips LG, Dancey A, Peart
F, Shokrollahi K. Redefining gigantomastia. J Plastic Reconstr Aesthet
Surg. 2011;64:160-3.
5. Schumacher O, Ashkar W, Daberning J, Nenadic I,
Ingianni G. Juvenile gigantomastia of extreme magnitude. A case report.
Ann Plast Surg. 2009;63:369-72.
|
|
|
 |
|
