|
Tuberculosis is a single major infectious
disease causing significant morbidity and mortality amongst all humans,
including children. Three sets of guidelines related to the management of
childhood tuberculosis have been produced by the various consensus groups
of the IAP since 1997(1-3), with the last one coming out in 2004(3). Cases
were classified into three categories, as per WHO and Revised National
Tuberculosis Control Program (RNTCP) guidelines. These guidelines also
addressed the issue of intermittent therapy and direct observation of
therapy.
Objectives
In consonance with the decision of Indian Academy of
Pediatrics to standardize and update the protocols for diagnosis and
treatment of childhood tuberculosis, a meeting of IAP Working Group was
held in Mumbai on 26th and 27th April 2008. Members of the Group were
given individual responsibilities to review the existing literature on
different aspects of the childhood TB and present the review to the Group.
The Group deliberated in the light of presentations made by the members,
based on literature reviewed, and developed a consensus for the topics
covered.
The deliberations were than written as a draft document
and circulated to all the members for review. The Group also informally
interacted with the different national and international bodies that were
also working on developing guidelines for TB management to incorporate the
latest changes that were in the offing. Efforts were made to ensure that
the recommendations are standardized for reasonably accurate diagnosis and
rational treatment of childhood TB.
Recommendations
1. Pulmonary Tuberculosis – When to Suspect?
Fever and/or cough of recent onset lasting for >2 weeks
should arouse suspicion of tuberculosis. It is important to document fever
and not depend merely on impression. Fever can be of any type and the
often-described evening rise of temperature is neither specific to this
etiology nor commonly present. Cough can be dry or moist and may be
severe. Cough persisting beyond 2 weeks, particularly as an only symptom
in an otherwise healthy child can be due to viral infection and is often
not due to TB. Such children, therefore, do not always warrant
investigations. Recurrent symptoms with normal intervening period are less
likely to be due to tuberculosis. Recent loss of appetite may be relevant
but unexplained recent loss of weight can be an important pointer to the
suspicion of tuberculosis. A static weight/not growing well are not
significant pointers to this disease. History of contact with an
infectious TB patient (smear positive) should always prompt detailed
examination for likelihood of the disease. However, in a symptomatic
child, contact with a person with any form of active tuberculosis within
last two years may be significant.
Diagnosis is also more likely in presence of risk
factors such as recent history of measles or whooping cough and immuno-compromised
state including steroid therapy. Persistent lower respiratory infection
not responding to antibiotic therapy may point to a probable diagnosis of
tuberculosis. Significant superficial lymphadenopathy must be specifically
looked for, as it may often coexist.
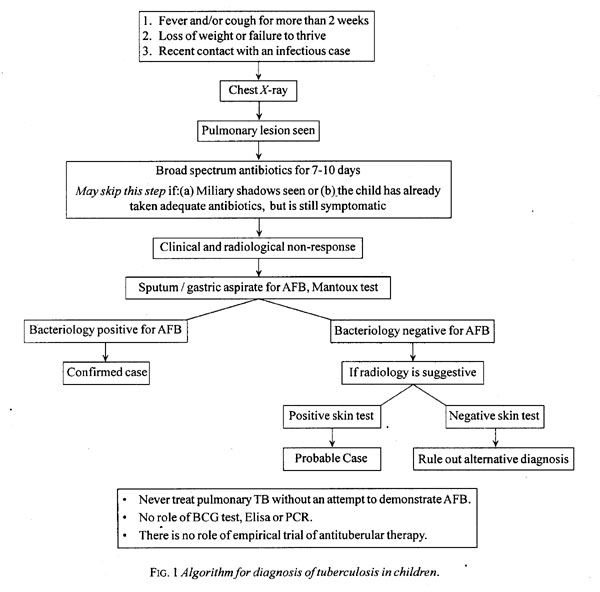
For a clinically suspected case, further investigations
are necessary. Diagnosis of tuberculosis should never be made only on
clinical features. The above-mentioned features in isolation or in
combination should only make you suspect TB. Therapeutic trial with
anti-TB drugs is, therefore, not recommended and instead, every attempt
must be made to prove the diagnosis.
Figure 1 depicts the diagnostic
algorithm for pulmonary tuberculosis in a child.
2. Tuberculin Test
The standard tuberculin test recommended for use is the
Mantoux’s test. Commercially available tuberculin in the country are 1, 2
and 5 Tuberculin Unit (TU) PPD (RT23 equivalent). It is important to raise
a wheal of about 6 mm after the intra-dermal injection and the test is
read 48-72 hours after an injection. Ballpoint or palpatory methods are
used to read the induration.
The width of reaction (induration) in the horizontal
plane is noted for interpretation (see annexure for details).
Mantoux’s test or PPD skin test is considered positive if the induration
is 10 mm or more. This cutoff was recommended using a 1 TU PPD RT23.
Currently the laboratories more often use 5 TU PPD
(RT23 equivalent), or sometimes even some other higher strengths or types
of PPD are used. The standard cut off of 10 mm can actually not be
justified for any higher strength of PPD used. The reaction evoked is not
only dependent on the amount of antigen given but also does not have a
linear relationship with the increasing strengths. Therefore, the current
practice may actually lead to an increase in false positive reactions
using the 10mm cutoff with the higher strength of PPD. The Group
recommends that the 10mm cutoff may be continued to use for strengths of
PPD only up to 5TU. Efforts should be made to use only 1 TU PPD to
decrease the false positives(4) and in no case strength higher than 5 TU
should be used. Degree of reaction, including necrosis and ulceration, may
not necessarily differentiate infected from diseased. Prior BCG vaccine
has minimal influence on PPD reaction(5,6).
If the patient returns for reading beyond 72 hours but
by 7th day, a positive test can still be read. A repeat test may be
needed, if there is no induration and the suspect presents beyond the
stipulated time for reading. Repeat tuberculin test when required should
preferably be done on the other arm. The reading of the same should be
interpreted as in any other individual.
3. BCG Test
BCG test is not recommended for diagnosis of
tuberculosis(7).
4. Chest Radiograph
Chest radiograph merely localizes the site of pathology
and not etiology. There are no pathognomonic radiological signs of
tuberculosis. In relevant clinical setting, certain radiological lesions
may strongly suggest tuberculosis and they include miliary, hilar or
paratracheal lymphadenopathy with or without parenchymal involvement and
fibrocaceous cavitatory lesions. Rarely chest X-ray may be normal,
such cases should be referred to an appropriate center for further
detailed investigations if the clinical suspicion is high.
In clinical practice, non-resolving chest shadows
despite adequate antibiotic therapy in a symptomatic child raises the
possibility of tuberculosis. It is worth mentioning that all persistent
radiological lesions are not necessarily due to TB. Asymptomatic patients
may have persistent shadows due to parenchymal scarring, pleural
thickening, and healed fibro-atelectatic changes. On the other hand, a
child with bronchiectasis or an interstitial lung disease may have
presence of non-resolving shadows with persistent symptoms.
Ultrasonography of chest is helpful to assess pleural
fluid collection; although decubitus chest X–ray film may also
reveal similar information. CT scan is rarely necessary and is not cost
and radiation effective. Chest CT scan, however, may offer an opportunity
for CT guided biopsy for tissue diagnosis.
5. Bacteriology
Demonstration of AFB from any body fluid or tissue is
the gold standard of diagnosis of tuberculosis. Such a proof is often
lacking in childhood tuberculosis because of difficulty in collection of
sputum and due to paucibacillary primary disease in children. However,
studies do report that the yield of a positive test in advanced cases may
be as high as in adults.
Few studies have reported as high as 33%
bacteriological positivity even in primary disease such as hilar
adenopathy(8,9). Therefore, every attempt must be made to
bacteriologically prove the diagnosis in every case of suspected
tuberculosis.
Early morning gastric aspirate is a preferred specimen
for most young children with suspected TB for detecting AFB or isolating
M. tuberculosis. The child is kept fasting for about 6 hours (at
night) and an appropriate size intra-gastric tube is passed in the
morning. Initially the aspirate is drawn from the stomach and then a
further washing with 15-30 mL saline is taken. The contents so recovered
are then immediately transferred to the laboratory. This specimen can also
be collected as an ambulatory procedure after 4-6 hours fasting(10).
Sputum collection is possible in older children with extensive and
cavitatory disease, particularly if the patient has a wet cough. Induction
of sputum by 3% nebulized hypertonic saline can be tried in older children
(after the age of 4 months). The patient is pretreated with nebulized
bronchodilators prior to induction. Following saline nebulisation, chest
physiotherapy is done to loosen up the secretion and the samples are
collected from the throat or nasopharynx(11). Whatever method one chooses
to use, one needs to collect at least two, preferably three, samples.
Where the facilities are limited, these tests may be
prioritized and atleast be done in all children with wet cough or children
who have definite parenchymal lesion on chest skiagram. Experience with
bronchoscopy and bronchoalveolar lavage (BAL) as a diagnostic tool is
limited but it is often needed when evaluating persistent pneumonia. TB
remains an important cause of persistent pneumonia in our country(9).
Ziehl-Neelsen stain can reveal AFB only if sample
contains >10,000 bacilli per mL. Different culture methods are used, such
as LJ medium, Radiometric (Bactec) and Non-radiometric (MGIT) can be used
for confirming diagnosis in pauci-bacillary state. The newer methods are
capable of giving faster results and may be used if available.
Mycobacterial culture assumes special significance in case of suspected
drug resistance.
6. Serodiagnostic Tests
As mycobacterial antigens overlap in different stages
of infection and disease, there are no specific antigens that can confirm
natural infection or active disease. Besides, antigen tests vary widely
and are often negative in paucibacillary disease. Antibody tests share
similar problems for interpretation and in addition cannot differentiate
natural infection from BCG vaccine induced infection and active disease
from old healed disease.
Thus both antigen and antibody TB ELISA tests are
poorly sensitive and specific and are not recommended for diagnosis of
tuberculosis(12).
7. Interferon Gamma Release Assays (IGRAs)
A newer generation of tests which measure the
production of interferon gamma by the peripheral mononuclear cells have
been developed to identify the patients with TB disease or latent
infection. These use two antigens, early secretion antigen target (ESAT 6)
and culture filtrate protein 10 (CFP 10), which are specifically present
only in Mycobacterium tuberculosis and not in other mycobateria or
the BCG vaccine strain. These tests though have a principle similar to
skin test but do away with the need for a repeat visit by the patient for
reading purposes(13). Quantiferon Gold and T spot are two of the
commercially available IGRAs. These are being used in place of the skin
test in low prevalence countries to detect latent TB infection. However,
these expensive tests do not differentiate the TB infection from disease.
Its exact utility in high burden situation is still not clear(14,15).
8. PCR Test
Nucleic acid amplification tests using polymerase chain
reaction (PCR) cannot differentiate living from dead bacilli and so
continues to be positive even after successful treatment. PCR is positive
in 95% to 100 % of culture positive cases but only in 50% to 60% of
culture negative cases. It may be false positive in 1% to 30% of cases.
Thus, no decisions can be made only on the basis of PCR tests and hence
these tests are not recommended in clinical practice(16).
9. Extra-pulmonary Tuberculosis
TB lymphadenitis
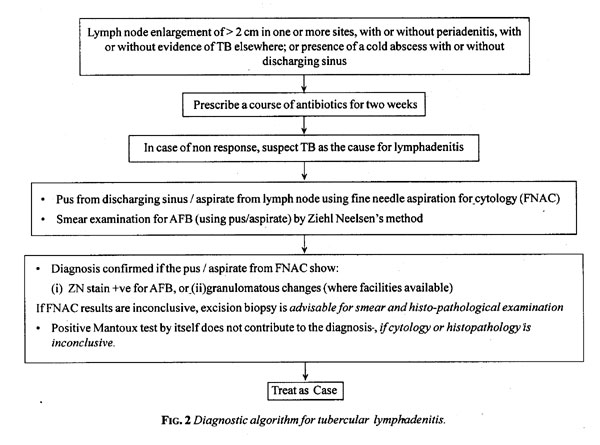
Clinical correlate of diagnosis includes progressive
enlargement of lymph node for more than 2 weeks, firm, minimally tender or
non-tender, fluctuating, further may get matted and develop chronic sinus
formation.
Mantoux test is positive in a significant proportion.
Fine needle aspiration cytology (FNAC) is usually adequate for accurate
diagnosis and it correlates well with biopsy in >90% of cases(17,18).
Histopathology, typically shows necrosis and epitheloid granuloma. It is
important to look for AFB in FNAC specimen and it may be positive in
20-70% of patients. When FNAC is inconclusive, biopsy is necessary for
confirmation of diagnosis. In children lymphadenopathy is common due to
recurrent tonsillitis and upper respiratory tract infections. Reactive
lymphadenitis may clinically mimic tuberculosis but do not warrant anti-TB
drugs. Hence, anti-TB drugs should not be given unless the diagnosis of TB
is confirmed by FNAC or histopathology. Figure 2 depicts a
diagnostic algorithm for tubercular lymphadenitis.
Pleural effusion
If chest X-ray is suggestive of pleural
effusion, pleural aspiration should be performed for biochemical,
cytological and smear examination by Ziehl-Neelsen stain to confirm the
diagnosis. Typically, a tubercular effusion fluid is straw colored (pus,
if aspirated, is very rarely due to TB etiology) has large numbers of
cells (in hundreds; predominantly mononuclear), with high proteins (>3g/dL).
ADA levels over 60 IU/L may be suggestive of tubercular pleural effusion
but are not diagnostic of TB(19,20). Pleural biopsy may be performed,
where available, particularly when the fluid aspirate findings are
inconclusive.
Tubercular meningitis
Children with tubercular meningitis (TBM) present with
a longer (>1 week) duration of fever, with vague CNS symptoms such as
behavior changes, irritability, drowsiness, headache, vomiting and
seizures. Physical examination typically reveals global encephalopathy
with focal deficits, hydrocephalus and movement disorder. Risk factors for
TBM include age <5 years, contact with an adult suffering from
tuberculosis, PEM grade III and IV, and HIV infection.
Typically CSF is clear, usually does not show very high
cell count (under 500 cells/cumm) with lymphocytosis. Biochemical
investigations reveal increased proteins and mild reduction in glucose.
The typical CSF picture may, however, not always be seen. Furthermore, the
typical CSF picture described above can also be mimicked by partially
treated pyogenic meningitis. In such a situation, CSF can be repeated
after 48-72 hours of treatment with a fresh set of broad spectrum potent
antibiotics to evaluate change in clinical status as well as in CSF.
During this time, efforts are made to establish the diagnosis by
collecting more evidence using PPD, chest skiagrams, and bacteriological
diagnosis from appropriate samples including CSF. Many a time concomitant
TB lesions elsewhere in the body (say, pulmonary) co-exist and can clinch
the diagnosis. Mycobacterial culture from CSF should also be attempted but
CSF culture has poor sensitivity (16%) though specificity is high (90%).
Neuroimaging is an important diagnostic modality. It
may reveal one or more of the following findings: basal meningeal
enhancement; hydro-cephalus with or without peri-ventricular ooze;
tuberculoma(s); or infarcts may be seen in different areas, especially in
basal ganglia.
Normal CT scan does not rule out TBM and in case of
strong clinical suspicion of diagnosis, a repeat follow-up CT scan after
few days may show newly developing lesions. CSF abnormalities in TBM may
take variable time up to few months to return to normal. Besides routine
CSF examination. CSF ADA is high in TBM. Various studies have a cut-off
point between 7 and 11.3 IU/L for diagnosis. This may offer supportive
evidence in favor of TBM but should not be taken in isolation(21). CSF
antigen and PCR tests are neither routinely available nor reproducible.
They are, therefore, not recommended. CSF antibody tests have poor
sensitivity and specificity and hence are not useful.
Tuberculoma
Often seen in older children, it may present as a focal
seizure in supra-tentorial cortical lesion or with symptoms and signs of
raised intracranial tension with multiple localizing signs and
hydrocephalus in posterior fossa lesion. It may sometimes also be seen as
a part of TB meningitis.
Differentiation from other ring lesions, especially
neurocysticercosis (NCC) is difficult in cortical lesion. A ring enhancing
lesion is not pathognomonic of tuberculoma. A larger lesion >20 mm, disc
lesion or ring lesion with thicker rim with central nodule favors
tuberculoma; while multiple, smaller, thin rim with epicentric nodule
favor NCC. MR spectroscopy may help in diagnosis of tuberculoma as it
shows lipid peak.
Abdominal tuberculosis
It may present as localized disease such as mesenteric
lymphadenopathy, intestinal disease, peritoneal involvement or systemic
disseminated disease presenting as hepatosplenomegaly. Large matted lymph
node mass may be clinically evident and ultrasound guided biopsy may help
in confirming the diagnosis.
There are no standard guidelines for sonography
diagnosis of abdominal tuberculosis. However, corroborative evidence
includes: echogenic thickened mesentery with lymph nodes >15mm in size;
dilated and matted bowel loops; thickened omentum, and ascites(22). Barium
follow-through examination may be suggestive of intestinal disease but is
not confirmatory. Exudative peritoneal disease presents as ascites that is
often clinically evident. The ascetic tap should always be done in such
situations and the fluid tapped is an exudate, typically showing
lymphocytic predominant cellular response with high proteins (>3g/dL).
10. Treatment of Tuberculosis
Basis of pharmacotherapy
Choice of anti-TB drugs is based on several
determinants such as bacillary and metabolic subpopulation, bacillary
load, drug resistant strains, lag period of bacterial population,
pharmacokinetic profile and pathological factors. There are different
types of bacillary population in every case of tuberculosis and hence
drugs are selected in a combination to attack entire (extra-cellular and
intra-cellular, slow and rapidly growing) bacillary population for
successful chemotherapy. Isoniazid (INH) and rifampicin (RMP) kill the
fast growing bacilli, pyrazinamide (PZA) acts against intracellular
organisms in acidic medium while extracellular slow growing bacilli are
best killed by RMP. Thus every case of tuberculosis must be treated at
least with these three drugs. The chances of naturally occurring mutants
are higher if the bacillary load is more and therefore, such cases need
more drugs in intensive therapy, say as in smear positive cases.
As dividing time of TB bacilli is about 21 hours, all
the drugs are administered in such a way that they achieve peak
concentration all at one time so as to hit bacilli hard. The drug
concentration is poor in caseum and sequestrated tissue, so these should
be removed surgically wherever feasible.
Mycobacterium tuberculosis when exposed to certain
concentration of most currently used anti-TB drugs in vitro shows
an inhibition of growth for 1 to several days. This suggests that the
drugs can be effective even when used on an intermittent basis as a
continuous high serum level of these drugs is not needed. This forms the
basis of intermittent therapy. While RCTs in children using thrice weekly
regime are awaited, RCTs from adults as well as observational studies
including programmatic data in all age groups have shown that intermittent
thrice a week therapy with higher dose is as effective as daily therapy
with conventional dose and is an effective alternative(23). However,
intermittent therapy is not safe when self-administered, as there is no
margin for any error in taking medications. The directly observed therapy
under DOTS takes care of the adherence issues and therefore uses thrice a
week intermittent therapy.
Anti-tubercular therapy
The appropriate management of tuberculosis requires
assessment of the patient correctly with respect to the site of disease,
bacteriological status, treatment type of patient and the severity of
disease. These definitions are detailed in Table I. After
appropriately defining the disease, the patient is then categorized to
receive appropriate anti- TB therapy (Table II). The drug
dosages are given in Table III.
TABLE I
Definitions for Categorizing for Treatment of Pediatric Tuberculosis
| A. Case definitions for site Pulmonary:
Refers to disease involving lung parenchyma. Extra Pulmonary: Refers
to disease involving sites other than lung parenchyma Both pulmonary
and Extra pulmonary constitutes Pulmonary Extra- Pulmonary involving
several sites is defined by most severe site.
B. Case definitions for severity
Pulmonary TB
Severe Pulmonary TB
Less severe Pulmonary TB
All other except PPC e.g.
• Primary Pulmonary complex (PPC)
o Progressive primary disease
o Fibro-cavitatory disease
o Miliary
Extra-Pulmonary TB
Severe Extra-Pulmonary TB
Less severe extra-pulmonary TB
Meningitis Spinal or Bone or Peripheral joints • Single
Lymph node site
Bilateral or extensive pleural effusion
• Unilateral pleural effusion
Intestinal
Genitourinary
Peritonitis
Pericarditis
Adrenal glands
C. Case definition for bacteriology
Smear positive- Sputum / Gastric aspirate /BAL/any other
tissue or fluid
Any sample positive for acid fast bacilli on staining
Smear Negative - None positive
D. Type of patient as per history of previous ATT
New Case: A patient who has had no previous ATT or had it for less than 4
weeks.
Relapse: Patient declared cured/completed therapy in past and has evidence
of recurrence.
Treatment Failure: Patient who fails to respond/deteriorates after 12
weeks of compliant intensive phase.
Treatment after default: A patient who has taken treatment for at least 4
weeks and comes after interruption of
treatment for 2 months and has active disease. |
TABLE II
Treatment Categories and Regimens for Childhood Tuberculosis
|
Category of |
Type of patients |
TB treatment regimens |
|
treatment |
|
Intensive phase |
Continuation phase |
|
Category I |
• New smear-positive pulmonary
Tuberculosis (PTB) |
HRZE (2 mo) |
HR (4 mo) |
|
|
• New smear-negative severe forms
of PTB |
|
|
|
|
• New severe forms* of
extra-pulmonary TB |
|
|
|
Category II |
• Smear-positive relapse, treatment
failure or |
|
|
|
|
treatment after default |
|
|
|
|
• Cases who are smear negative but
considered to have |
SHRZE (2mo) |
HRE (5 mo) |
|
|
relapse, treatment failure
or defaulted |
+HRZE (1 mo) |
|
|
Category III |
• Less severe forms of pulmonary TB* |
HRZ (2 mo) |
HR (4 mo) |
|
|
• Less severe forms of
extra-pulmonary TB* |
|
|
|
H=INH, R= Rifampicin, Z= Pyrazinamide, E=
Ethambutol, S= Streptomycin; *Refer Table 1 for details of severity
In patients with TB meningitis on Category I
treatment, the four drugs used during the intensive phase can either
be HRZE or HRZS. The present evidence suggests that ethambutol can
be used in children; Continuation phase of treatment in TB
meningitis, miliary and spinal TB with neurological complications
should be given for 6 - 7 months, extending the total duration of
treatment to 8 - 9 months. Under Revised National Tuberculosis
Program (RNTCP) all patients shall be covered under directly
observed intermittent (thrice weekly) therapy. While the supervised
therapy is considered the most optimal treatment, this very same
combination of drugs can also be used on a daily basis, for a
similar duration, in case the treatment is being given unsupervised.
It is important to ensure completion of treatment in every case put
on treatment to prevent emergence of resistance, particularly to
rifampicin. |
TABLE III
Dosage and Adverse Effects of Anti-tuberculous Drugs
|
Drug (symbol) |
Daily |
Maximum |
Intermittent |
Maximum |
Major side effects |
| |
dosages |
per day |
thrice |
per day |
|
| |
per kg |
dose (daily |
weekly |
dose (inter- |
|
| |
body |
regime) |
dosage |
mittent |
|
| |
weight |
|
as under |
regime) |
|
| |
|
|
RNTP |
|
|
| |
|
|
per kg body |
|
|
| |
|
|
weight |
|
|
| Streptomycin*(S) |
15-20 mg |
1000 mg |
20 mg |
1000 mg |
tinnitus |
| Rifampicin (R) |
10 mg |
600 mg |
15 mg |
600 mg |
hepatotoxicity, gastritis, flu like illness |
| Isoniazid (H) |
5-10 mg |
300 mg |
15 mg |
600 mg |
peripheral neuropathy, hepatotoxicity |
| Pyrazinamide (Z) |
30-35 mg |
2000 mg |
35 mg |
2000 mg |
arthralgia, hepatotoxicity |
| Ethambutol (E) |
20 mg |
1000 mg |
30 mg |
1200 mg |
oculotoxicity |
The Group agreed to include all children with extensive
pulmonary lesions (any thing beyond the primary pulmonary complex) under
Category I because of the evidence and experience that a significant
proportion of these turn out to be smear positive when diligent efforts
are made. It is only milder forms of the disease, also more likely to be
paucibacillary, such as primary complex (mediastinal or hilar
lymphadenitis with or without a parenchymal lesion, Single site peripheral
lymphadenitis and unilateral pleural effusion that are treated as Category
III(24).
In case of delayed response to assigned therapy,
intensive phase may be prolonged by one more month in Category I and II.
Similarly, continuation phase may have to be prolonged by 3 months for TB
meningitis, miliary and spinal TB. There are studies to suggest that 6
months therapy may be adequate in these situations as well . Yet, the
group felt that the prolongation of the continuation phase is justified in
these situations as (a) the lesions may take longer to sterilize in
such pathology, and (b) due to the risk of serious morbidity
associated with relapse.
Category II therapy utilizes all the first line drugs
as it is used to treat relapsers, treatment defaulters and treatment
failures who are more likely to have drug resistance. It is generally
considered to add two drugs to the failed regime till culture and drug
sensitivity reports are available. However, this categorization can also
mean addition of a single drug – Streptomycin – to a failed regime (say a
Category I failure). Evidence suggests that most common drug resistance is
limited to first line drugs singly or in combination, and the multidrug
resistance with bacilli resistant to at least INH and rifampicin is
relatively uncommon (<5%). There-fore, except for multidrug resistance,
this regime would work well for most. Complete adherence to therapy being
the key to achieving cure and decrea-sing the chances of development of
resistance, this is imperative that the treating pediatrician makes all
efforts to ensure compliance. DOTS provide, a great opportunity for the
same. Patients who are non-responsive to a well-supervised category II are
likely to have MDRTB and should therefore be referred to an appropriate
facility.
The above definition, categorization and duration of
therapy should be used for every child with TB whether the patient is
under individual care or under the program. This protocol should form the
current standard of care and should override all earlier recommendations.
Steroids in tuberculosis
Definite indications for concomitant steroid therapy
include TBM and pericarditis. Steroids are routinely not indicated in
lymphadenitis and pleural effusion. They may be used in endobronchial
tuberculosis or mediastinal compression syndrome due to tuberculosis,
pleurisy with severe distress and miliary disease with alveolo-capillary
block. Predinsone 2-4 mg/kg/d or its equivalent is used for 2-4 weeks and
then tapered over next 2 weeks.
Fixed drug combination (FDC)
These combinations contain 2 or more drugs in a single
formulation and therefore simplify the prescription of drugs. More
importantly, they limit the risk of drug-resistant tuberculosis arising as
a result of inappropriate drug selection due to prescription errors or due
to omission of some drugs by the patient. FDC is patient friendly but
there are some relevant issues about them. Bioavailability of liquid
formulations is not dependable. One of the problem with FDC is that it is
"fixed" and makes titration of individual drug dosage difficult. While the
combination of rifampicin and INH as a single formulation are still well
accepted, the bioavailability of individual components, particularly
rifampicin, may be affected in other 3 or 4 drugs FDC formulations. It is
reported that in most situations, blood levels of the drugs are inadequate
because of poor drug quality rather than poor absorption(25). Currently,
there are several formulations available with varying combinations with
confusing and similar sounding brand names. This could make the
prescription not simplified but error prone. FDCs from standard
manufacturers with proven bioavailability should only be used.
Control Program-RNTCP
TB is considered a global emergency and in countries
like ours, despite effective chemotherapy, control has not been achieved
due to poor therapeutic practices. The emerging threat of poorly treatable
rifampicin resistant TB warrants that the first line drugs be used
appropriately to give them longevity in the armamentarium. RNTCP has
evolved to take care of these problems by using DOTS strategy(26,27). This
includes quality diagnosis by sputum microscopy, supervised drug therapy
(thrice weekly visits in intensive phase followed by weekly visit to the
clinic during continuation phase when one dose is administered under
supervision and two doses are given to the patient to be taken at home
subsequently), regular drug supply, patient tracking (progress to be
monitored till end of therapy) and administrative and political
commitment. Each patient on diagnosis has an entire box of drugs allocated
with his name on it, though not handed over, to ensure supervised
uninterrupted therapy. The Indian program is the first program in the
world to provide pediatric patient-wise boxes for childhood TB cases and
the pediatricians should help their patients in using these facilities.
11. Chemoprophylaxis
It is estimated that in developing countries the annual
risk of tuberculosis infection in children is 2- 5%(28). The estimated
lifetime risk of developing tuberculosis disease for a young child
infected with Mycobacterium tuberculosis as indicated by positive
tuberculin test is about 10%(29).
About 5% of those infected are likely to develop
disease in the first year after infection and another 5% in rest of their
lifetime. These rates increase in HIV infected individuals. Nearly 8-20%
of the deaths caused by tuberculosis occur in children(30). The age of the
child at acquisition of tuberculosis infection has a great effect on the
occurrence of tuberculosis disease.
Approximately 40% of infected children less than 1 year
of age, if left untreated, develop radiologically significant
lymphadenopathy or segmental lesions compared with 24% of children between
1-10 years and 16% of children 11-15 years of age(31).
Six months of chemopropylaxis is recommended for all
under 6 years age contacts of an infectious case, irrespective of their
BCG or nutritional status. PPD positive children over 6 years of age and
who do not have any evidence of active disease but are planned for
immunosuppressive therapy (e.g. children with nephrotic syndrome, acute
leukemias, etc) may also be given the benefit of chemoprophylaxis. While
there is evidence that HR combination can make the prophylaxis shorter (3
months) but the group does not recommend this due to the risk of misuse of
rifampicin.
12. Follow-up
With correct evaluation of type of patient, site and
severity of disease and compliant treatment, one can anticipate clinical
and radiological improvement over a standard time frame. Symptoms of
active disease such as fever, cough and loss of appetite usually disappear
within 2-4 weeks. Weight gain is evident only if active disease had
resulted in loss of weight. Children often do not loose significant weight
and so would not show weight gain even after successful treatment.
The present evidence does not suggest any cost benefits
of repeating X-ray chest at the end of intensive phase, if the
clinical improvement is on expected lines. Few patients who have
persistence of symptoms on therapy will need investigations for
bacteriological and radiological response. They should be given the
benefit of extension of intensive phase by 4 weeks provided alternative
diagnosis and co-morbidities are ruled out.
At the end of stipulated therapy, patient must be shown
to have achieved cure by demonstrating negative bacteriology. A chest
radiograph at the end of treatment is desirable to document the
radiological status. This may be helpful to diagnose any subsequent
disease in this high-risk group.
Repeat chest X-ray may sometimes be considered
early in case of unanticipated clinical progress. In the presence of
clinical improvement but radiological persistence of lesion, it is best to
wait for radiological clearance over time, as it may not signify active
disease. The patient should be followed up every 3 months for at least one
more year for a possible relapse.
Paradoxical upgrading reaction (PUR) – worsening of
lesion on treatment or appearance of new lesion is often seen in TB
irrespective of HIV co- infection. Immune reconstitution syndrome occurs
in individuals on treatment with HAART.
Routine monitoring of liver transaminases in patients
on ATT is not recommended though hepatitis is the commonest serious drug
toxicity seen. As the anti-TB drugs are hepatic enzyme inducers,
asymptomatic biochemical derangement without increase in billirubin level
may be tolerated till the enzymes remain up to 5 times the normal range.
However, if patient develops jaundice or other signs of liver dysfunction
during therapy, it is prudent to stop ATT immediately irrespective of
enzyme levels. The drugs are withheld till the serum bilirubin becomes
normal and the enzymes also start touching the normal range. Although many
patients with drug-induced hepatotoxicity can be success-fully
rechallenged, this is best done in a place where liver function can be
carefully monitored. The drugs should be re-introduced in sequential order
starting with rifampicin, followed by isoniazid and then pyrazinamide. We
add the first drug and reassess for its impact on liver enzymes. If the
enzymes remain within the acceptable range, then only the subse-quent
drugs are added in the given sequence every 5-7 days. Some experts prefer
building up the doses of each of the drug; starting with half the dose and
then increasing to full dose after 3-4 days, and then adding the next drug
in half the dose and continuing the same way till all the drugs are
re-introduced. Drugs causing severe intolerance on reintroduction are best
avoided and substituted with other drugs. If the period without drugs is
likely to be prolonged, and the patient is sick and requires treatment, at
least two other drugs (e.g. streptomycin, ethambutol,
floroquinolones) should be given until it is determined whether the
offending drug can be resumed. All patients who require alteration from
the standard regimen should be referred to experienced pediatricians.
Efforts should be made to ensure drug adherence in
every patient. If the patient is under non-DOTS treatment, then the
treating pediatrician should monitor adherence to therapy and followup. At
each visit a pill count or prescription review should be done with the
patient or the caregiver. It is very important to realize that the
emergence of multidrug resistant TB (MDR TB) is always a man made problem
and failure of the patient to complete the prescribed course completely
and adequately is one of the major reasons. When you have a patient who
has returned after a break in therapy, further management becomes
difficult. Table IV details the guidelines for treatment
after a period of interruption in therapy. Whenever treatment is
interrupted for more than 2 wks, the child should be reassessed clinically
and radiologically, with bacteriological examination, wherever possible.
In all such cases the resumption of treatment must be preceded by
evaluation for activity and investigating the causes for non-adherence.
The pediatrician should not merely restart the treatment but also enable
the completion of treatment by addressing issues related to non-adherence
in the first instance. Addressing issues like side effects of the therapy
(real or perceived), cost involved as well as educating about the need for
a complete treatment even after the symptoms abate may help adherence.
Both the child as well as the caregivers must be involved in decision
making for re-initiating treatment.
TABLE IV
Managing Patients with Interruptions in Treatment
| Duration of therapy |
Duration of interruption |
Decision |
| Upto 4 weeks |
<2 weeks |
Resume original regime |
| |
> 2 weeks |
Reassess and start treatment again |
| 4-8 weeks |
<2 weeks |
Resume original regime |
| |
2-8 weeks |
Extend intensive phase by 1 month more |
| |
>8 weeks |
Category II if diagnosis is still TB |
| > 8 weeks |
<2 weeks |
Resume original regime |
| |
>2 weeks |
Review activity |
| |
|
• continue same treatment if no active disease |
| |
|
• Category II therapy for active diseases |
13. Special Situations
When to suspect MDRTB
It may be suspected prior to starting therapy in case
of contact with proven MDRTB. It is also likely in a child who has had one
or more courses of ATT in the past or had been non-compliant with
prescribed therapy. Persistence of positive sputum or symptoms after
extended intensive phase (3 months) in spite of compliant therapy should
alarm you to the possibility of drug resistant TB and all necessary
cultures should be sent while the patient is put on Category II therapy.
The patients who are non-responsive to a well-supervised Category II are
likely to have MDRTB and should therefore be referred to an appropriate
facility.
Multi-bacillary lesions are more likely to be drug
resistant than paucibacillary. HIV infection by itself does not predispose
to MDRTB but the MDRTB prevalence is higher in such cases due to several
factors. Malabsorption of anti-TB drugs in such patients may lead to
suboptimal concentration of drugs in spite of compliance. Due to frequent
hospital visits, they may also come in contact with MDRTB.
The treatment of MDRTB should only be done by experts.
The details of the management of MDR TB in children are beyond the scope
of this consensus guidelines.
When to consider HIV testing
Clinical markers of HIV infection such as oral thrush,
chronic diarrhea, clubbing of nails, herpes infection, failure to thrive,
require HIV testing. Beside these, history of HIV infection in parents and
past history of blood transfusion justifies HIV testing. In case
tuberculosis in a child does not respond as anticipated to compliant
treatment, HIV infection may be one of the causes. HIV testing may be
considered, especially if there is no other cause for poor response to
treatment.
Management of a neonate born to a mother with
tuberculosis
Prophylactic INH is recommended for newborns born to
mother with tuberculosis after ruling out congenital tuberculosis. Modern
chemotherapy is so efficacious that separation of the mother and infant is
no longer considered mandatory, once the mother’s therapy is started.
Separation should occur only if the mother is ill enough to require
hospitalization, if she has been or is expected to become non-adherent to
her treatment, or if she is infected with a drug resistant strain of M.
tuberculosis. INH therapy should be continued in the infant at least
until the mother has been shown to be non infectious (culture negative)
for 3 months. The infant should receive INH for a total of 6-9 months.
Vaccination with BCG appears to decrease the risk of tuberculosis in
exposed infants, but the effect is variable. The mother can continue to
breast feed the baby. The ATT excreted in the milk has no therapeutic or
adverse effect on the baby. Appropriate cough hygiene should be observed
by the mother.
14. Gaps in Knowledge
The group identified the following key research areas
which can provide answers to some of the unresolved issues.
1. Feasibility and utility of induced sputum in
children.
2. Tuberculin test and redefining cutoff values for
diagnosis of infection with the different strengths and formulations
available.
3. Role of gestric aspirate in ambulatory setting.
4. Role of Interferon gamma release assays in
diagnosis and assessment of activity in children.
5. Possibility of shorter duration of ATT for CNS/
renal and bone and joint TB by RCTs.
Finally, in conclusion we submit that the current
guidelines have been developed keeping in mind the earlier guidelines of
IAP, the National program guidelines and the International standard for TB
care. We hope that these guidelines will henceforth form the basis of
childhood TB management in the country in both public and private sectors.
Writing committee: YK Amdekar, Varinder Singh,
Sushil K Kabra and GR Sethi. Following members attended the meeting(s): YK
Amdekar: Convenor; Varinder Singh, G.R. Sethi, Sushil Kabra, Mahesh Babu,
D Vijayasekaran, Joseph Mathews, RK Agarwal; President IAP 2008, Panna
Choudhury: President elect IAP 2008; and Rohit Agarwal: Secretary General
IAP 2008.
Funding: The meeting of the group was
facilitated by an academic grant from M/s Lupin Pharma.
Conflict of Interest: None stated.
|
Annexure
Tuberculin test
Purified protein derivative (PPD) solution must
be kept refrigerated at 2-8 °C
and to avoid fluctuations in temperature, never store in the
refrigerator door. The vial should be discarded if it has been open
for more than 30 days or the expiration date has passed. Select a
well-lit area for administering the test.
Administration of Skin Test
The patient’s forearm is exposed with the
palm-side-up and slightly flexed at the elbow. The injection is to
be given about 2 to 4 inches below the elbow avoiding areas of skin
with veins, sores, rashes, scars, or excess hair. Using standard
precautions for injection safety, the injection site is cleaned with
alcohol swab, using circular motion beginning in the center and
working the way outward.
The 1mL tuberculin syringe is loaded with PPD
just prior to administration ensuring that all air and excess
solution is expelled from the syringe, leaving exactly 0.1 mL of
tuberculin solution in the syringe.
The skin is stretched taut over the injection
site to provide a surface that is easy for the needle to penetrate.
The syringe is held between thumb and index finger with the needle
bevel facing up and the syringe parallel to the forearm. With the
needle against the patient’s skin, the needle is inserted slowly at
a 5- to 15-degree angle, just below the surface of the skin (one
should be able to see the bevel of the needle just below the skin
surface). Once the bevel of the needle has fully entered just
beneath the superficial most part of the skin, the stretched skin is
released holding the syringe in place. The tuberculin solution is
then injected slowly forming a 6 to 10 mm wheal (pale, raised area
with distinct edges; has orange peel appearance and does not
disappear immediately). If no wheal forms or if it is less than 6 mm
in diameter, the test should be repeated about 2 inches from the
original site or on the opposite arm.
After a successful injection the needle is
removed without massaging or pressing the area. Sometimes there may
be minor bleeding which can be dabbed with a 2x2 gauze pad or cotton
ball till oozing of blood stops. There is no need to cover the site
with an adhesive bandage. The patient can get mild itching,
swelling, or irritation which is normal and usually goes away within
1 week. The patient is advised to avoid scratching the site, keeping
the site clean and dry and is also advised to return within 48 to 72
hours for reading of the test result.
Reading the Mantoux Tuberculin Skin Test
The site of injection on the forearm of the
patient is located. The fingernails of the reader should be short
and should not extend beyond the fingertip. The induration may not
always be visible, Therefore palpation of the area with fingertips
to determine induration at the injection site is needed. The area is
touched lightly with the pads of fingertips and the fingertips are
lightly swept in 2-inch diameters from the injection site in all
four directions to locate the edges of the induration.
Alternatively, one can use a zig-zag, feather-like touch to palpate
the area for margins of induration. Some times a margin of
induration may be confused with a margin of muscle on the forearm.
In such a case a repeat palpation with the patient’s arm raised to a
45-degree angle is done.
Once the outer edge of the induration is reached
rest one fingertip firmly against the induration margin on one side
before marking the margin. The fingertip should remain in contact
with the skin at all times. A ball point pen is used to mark the
margin lightly with a fine dot at the widest edge of the induration.
The procedure is reported on the opposite margin on the other side
of the induration. It is ensured that the induration was marked
correctly by a repeat palpation. If needed, the dots are altered on
repeat measurement.
Alternatively the induration may be detected by
the Ball point method. In this technique, a medium-point
ballpoint pen is used to draw a line starting 1 to 2 cm away from
the skin reaction and moving toward its center. When the pen reaches
the margin of the induration, an increased resistance to further
movement is felt and the pen is lifted. The procedure is repeated on
the opposite side of the skin reaction. The distance between the
ends of the opposing lines at the margins of the induration is
measured.
Usually a millimeter ruler is used to measure the
widest diameter of the induration perpendicular to the long axis of
the forearm. Only the margins of the induration are relevant for
measurement and the redness should not be measured. Reactions to the
tuberculin skin test at the injection site vary and if there is
blistering, the induration should be palpated gently as it may be
painful. Sometimes the margins are not equally clear all the way
around the induration but it is still necessary to mark the margins
on each side of the induration. For irregular margins of induration,
mark and measure the longest diameter across the forearm. The exact
measurement in millimeters of induration should be recorded and not
the interpretation of the results aspositive or negative along with
the date and time the test was read. If there is no induration, this
measurement should be recorded as 0 mm of induration. |
References
1. IAP Working Group. Treatment of childhood
tuberculosis: consensus statement of IAP working group. Indian Pediatr
1997; 34: 1093-1097.
2. IAP Working Group. Consensus statement of IAP
Working Group: status report on diagnosis of childhood tuberculosis.
Indian Pediatr 2004; 41: 146-155.
3. Management of Pediatric Tuberculosis under the
Revised National Tuberculosis Control Program (RNTCP). A joint statement
of the Central TB Division, Directorate General of Health Services,
Ministry of Health and Family Welfare, and experts from Indian Academy of
Pediatrics. Indian Pediatr 2004; 41: 901-905.
4. Chadha VK. Tuberculin test. Indian J Pediatr 2001;
68: 53-58.
5. Araujo Z, de Waard JH, de Larrea CF, Borges R,
Convit J. The effect of Bacille Calmette-Guérin vaccine on tuberculin
reactivity in indigenous children from communities with high prevalence of
tuberculosis. Vaccine 2008; 16: 26: 5575-5581.
6. Wang L, Turner MO, Elwood RK, Schulzer M, FitzGerald
JM. A meta-analysis of the effect of Bacille Calmette Guérin vaccination
on tuberculin skin test measurements. Thorax 2002; 57: 804-809.
7. Singla M, Sahai V, Sodhi S, Gupta RP. BCG skin
reaction in mantoux negative healthy children. BMC Infect Dis 2005; 5:
19-20.
8. Somu N, Swaminathan S, Paramasivan CN, Vijayasekaran
D, Chandrabhooshanam A, Vijayan VK, et al. Value of bronchoalveolar
lavage and gastric lavage in the diagnosis of pulmonary tuberculosis in
children. Tuber Lung Dis 1995; 76: 295-299.
9. Singh M, Moosa NV, Kumar L, Sharma M. Role of
gastric lavage and broncho-alveolar lavage in the bacteriological
diagnosis of childhood pulmonary tuberculosis. Indian Pediatr 2000; 37:
947-951.
10. Lobato MN, Loeffler AM, Furst K, Cole B, Hopewell
PC. Detection of Mycobacterium tuberculosis in gastric aspirates collected
from children: Hospitalization is not necessary. Pediatrics 1998; 102:
e40.
11. Zar HJ, Hanslo D, Apolles P, Swingler G, Hussey G.
Induced sputum versus gastric lavage for microbiological confirmation of
pulmonary tuberculosis in infants and young children: a prospective study.
Lancet 2005; 365: 130-34.
12. Ichhpujani RL, Agarwal SP, Chauhan LS. Diagnostic
needs and status of new diagnostic tools for tuberculosis. In:
Agarwal SP, Chauhan LS. Tuberculosis control in India. Directorate General
of Health Services, Ministry of Health and Family Welfare, Government of
India. New Delhi: 2005. p. 165-178.
13. Dheda K,Udwadia ZF, Hugget JF. Utility of
antigen-specific interferon gamma assay for the management of
tuberculosis. Curr Opin Pulm Med 2005; 11: 195-202.
14. Bianchi L, Galli L, Moriondo M, Veneruso G,
Becciolini L, Azzari C, et al. Interferon-gamma release assay
improves the diagnosis of tuberculosis in children. Pediatr Infect Dis J
2009; 28: 510-514.
15. Kampmann B, Whittaker E, Williams A, Walters S,
Gordon A, Martinez-Alier N, et al. Interferon- gamma release assays
do not identify more children with active TB than TST. Eur Respir J 2009;
33: 1374-1382.
16. Kabra SK, Lodha R, Seth V. Some current concepts on
childhood tuberculosis. Indian J Med Res 2004; 120: 387-397.
17. Verma K, Kapila K. Aspiration cytology for
diagnosis of tuberculosis—perspectives in India. Indian J Pediatr 2002; 69
Suppl 1: S39-43.
18. Sharma M, Agarwal S, Wadhwa N, Mishra K, Gadre DJ.
Spectrum of cytomorphology of tuberculous lymphadenitis and changes during
anti-tubercular treatment. Cytopathology 2007; 18: 180-183.
19. El Jahiri Y, Chellak S, Garcia C, Ceppa F, Burnat
P. The usefulness of adenosine deaminase determination in biological
fluids for tuberculosis diagnosis. Ann Biol Clin 2006: 64; 117-124.
20. Kaur A, Basha A, Ranjan M, Oommen A. Poor
diagnostic value of adenosine deaminase in pleural, peritoneal and
cerebrospinal fluids in tuberculosis. Indian J Med Res 1992; 95: 270-277.
21. Gambhir IS, Mehta M, Singh DS, Khanna HD.
Evaluation of CSF-adenosine deaminase activity in tubercular meningitis. J
Assoc Physicians India 1999; 47: 192-194.
22. Jain R, Sawhney S, Bhargava DK, Berry M. Diagnosis
of abdominal tuberculosis: sonographic findings in patients with early
disease. AJR 1995; 165: 1391-1395.
23. Mwandumba HC, Squire SB. Fully intermittent dosing
with drugs for treating tuberculosis in adults. Cochrane Database Syst
Rev. 2001;(4):CD000970.
24. Kabra SK, Lodha R. Seth V. Category based treatment
of tuberculosis in children. Indian Pediatr 2004; 41: 927-937.
25. Blomberg B, Spinaci S, Fourie B, Laing R. The
rationale for recommending fixed-dose combination tablets for treatment of
tuberculosis. Bull WHO 2001; 79: 61-68.
26. Kumar P. Journey of tuberculosis control movement
in India: national tuberculosis control program to revised national
tuberculosis control program. Indian J Tuberc 2005; S2: 63-71.
27. Kelkar-Khambate A, Klelmann K, Pawar S, Porter J,
Inamdar V, Datye A, et al. India’s Revised National Tuberculosis
Control Program: looking beyond detection and cure. Int J Tuberc Lung Dis
2008; 12: 87-92.
28. Chugh S. Paediatric tuberculosis and DOTS strategy
under RNTCP. J Indian Med Assoc 2008; 106: 799-802.
29. Enarson DA. The International Union Against
Tuberculosis and Lung Disease. Model National Tuberculosis Programmes.
Tuber Lung Dis 1995; 76: 95-99.
30. Comstock GW, Livesay VT, Woolpert SF. The prognosis
of a positive tuberculin reaction in childhood and adolescence. Am J
Epidemiol 1974; 99: 131-138.
31. Munoz FM, Starke JR. Tuberculosis in children.
In: Reichman LB, Hershfield ES, editors. Tuberculosis: A Comprehensive
International Approach: NewYork. Marcell Dekker Inc: 2000. p. 553-595.
|