|
|
|
Indian Pediatr 2010;47: 11-18 |
 |
Rational Use of Antibiotics for Pneumonia |
|
India Clinical Epidemiology Network (IndiaCLEN) Task Force on Pneumonia
Correspondence to: Narendera K Arora, Executive Director,
INCLENTRUST, 2nd Floor, F-1/5, Okhla Industrial Area, Phase I, New Delhi
110 020, India.
Email: [email protected]
|
|
Pneumonia affects 156 million children
under the age of five years every year across the globe, and is the
leading cause of mortality in this age group(1). More than two million
annual deaths are estimated to occur because of pneumonia in under-five
children, and almost all of these occur in the developing world(2).
Pneumonia kills more children in this age group than AIDS, malaria and
measles combined. India carries the largest burden of disease and
deaths because of pneumonia, accounting for 43 million cases and 0.4
million deaths(2). The median incidence of pneumonia in India is estimated
to be 0.37 episodes per child per year(2). Fortunately, most of the deaths
attributable to pneumonia can be prevented by relatively inexpensive and
feasible strategies. An increasing focus on the scaling up of
interventions for appropriate management of childhood pneumonia is crucial
to achieve the Millennium Development Goal (MDG) 4 of "reducing by
two-thirds, between 1990 and 2015, the under-five mortality rate."
Role of Antibiotics and Current Practices
Early diagnosis and appropriate case management by
rational use of antibiotics remains one of the most effective intervention
to reduce pneumonia-related mortality. As per the UNICEF/WHO report on
pneumonia "estimates suggest that if antibiotic treatment were universally
delivered to children with pneumonia, around 600,000 lives could be saved
each year"(3). Management issues for pneumonia also include early
diagnosis, availability of appropriate antibiotics, timely and appropriate
referral, monitoring and follow-up. These components are addressed in the
IMNCI/F- IMNCI/ARI control programs as are being implemented in India.
Access to universal availability of health services is also dealt within
the broad framework of the National Rural Health Mission (NRHM). What
requires strengthening is the rationalization of the use of antibiotics
for the treatment of pneumonia, and ensuring that it is made synchronous
with the actual field medical practices; so that the health care
providers, in the public as well as the private sector, implement the same
protocols.
Under-utilization and Misuse of Antibiotics
There are critical inequities in the access to
antibiotics and health services in most developing nations. There is a
clear dichotomy between the need and use of antibiotics; a large
proportion of children who need antibiotics for treatment of acute
respiratory infection (ARI) never reach any health facility and among
those who seek health care, irrational use of antibiotics is common.
Almost two-thirds of children who die at home are never taken to any
health facility before dying, and home treatments are given to majority of
them. Cumulative data from 27 countries suggested that only 19 per cent of
children with pneumonia received an antibiotic in the early 1990s(3). More
recent (2005-2006) National Family Health Survey-3 (NFHS-3) data from
India indicated that almost one-third (31%) of the children do not receive
any advice or treatment from a health facility or health provider for
their complaints of cough accompanied by short, rapid breathing that could
be suggestive of pneumonia(4). Further, only 12.5% children received
antibiotics for these complaints. The health seeking practices were poorer
in socioeconomically disadvantaged population, rural areas, and uneducated
mothers. The situation is similar in Bangladesh and Nepal, where less than
25% of under-five children with suspected pneumonia receive
antibiotics(5). The lack of any significant progress over the past 10
years across the developing world underscores the urgent need to act now
to ensure that children with pneumonia receive appropriate medical care.
The reasons for the under-utilization of antibiotics
are diverse. Caregivers often fail to recognize the importance of seeking
care in presence of difficult breathing or chest indrawing. Inadequate
resources, lack of political commitment, lack of coordination between
various health and government agencies, and fragmented implementation are
the other reasons for inadequate use of antibiotics in pneumonia. There is
an urgent need to increase the utilization of facilities by spreading
awareness about the importance of seeking care by children suffering from
symptoms and signs of possible pneumonia. Education programs also need to
emphasize that caregivers broadly understand the importance of the disease
and its treatment regimen, and are convinced of treatment efficacy.
On the other hand, inappropriate antibiotic use,
including prescribing antibiotics to children with simple colds or coughs,
is extremely common amongst those who seek health care. Antibiotics are
commonly prescribed for upper respiratory tract infections where they are
not required. New and expensive antibiotics are preferred, even in rural
areas, without knowledge about their safety and efficacy(6). The duration
of the use of antibiotics is often not regulated and the caregivers
frequently do not continue the drug for the prescribed period. These
practices lead to the emergence of drug resistant strains not only of the
causative bacteria but also for other bacteria present in the environment.
Antibiotic resistance amongst the common pneumonia causing bacteria (Streptococcus
pneumoniae and Haemophilus influenzae b) is being reported with
increasing frequency worldwide, including India(7,8). Unnecessary
antibiotic use also leads to wastage of healthcare resources, and
unnecessarily exposes patients to risk of adverse effects.
Under-utilization and misuse of antibiotics are thus
the two key features of the current scenario which need to be addressed.
Antibiotics – When, Which and How?
One needs to address the following 3 questions to
rationalize the use of antibiotics in pneumonia:
1. Decision on antibiotic: Whether antibiotic
is needed at all in a particular child with acute respiratory infection
(ARI)?
2. Choice of antibiotic: Which antibiotic to
use in which situation?
3. Appropriate regimen: How to prescribe i.e.
dose, frequency, route and duration of the antibiotic?
Assessing the Severity of Pneumonia
Children presenting with cough or difficult breathing
are diagnosed as pneumonia if they exhibit ‘fast breathing’. The
WHO algorithm for children presenting with cough or difficult breathing
proposes that ‘fast breathing’ is the most sensitive sign to identify
pneumonia in the community. The age related cut-offs of the respiratory
rate to define ‘fast breathing’ are:
³60/min
for age below two months;
³50/min
for age two months up to one year; and
³40/min
for children aged between one and five years. The respiratory rate should
be counted with a seconds’ watch for one complete minute.
Severe pneumonia is diagnosed if there is presence
of lower chest indrawing (definite inward motion of the lower chest wall
during quiet breathing). Children having danger signs such as inability to
feed, lethargy, central cyanosis, severe respiratory distress (head
nodding) or grunt are classified to be having very severe pneumonia.
It is mandatory that the health care providers are
trained in the recognition of fast breathing, lower chest indrawing, and
danger signs. The skills to identify signs, especially lower chest
indrawing, are awfully lacking in most health care providers who are not
properly trained. Community health workers have shown to be capable of
acquiring the skills needed to effectively manage ARI cases if training
emphasizes how to count the respiratory rate of children with tachypnea
and how to identify chest indrawing(9). In hospital or clinic settings,
additional clinical skills and investigations (wherever indicated), should
be used to diagnose the exact cause of respiratory distress (e.g.
pneumonia, bronchiolitis, asthma, croup, and non-respiratory causes); this
should dictate the further need for appropriate antibiotics.
Assessing the Need of Antibiotic
Most children reporting with cough, fever, and running
nose without presence of ‘fast breathing’ do not need antibiotics. Most
cases of bronchiolitis, asthma and croup do not require antibiotic
treatment.
A significant proportion of cases of pneumonia in
under-five children are likely to be of viral origin where antibiotics
will not be of any use. Studies from developing countries have documented
Respiratory Syncytial Virus (RSV) to be responsible for 15-40% of cases of
pneumonia in children admitted to hospital(2). Identifying cases who are
likely to have a viral rather than bacterial cause of pneumonia may lead
to decrease in antibiotic prescription. However, clinical differentiation
of viral and bacterial pneumonias is difficult, and occasionally they may
co-exist. Therefore, as of now, antibiotics need to be prescribed to all
children from the developing countries in the community setting who
are identified to be having pneumonia based on the clinical signs
described above.
Wheezing is a very common sign present in cases of non
severe and severe pneumonia in children. In most of the studies on
pneumonia and severe pneumonia, wheezing is associated in a large
proportion of children having lower chest indrawing or fast breathing. In
a recent trial evaluating the efficacy of oral drugs in treatment of
severe pneumonia, wheezing on auscultation was present in 62-82% of
children with lower chest indrawing despite excluding known asthmatics
from the study(10). Further, the signs of pneumonia and severe pneumonia
disappear after an initial trial (2-3 times) of inhaled bronchodilator
medications in almost half of these cases(11). History of two or more
previous episodes of respiratory distress also serves as a reliable tool
for diagnosing cases with wheezing(12). Therefore, it is logical to give a
trial of 2-3 doses of inhaled bronchodilators in children who have had two
or more previous episodes of respiratory distress, or those who are
identified to have wheezing in addition to ‘fast breathing’ or/and ‘lower
chest indrawing.’ Antibiotics may be withheld from cases where wheezing is
present, and signs of pneumonia or severe pneumonia disappear after an
initial course of inhaled bronchodilator drugs. However, only about
one-third of cases having wheezing and chest indrawing are known to have
an audible wheeze(12). The
feasibility of training health care providers in community to recognize
and manage wheezing should be evaluated. At first referral units, the
skills and equipments for recognizing and managing wheeze must be present.
Selection of Appropriate Antibiotic
The two most common bacterial pathogens causing
pneumonia in under-five children are: Streptococcus pneumoniae and
Haemophilus influenzae(2). A recent study suggests that
Staphylococcus is also an important cause contributing to 42% of
bacterial causes of very severe pneumonia in children(13). It is
imperative that antibiotic used for empirical treatment of pneumonia
should cover these organisms adequately.
Antibiotic of Choice for Pneumonia
Co-trimoxazole and amoxicillin are the two most
commonly recommended antibiotics for domiciliary treatment of pneumonia.
In a large hospital-based multicentric study of pneumococcal diseases in
children from India, co-trimoxazole resistance was found in 56% of the
isolates(7). The resistance to penicillin was rare (1.3%), and none of the
isolates was resistant to injectable third generation cephalosporins.
Amongst H. influenzae isolated from these centers, resistance was
common both to co-trimoxazole (45%) and ampicillin (38%)(8). Similarly,
data from other centers in India show increasing resistance in S.
pneumoniae isolates, with co-trimoxazole, the first choice of drug for
pneumonia till recently(14,15). Amoxicillin is another suitable
alternative which can be used in clinic setting as a first line drug for
non-severe pneumonia. Clear evidence regarding the superior efficacy of
amoxicillin over co-trimoxazole in field settings (using the WHO
definition of pneumonia) is lacking. A systematic review on the efficacy
of various antibiotics for pneumonia has documented a superior efficacy of
amoxicillin over co-trimoxazole(16). Co-trimoxazole was inferior in
efficacy to both amoxicillin (failure rates odds ratio (OR) 1.33; 95% CI
1.05 to 1.67) and procaine penicillin (cure rates OR 2.64; 95% CI 1.57 to
4.45). However, a recent multicentric trial from India reported that there
was no difference in effectiveness of oral co-trimoxazole or amoxicillin
in treating non-severe pneumonia in a field setting(17). Also, none of the
trials have documented any difference in mortality by using amoxicillin or
cotrimoxazole.
Thus, at the community level in India, there is no
compelling evidence to switch over from the current policy of using
cotrimoxazole (dose 5-7 mg/kg of trimethoprim+25-35mg/kg/day of
sulphamethoxa-zole for a duration of 5 days) as the first line antibiotic.
However, amoxicillin (dose 30-40 mg/kg/day for 3-5 days) is a suitable
alternative drug that can be used by the practicing physician in
outpatient setting. Amoxicillin also has the advantage of shortening the
duration of therapy to 3 days. A meta-analysis of three randomized
controlled trials from developing countries, including India, has
demonstrated the equivalent efficacy of a shorter course of amoxicillin in
comparison to the standard five-day regimen(18). The domiciliary
management of pneumonia is outlined in BOX.
|
BOX
Domiciliary Treatment of Pneumonia |
|
OR
Amoxicillin (30-40 mg/Kg/day)
in 2-3 divided doses for 3-5 days
- Advise mother to return immediately if the child develops chest
indrawing, is unable to feed or looks sick
- Follow-up after 2 days
* Check the child for general danger signs
* Assess the child for cough or difficult breathing
* Ask: Is the child breathing slower? Is there less fever? Is
the child eating better?
* If the answer to above questions is Yes, complete 5 days of
cotrimoxazole or 3-5 days of amoxicillin
* If condition is same, refer for second line antibiotic to FRU
* If chest indrawing or a general danger sign, refer urgently
for treatment of severe/very severe pneumonia
|
Oral cephalosporins (eg. cefixime) and quinolones
should not be used for treatment of childhood pneumonia. The mother should
be advised to return immediately if the child develops chest indrawing, is
unable to feed or looks sick. Additionally, all children started on first
line antibiotics need to be monitored for response (breathing slower, less
fever, eating better) after 48 hours. If there is no improvement or chest
indrawing or a general danger sign appears, the child should be referred
for assessment and second line antibiotics.
Antibiotics for Severe and Very Severe Pneumonia
The issues in the treatment of severe pneumonia are:
1. Whether these children require hospitalization?
2. What should be the first line antibiotic for
in-patient treatment?
There is a general consensus that all children aged
less than 2 months of age presenting with cough and fast breathing should
be diagnosed as having severe pneumonia and hospitalized in view of the
high mortality, treatment failure rates, and co-existence of other serious
morbidities such as sepsis and meningitis in this age group.
According to current guidelines, all children diagnosed
as severe pneumonia need to be hospitalized for detailed assessment,
injectable antibiotics, other supportive therapy and monitoring. Regarding
choice of injectable antibiotics for in-patient treatment of severe
community-acquired pneumonia; there is evidence that penicillins are
superior to chloramphenicol. In the systematic review evaluating all
antibiotics in pneumonia, penicillin in conjunction with genta-micin was
found to be better than chloramphenicol alone (re-hospitalization rates OR
1.61; 95% CI 1.02 to 2.55)(16). A recent multicentric trial (published
after the last significant update of the systematic review) also concluded
that injectable ampicillin plus gentamicin was superior to injectable
chloram-phenicol for the treatment of community acquired very severe
pneumonia in children aged 2-59 months in low resource settings(13). As
chloramphenicol is currently the recommended first choice drug for
in-patient treatment of very severe pneumonia, there is a need to update
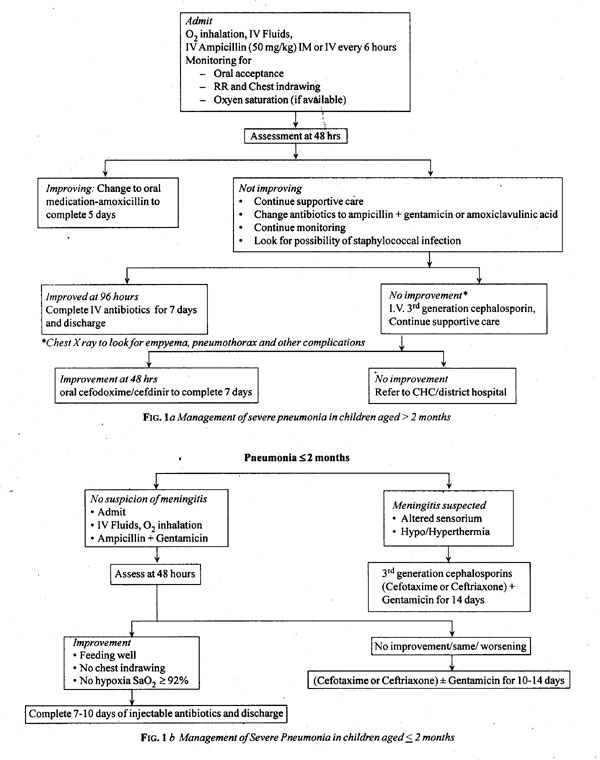
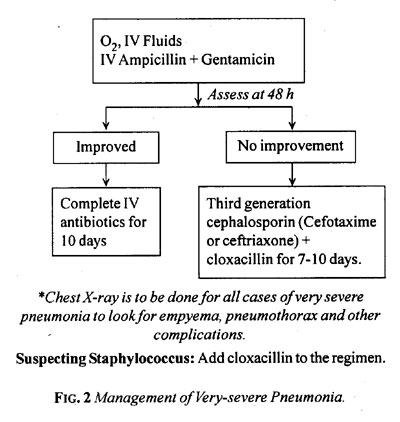
the current WHO guidelines for management of ARI. All children with severe
pneumonia should be initially treated with ampicillin (50 mg/kg IM/IV
every 6 hours). Gentamicin (7.5 mg/kg IM/IV once a day) should be added
for children aged less than two months, children having very severe
disease at the outset, or those who fail to respond at 48 hours. The
antibiotic should be changed to parenteral third generation
cephalos-porins such as cefotaxime and ceftriaxone, if still there is no
improvement after another 48 hours. Those with associated septicemia and
meningitis should receive intravenous cefotaxime or ceftriaxone as first
line drugs. Staphylococcal infection needs to be recognized based on
clinical and radiological features (skin boils, abscesses, rapid
progression/deterioration, pneumatoceles, empyema) and cloxacillin
(50mg/kg/dose, every 6 hourly) should be added. Antibiotics should be
continued for 5-7 days for severe pneumonia and 7-10 days for very severe
disease (Fig. 1 and Fig. 2). The
temptation of using new and fancy antibiotics promoted and pushed by
pharmaceutical companies should be resisted. In addition, all children
hospitalized with severe or very severe pneumonia should be monitored to
detect any complications or deterioration. If possible, a chest X-ray
should be obtained. The health provider should consider transferring the
patient to a higher facility in case of poor response or deterioration
despite second line therapy.
Regarding the use of oral amoxicillin for severe
pneumonia, a couple of studies have demonstrated that injectable
penicillin and oral amoxicillin are equivalent for severe pneumonia in
controlled settings(10,19). However, these results are not applicable to
all settings, especially where the risk of mortality is high such as those
with very severe disease (cyanosis, lethargy, recurrent vomiting, unable
to feed) or child having severe malnutrition. These subjects and those who
received prior antibiotic therapy, were invariably excluded by these
studies. Unless the evidence is more compelling, and is replicated to all
settings, it is not justified to change the current practice of
hospitalizing all children with severe pneumonia for detailed assessment,
injec-table antibiotics, oxygen and other supportive therapy and
monitoring. Oral treatment with amoxicillin can be given to selected
patients (who are aged more than three months old, look stable otherwise,
are not severely malnourished) where hospitalization is not possible
despite adequate counseling.
Epilogue
Pneumonia is a significant public health problem with
India carrying the largest burden of morbidity and mortality attributable
to pneumonia. A large proportion of these deaths can be prevented by
following the rational guidelines for management of acute respiratory
infections. Selection of the appropriate antibiotic in adequate dose and
correct duration is the need of the hour. There is a clear need of
strengthening health care practices related to pneumonia, including care
seeking and referral systems. Health care providers need to be trained in
recognizing the important signs that guide antibiotic therapy or referral.
Doctors working in all capacities need to be made aware of the standard
treatment protocols for pneumonia. Unnecessary and inappro-priate use of
antibiotics should be restricted to prevent antibiotic resistance.
Capacity building should also be done at referral units for other
supportive treatments such as bronchodilator and oxygen therapy.
Funding: IndiaCLEN through The United States
Agency for International Development (USAID) Maternal and Child Health
Sustainable Technical Assistance and Research (MCH-STAR) initiative.
Competing interests: USAID launched the MCH-STAR
initiative to help create a legacy of Indian institutions, such as
IndiaCLEN, that provide technical leadership in research, program
evaluation, policy analysis, responsive technical assistance and advocacy
of global standards in maternal, neonatal, child health and nutrition (MNCHN).
Disclaimer: The contents of this article are solely
the responsibility of the authors and do not necessarily represent the
official views of USAID or the United States Government.
Advisors: Vijay Kumar (WHO-SEARO), Rajesh Mehta
(WHO), Pavitra Mohan (UNICEF), Ashok Patwari (MCH-STAR), Sangeeta Saxena
(Govt. of India) and Rajiv Tandon (USAID).
Task Force Members: NKArora (IndiaCLEN, Delhi).
Shally Awasthi (KGMC, Lucknow), Piyush Gupta (UCMS, Delhi), SK Kabra (AIIMS,
Delhi), Joseph L Mathew (PGIMER, Chandigarh), K Nedunchelian (ICH&HC,
Chennai), AK Niswade (India-CLEN, Nagpur), Archana Patel (IGGMC, Nagpur),
Sneh Rewal (Social Scientist, Delhi), GR Sethi (MAMC, Delhi), Dheeraj Shah
(UCMS, Delhi) and Varinder Singh (LHMC, Delhi).
Writing Committee: Dheeraj Shah and Piyush
Gupta.
Convener: NK Arora (IndiaCLEN).
|
Key Messages |
|
• Fast breathing and lower chest indrawing are sensitive signs to
diagnose pneumonia and severe pneumonia, respectively in the
community.
• Most children with cough, runny nose and fever
without the presence of ‘fast breathing’ do not need antibiotics.
• Many children with lower chest indrawing caused
by bronchiolitis, asthma and croup also do not need antibodics.
• Oral co-trimoxazole (5 days) or amoxicillin
(3-5 days) should be used for domiciliary treatment of non-severe
pneumonia.
• All children with severe or very severe
pneumonia need hospitalization for injectable antibiotics, and
supportive therapy that may include oxygenation, intravenous fluids,
and monitoring.
|
References
1. Bryce J, Boschi-Pinto C, Shibuya K, Black RE; WHO
Child Health Epidemiology Reference Group. WHO estimates of the causes of
death in children. Lancet 2005; 365: 1147-1152.
2. Rudan I, Boschi-Pinto C, Biloglav Z, Mulholland K,
Campbell H. Epidemiology and etiology of childhood pneumonia. Bull World
Health Organ 2008; 86: 408-416.
3. UNICEF. Pneumonia: The Forgotten Killer of Children.
The United Nations Children’s Fund (UNICEF)/World Health Organization
(WHO), 2006. Available from: URL: http://www.unicef.org/publications/files/Pneumonia_The_Forgotten_Killer_of_Children.pdf.
Accessed August 30, 2009.
4. International Institute for Population Sciences (IIPS)
and Macro International. 2007. National Family Health Survey (NFHS-3),
2005–06: India: Volume I. Mumbai: IIPS. p. 223-266.
5. UNICEF: Progress for Children: A World Fit for
Children Statistical Review. United Nations Children’s Fund, 2007.
Available from: URL: http://www.unicef.org/progressforchildren/2007n6/files/Progress_for_Children_-_No._6.pdf.
6. Sharma R, Chopra VS, Kour G. Use of antibiotics for
respiratory illnesses in rural India. J Clin Diag Res 2009; 3: 1557-1561.
7. Invasive Bacterial Infection Surveillance (IBIS)
Group, International Clinical Epidemiology Network (INCLEN). Prospective
multicentre hospital surveillance of Streptococcus pneumoniae
disease in India. Lancet 1999; 353: 1216-1221.
8. Steinhoff MC, Thomas K, Lalitha MK, for the Invasive
Bacterial Infections Surveillance Group of the International Clinical
Epidemiology Network. Are Haemophilus influenzae infections a
significant problem in India? A prospective study and review. Clin Infect
Dis 2002; 34: 949-957.
9. Zeitz PS, Harrison LH, López M, Cornale G. Community
health worker competency in managing acute respiratory infections of
childhood in Bolivia. Bull Pan Am Health Organ 1993; 27: 109-119.
10. Hazir T, Fox LM, Nisar YB, Fox MP, Ashraf YP,
MacLeod WB, et al. New Outpatient Short-Course Home Oral Therapy
for Severe Pneumonia Study Group. Ambulatory short-course high-dose oral
amoxicillin for treatment of severe pneumonia in children: a randomised
equivalency trial. Lancet 2008; 371: 49-56.
11. Awasthi S, Agarwal G, Kabra SK, Singhi S, Kulkarni
M, More V, et al. Does 3-day course of oral amoxicillin benefit
children of non-severe pneumonia with wheeze: a multicentric randomised
controlled trial. PLoS One 2008; 3: e1991.
12. Sachdev HPS, Mahajan SC, Garg A. Improving
antibiotic and bronchodilator prescription in children presenting with
difficult breathing: experience from an urban hospital in India. Indian
Pediatr 2001; 38: 827-838.
13. Asghar R, Banajeh S, Egas J, Hibberd P, Iqbal I,
Katep-Bwalya M, et al. Multicentre randomized controlled trial of
chloramphenicol vs. ampicillin and gentamicin for the treatment of very
severe pneumonia among children aged 2 to 59 months in low resource
settings: a multicenter randomized trial (spear study). BMJ 2008; 336:
80-84.
14. Kanungo R, Rajalakshmi B. Serotype distribution and
antimicrobial resistance in Streptococcus pneumoniae causing invasive and
other infections in south India. Indian J Med Res 2001; 114: 127-132.
15. Blondeau JM, Tillotson GS. Antimicrobial
susceptibility patterns of respiratory pathogens—a global perspective.
Semin Respir Infect 2000; 15: 195-207.
16. Kabra SK, Lodha R, Pandey RM. Antibiotics for
community acquired pneumonia in children. Cochrane Database Syst Rev
2006; 3: CD004874.
17. Awasthi S, Agarwal G, Singh JV, Kabra SK, Pillai RM,
Singhi S, et al., for ICMR-IndiaClen Pneumonia Project Group.
Effectiveness of 3-day amoxicillin vs. 5-day co-trimoxazole in the
treatment of non-severe pneumonia in children aged 2-59 months of age: a
multi-centric open labeled trial. J Trop Pediatr 2008; 54: 382-389.
18. Haider BA, Saeed MA, Bhutta ZA. Short-course versus
long-course antibiotic therapy for non-severe community-acquired pneumonia
in children aged 2 months to 59 months. Cochrane Database Syst Rev 2008;
2: CD005976.
19. Addo-Yobo E, Chisaka N, Hassan M, Hibberd P, Lozano
JM, Jeena P, et al., for APPIS Group. Oral amoxicillin versus
injectable penicillin for severe pneumonia in children aged 3 to 59
months: a randomized multicentre equivalency study. Lancet 2004; 364:
1141–1148.
|
|
|
 |
|