|
|
|
Indian Pediatr 2014;51: 48-51 |
 |
Sex-specific Trends in Under-five Mortality in
Rural Ballabgarh
|
|
*Anand Krishnan, *Nawi NG, *Peter Byass, Chandrakant S
Pandav and #Suresh K Kapoor
From Centre for Community Medicine, All India
Institute of Medical Sciences, New Delhi, India; *Umeå Centre for Global
Health Research, Department of Public Health and Clinical Medicine, Umeå
University, Sweden and #Department of Community
Health, St. Stephen’s Hospital, Delhi, India.
Correspondence to: Dr Anand Krishnan, Additional
Professor, Centre for Community Medicine,
All India Institute of Medical Sciences, New Delhi 110 029, India.
Email: [email protected]
Received: May 01, 2013;
Initial review: June 04, 2013;
Accepted: July 05, 2013.
Published online: August 05, 2013.
PII: S097475591300450
|
Objectives: To assess
sex-specific differentials in child survival from 1992-2011.
Methods: We analyzed data from the electronic database of Health
and Demographic Surveillance System (HDSS) site in Ballabgarh in
North India. Results: Sex ratio at birth was adverse for
girls throughout the study period (821 to 866 girls per 1,000 boys)
and was lowest in the period 2004-2006 at 821 girls per 1,000 boys.
Overall, under-five mortality rates during the period 1992-2011
remained stagnant due to increasing neonatal mortality rate (9.2 to
27.7 P< 0.001). Mortality rates among girls were consistently
and significantly higher than boys during the post-neonatal period
(160% to 200% higher) as well as in childhood (160% to 230% higher).
Conclusions: Strategies to address the neonatal mortality and
gender differences are required for further reductions in child
mortality in India.
Keywords: Gender discrimination, Infant
mortality, Neonatal mortality.
|
|
Reducing child mortality and
gender disparities are among the keystones for achieving Millennium
Development Goals (MDGs) as enunciated by United Nations [1]. India has
achieved considerable success in reducing under-five mortality, although
it is still a long way from the MDG target of in 2015 [2].
Most efforts to reduce childhood mortality in
developing countries have focused on the causes of post-neonatal
mortality. Female disadvantage in sex ratio at birth and higher
mortality rates among girls; however, present further challenges to
child health in India [3].
The Ballabgarh Health and Demographic Surveillance
System (HDSS) site had earlier reported trends in infant mortality from
1972 to 1997 but did not focus on sex differentials in mortality, since
gender discrimination was not yet identified at that time as a major
determinant of mortality [4]. However in 2004, the site published data
on sex ratio at birth from 1991 to 2002 [5]. This paper uses the
Ballabgarh HDSS data for subsequent years to assess the progress made
since then. The objectives were to estimate the overall and sex specific
trends for mortality in different age groups during childhood including
sex ratio at birth.
Methods
The study area of Ballabgarh HDSS comprises of 28
villages, which are under demographic surveillance (a population of
85,795 in 2009). The details of the study area have been described
previously [6]. All routine information collected is updated once a month
in a computerised management information system (MIS) at Ballabgarh. The
full details of the MIS and its quality control procedures have been
described elsewhere [7].
Based on the dates of birth and death in the
database, deaths were classified as neonatal (up to and including 28
days), post-neonatal (29 to 365 days) or childhood (1 year to 4 years).
The data for eighteen years was divided into six three-year periods.
The significance of differences in mortality rates
between boys and girls in each of the three-year periods was tested
using chi-squared tests after Bonferroni correction for multiple
comparisons. We used three-year moving averages to plot curve but used
individual year data to measure the slopes of trends in mortality rate
and their significance using linear regression with year as predictor
variable and crude mortality rate as dependent variable. All the
analyses were conducted using STATA 10. The sex ratio presented is
defined as the number of female births per 1,000 male births. The study
protocol was cleared by the Institutional Ethics Committee of AIIMS.
Only secondary data without personal identifiers were used for analysis
in this study.
Results
A total of 41,678 live births (22,597 boys) were
recorded in the study area from 1992 to 2011. Sex ratio at birth was
adverse for girls throughout the study period (821 to 866 girls per
1,000 boys) (Table I). It was lowest in the period
2004-2006 at 821 girls per 1,000 boys.
TABLE I Number of Births and Sex Ratio at Birth in Rural Ballabgarh from 1992 to 2011
|
Year |
Total population
in the second year |
Female |
Total |
Sex Ratio
|
|
1992-94 |
68260 |
3,032 |
6,532 |
866.3 |
|
1995-97 |
72995 |
2,948 |
6,412 |
851.0 |
|
1998-00 |
76138 |
2,875 |
6,303 |
838.7 |
|
2001-03 |
79697 |
2,858 |
6,213 |
851.9 |
|
2004-06 |
82612 |
2,720 |
6,034 |
820.8 |
|
2007-09 |
85795 |
2,733 |
5,991 |
838.9 |
|
2010-11 |
89996 |
1,915 |
4,193 |
840.6 |
Neonatal mortality rate increased three-fold during
the study period and this was true for both boys and girls (Web
Table I). The rate increased by 1.13 per 1,000 live births
annually during 1992-2011 (P<0.001). The proportion of IMR
contributed by neonatal mortality doubled from 24.2% in 1992-94 to 53%
in 2010-11. As a proportion of all under-5 mortality, it ranged from 15%
in 1992-94 to 42% in 2007-09. The increase in neonatal mortality was
mainly due to early neonatal deaths (<7 days) in both sexes, especially
since 1998 (data not shown). Post-neonatal mortality rates declined
slightly (P>0.05) during the study period (from 28.8 to 24.6 per
1,000 live births) and the decline was similar in both sexes (Web
Table I). Girls experienced significantly higher mortality at
this age during 1995-2003 (160% to 200% higher). Post-neonatal mortality
accounted for between 37% and 47% of total under-5 mortality over time.
Childhood mortality rates showed a significant decline during the study
period (Web Table I). The decline was sharper for girls
(from 33.3 to 16.7, P < 0.002) as compared to boys (from 16.0 to
10.5, P < 0.02)
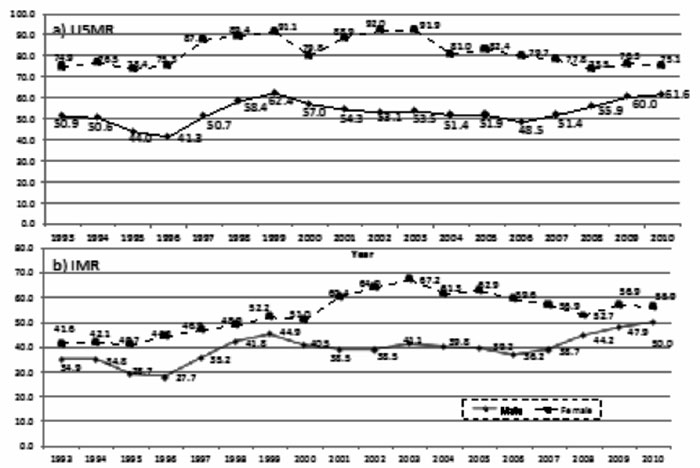
Infant mortality rates increased significantly (P<0.002)
during this period. The increase was roughly equal for both sexes. While
there was a consistently higher mortality among females (115% to 166%),
this was significant only for three time periods (1995-97, 2001-03,
2004-06). Under-5 mortality rates during the period 1992-2009 remained
more or less stagnant (P>0.05) in the population. This was due to
rising neonatal mortality rates and decreasing childhood mortality rates
and post-neonatal mortality rates. For boys there was a slight but not
significant increase in mortality rates during this period (from 50.9 in
1992-94 to 61.6 per 1000 in 2009-11). Throughout this period, females
had significantly higher under-five mortality rates, which ranged from
122% to 180% of the rate for boys. During 2004-2006, the effects of
discrimination against girls peaked.
Discussion
Using data from a population under longitudinal
demographic surveillance in a rural area of Northern India, we show that
sex differentials in mortality and an increase in neonatal mortality
during the study period present major barriers for further reduction in
infant mortality in Ballabgarh. In the study area, even during the early
neonatal period, mortality rate was skewed unfavourably for girls in
three of the six three year periods. This probably indicates more active
discrimination against girls. We have earlier reported that
significantly excess deaths in girls are due to low birth weight,
diarrhoea and malnutrition [8]. Another study among neonates showed that
even though the overall rate of perceived illness was similar in males
and females, parents preferred better health-care facilities, and spent
more on boys [9].
The increase in neonatal mortality in the study area
cannot be completely explained. During the study period at Ballabgarh
HDSS, the stillbirth rate remained fairly constant at about 2% but the
reported abortion rate increased from about 3% in the earlier years to
about 8% in the later years, probably due to earlier registration of
pregnancies and therefore subsequent abortions. Despite an increase in
institutional delivery from around 20% in mid-nineties to about 60% in
2009 neonatal mortality rates have not come down. Our initial surveys
have shown that many of these facilities do not have essential equipment
(for resuscitation, temperature maintenance) and are assisted by people
with inadequate skills for conducting delivery. Except for the change in
recent times in the study area in neonatal mortality, a higher mortality
among females at roughly the same magnitude has been reported since
mid-sixties when this project started [14].
The "One million death" study, based on a national
cluster sample in India, in 2005 reported a lower neonatal mortality
among girls (85% of boys) and a higher mortality among girls in the 1-59
months age group (135% of boys). However, the actual mortality rates
were higher than this study area [17]. The National Family Health Survey
(NFHS) data from all the three rounds covering events of a time period
between 1988 to 2005, as well as Sample Registration System (SRS) data
from 1971 to 2008, confirm a slightly lower neonatal mortality among
girls in rural India (85% to 95%) and higher mortality rates for girls
after that age group [10,11].
The data for the study were retrieved from
computerized HMIS of Ballabgarh HDSS which has maintained a longitudinal
record of all individuals residing in Ballabgarh HDSS since 1992. The
regular liaison with other community based workers, provision of health
care by the same set of workers, antenatal tracking ensure high validity
of the data collected. The study population is not necessarily
representative of the rest of the country and the experiences shared
here may not mirror the changes in the rest of the country. The issues
raised in our study are applicable to other parts of north and western
India, which are socio-demographically and culturally similar to
Ballabgarh HDSS. Sex-differential mortality occurs to some extent
throughout the country and our findings may be similar or attenuated in
other settings. However, many factors like high antenatal care and
immunisation coverage in the study area might have blunted any sex
differentials arising out of differential coverage due to these
programmes. Overall high gender bias existed in other states also
[14,15].
In conclusion, increasing neonatal mortality and
sustained excess mortality among girl children before and after birth
point to the need for new strategies for further reduction of child
mortality in Ballabgarh and rest of Northern India. A much more vigorous
social mobilization campaign on girl child using ASHAs during Village
Health and Nutrition Days and universalizing access to free care for
childhood illnesses are imperative to make sufficient progress so as to
achieve MDG4.
 |
|
Fig.1 Trends in under-five (US MR) and
infant mortality rate (IMR) in rural Ballabgarh 1992-2010.
|
Contributors: AK: Conceived the paper, analyzed
the data, interpreted the findings and wrote the first draft. Both NN
and PB: provided critical inputs for data analysis and interpretation,
revised the manuscript. Both SKK and CSP: were involved in the
initiation and maintenance of database, provided inputs for data
interpretation and reviewed the manuscript. All authors approved the
manuscript for publication.
Funding: No external funding was used for the
study; Competing Interest: None stated.
|
What This Study Adds?
• In addition to the continued higher girl
child mortality in 1-4 year period, there is evidence of a
worsening gender differential in terms of sex ratio at birth and
higher mortality even in neonatal period.
• Despite increase in institutional
deliveries, there has been no concomitant decrease in neonatal
mortality in the study population.
|
References
1. United Nations. A gateway to UN Systems work on
the MDGs. http://www.un.org/millenniumgoals/childhealth. shtml, Accessed
10 June, 2013.
2. UN Inter-agency Group for Child Mortality
Estimation. Levels & Trends in Child Mortality – Report 2011. Unicef New
York; p 13.
3. Jha P, Kumar R, Vasa P, Dhingra N, Thiruchelvam D,
Moineddin R. Low female [corrected]-to-male [corrected] sex ratio of
children born in India: national survey of 1.1 million households.
Lancet. 2006;367:211-8.
4. Anand K, Kant S, Kumar G, Kapoor SK. Development
is not essential to reduce infant mortality rate in India: experience
from the Ballabgarh project. J Epidemiol Community Health.
2000;54:247-53.
5. Bardia A, Paul E, Kapoor SK, Anand K. Declining
sex ratio: role of society, technology and government regulation in
Faridabad district, Haryana. Natl Med J India. 2004; 17:207-11.
6. Kant S, Misra P, Gupta S, Goswami K, Krishnan A,
Nongkynrih B, et al. Cohort Profile: The Ballabgarh Health and
Demographic Surveillance System (CRHSP-AIIMS). Int J Epidemiol. 2013 Apr
25. [Epub ahead of print]
7. Krishnan A, Nongkynrih B, Yadav K, Singh S, Gupta
V. Evaluation of computerized health management information system for
primary health care in rural India. BMC Health Serv Res. 2010;10:310-17.
8. Krishnan A, Ng N, Kapoor SK, Pandav CS, Byass P.
Temporal trends and gender differentials in causes of childhood deaths
at Ballabgarh, India - need for revisiting child survival strategies.
BMC Public Health. 2012 26;12:555.
9. Upadhyay RP, Rai SK, Anand K. Community neonatal
practices and its association with skilled birth attendance in rural
Haryana, India. Acta Paediatr. 2012;101:e535-9.
10. Reddaiah VP, Lobo J, Kapoor SK, Nath LM.
Comprehensive Rural Health Services Project Ballabgarh: trends in
under-five mortality. Indian J Pediatr. 1988;55:287-94.
11. Nath LM. Malhotra BD, Parmar BS. Differentials
death rates in community development Block: Ballabgarh 1966-69. Indian J
Med Res. 1974;62:211-7.
12. Million Death Study Collaborators, Bassani DG,
Kumar R, Awasthi S, Morris SK, Paul VK, et al. Causes of neonatal
and child mortality in India: a nationally representative mortality
survey. Lancet. 2010;376:1853-60.
13. International Institute for Population Sciences
(IIPS) and Macro International. 2007. National Family Health Survey
(NFHS-3), 2005–06: India: Volume I. Mumbai: IIPS. p179-190.
14. Pandey A, Choe MK, Luther NY, Sahu D, Chand J.
Infant and Child Mortality in India. National Family Health Survey
Subject Reports Number 11 December 1998.
15. Hirve S, Ganatra B. A prospective cohort study on
the survival experience of under five children in rural western India.
Indian Pediatr. 1997;34:995-1001.
|
|
|
 |
|
