|
|
|
Indian Pediatr 2020;57: 1147-1152 |
 |
Immunization During the COVID-19 Pandemic:
Recommendations From Indian Academy of Pediatrics Advisory
Committee on Vaccines and Immunization Practices
|
|
Srinivas G Kasi, 1
Shashi Kant Dhir,2 Sanjay
Verma,3 Harish Kumar Pemde,4
S Balasubramanian,5
Sunil Agarwalla,6 Abhay K
Shah,7 S Shivananda,8
Sanjay Marathe,9 Kripasindhu
Chatarjee,10 Sanjay
Srirampur,11 Srinivas
Kalyani,12 Bakul J Parekh,13
GV Basavaraja14 and Piyush
Gupta15
From 1Kasi Clinic, Bengaluru, Karnataka;
2Departments
of Pediatrics, Guru Gobind Singh Medical College, Faridkot, Punjab;
3Department of Pediatrics, Postgraduate Institute of Medical Education
and Research, Chandigarh; 4Lady Hardinge Medical College, New Delhi;
5Department of Pediatrics, Kanchi Kamakoti Childs Trust Hospital,
Chennai, Tamil Nadu; 6MKCG MCH, Berhampur, Odisha; 7Dr Abhay K Shah
Children Hospital, Ahmedabad, Gujarat; 8Fortis Hospital, Bengaluru,
Karnataka; 9Marathe Child Care Hospital, Nagpur, Maharashtra;
10Gouri
Devi Institute of Medical Science and Hospital, Durgapur, West Bengal;
11Aditya Super speciality Hospital, Hyderabad, Telangana;12Niloufer
Hospital, Osmania Medical College, Hyderabad; 13Bakul Parekh Hospital
for Children, Mumbai; 14IGICH, Bengaluru, Karnataka; and 15University
College of Medical Sciences, New Delhi; India, for the Advisory
Committee on Vaccines and Immunization Practices (ACVIP), 2020-21,
Indian Academy of Pediatrics, India.
Correspondence to: Dr Srinivas G Kasi, Convener,
ACVIP of IAP, Kasi Clinic, 2nd Cross, 3rd Block, Jayanagar, Bengaluru,
Karnataka, India.
Email: [email protected]
|
|
During the severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) pandemic, immunization practices of all age groups,
especially routine childhood vaccines, have been interrupted.
Immunization is considered an essential health activity, which
needs to be resumed as early as possible. This pandemic has
created several unique issues related to routine immunization of
individual children at clinics, which needs to be addressed. In
this communication, the Advisory Committee on Vaccines and
Immunization Practices (ACVIP) of Indian Academy of Pediatrics
addresses the common questions and issues related to SARS-CoV-2
and routine immunization services. This also includes the
recommendations for routine immunization of SARS-CoV-2 suspect
and positive children, and for the logistics to be followed for
immunization services.
Keywords: COVID-19, Guidelines, Missed
Vaccination, Routine immunization.
|
|
T
he coronavirus disease (COVID-19) pandemic has
negatively impacted every aspect of life. The economic sector has been
the most affected and preventive health services have been almost kept
on hold. Primary health care services, including immunization, have been
disrupted, putting women and children at risk for vaccine-preventable
diseases (VPDs), such as measles, rotavirus, and tetanus. Several
districts and blocks in India have had partial or complete lockdown
on-and-off, affecting movement of people. Fear of getting the infection,
social distancing norms and other infection prevention control practices
have adversely affected health seeking behavior and routine visits to
health care facilities. The primary focus of public health has been
diverted towards preparedness and containment of COVID-19 pandemic in
the country, and all other preventive health activities have been
relegated to the background.
The immunization services had to bear the brunt of
these unprecedented circumstances and various on-site and community
immunization services were severely affected. In April 2020, the health
management and information system data reported a decrease in the number
of routine immunization sessions relative to the previous year. The
number of fully immunized children also decreased over the same time
period. It is to be emphasized that any flare of VPDs will additionally
burden already stressed health care systems.
The severe acute respiratory infection 2 (SARS-CoV-2)
pandemic has created several unique issues related to vaccines and
immunization services. ACVIP has taken on itself to address the common
questions and issues related to COVID-19 and routine immunization
services in a question-answer format, with an objective to guide
pediatricians on these important issues.
Should children be vaccinated during the pandemic?
ACVIP recommends that all routine vaccinations be
administered as scheduled, even during the COVID-19 pandemic as it is an
essential health activity [1]. The benefits of immunizations far
outweigh the associated risks. The importance of continued immunization
activities is further emphasized by the observation that during the
2014-2015 Ebola outbreak, the increased number of deaths caused by
measles, malaria, HIV/AIDS and tuberculosis attributable to health
system failures, exceeded deaths from Ebola itself. In a benefit-risk
analysis of health benefits versus excess risk of SARS-CoV-2 infection,
in Africa, it was estimated that in a high-mortality scenario, for every
one excess COVID-19 death attributable to SARS-CoV-2 infections acquired
during routine vaccination clinic visits, 84 (95% CI 14-267) deaths in
children could be prevented by sustaining routine childhood
immunization. The advantages of sustained immunizations extended to
their siblings (<20 years) and to other family members also [2]. In the
private practice settings, the existing ACVIP Guidelines are to be
followed for routine immunization.
Is my child at an increased risk for getting infected
with SARS-CoV-2 by the hospital/clinic visit for immunization?
If SMS (social distancing, mask, sanitization) is
strictly followed, and the recommended COVID-19 related norms are
observed in the immunization session, the risk is minimal.
Is there any risk from immunizing a child during the
pandemic?
There is no documented risk of immunizing a well
child during the COVID-19 pandemic. COVID-19 is still an evolving
disease and hence we need to monitor strictly for any increased adverse
events following immunization (AEFI).
Is there a risk if we vaccinate a child during the
incubation period of COVID-19?
Currently there is no evidence that there is any risk
to the vaccinee if vaccination is done during the incubation period of
COVID-19. The efficacy and safety of the administered vaccines would be
the same.
Does vaccination increase a child’s risk of becoming
infected with SARS-CoV-2 or of developing COVID-19?
In general, vaccination against one disease does not
weaken the immune response to another disease. As of now, there is no
evidence that vaccination would increase the risk of a child becoming
infected with COVID-19 or affect the course of the disease in a child
who has been inadvertently vaccinated during the asymptomatic phase or
incubation period [3].
Is there a change in the existing immunization
schedule during the pandemic?
There is no information about the effect of COVID-19
on responses following immunization. ACVIP recommends that in private
practice settings, the existing ACVIP Guidelines are to be followed for
routine immunization [4]. There is currently no need for a change in the
immunization schedule.
How is area categorization being done by the
Government during the COVID-19 pandemic for providing immunization
services?
Based on World Health Organization (WHO) guidelines,
the Government of India (GOI) has categorized areas
(district/sub-division/municipal corporation/ward/any other appropriate
administrative unit) into Red and Orange zones with active COVID-19
cases, and Green zones with no active COVID-19 cases [5]. Areas where
COVID-19 cases are reported and surrounding areas with risk of COVID-19
spread are classified as Containment zone and Buffer zone respectively;
whereas areas outside the buffer zone are identified as Area beyond
buffer zone. The categorization of containment and buffer zones is a
dynamic process updated on a weekly basis or earlier. In alignment with
the area categorization, immunization services are classified into two
heads: Immunization in containment and buffer zones, and immunization in
areas beyond buffer zones and green zones.
How are immunization services to be conducted in
containment zones and buffer zones?
Traditionally, immunization services in India get
delivered through the following modes: Birth dose vaccination (at
delivery points), Health facility-based sessions (at fixed health
facilities), and Outreach sessions (as part of Urban/village health
sanitation and nutrition day services). The birth dose vaccination at
all health facilities should be provided to all the eligible babies. A
child reporting to the health care facility due to any reason should not
be denied immunization and every opportunity must be utilized for
vaccinating the beneficiaries. The health facility-based immunization
services should be provided only on demand to walk-in beneficiaries. The
outreach immunization sessions should not be undertaken in these areas.
However, the facility-based as well as outreach immunization activities
can be started after two weeks of delisting of the area as containment
or buffer zone, after being assessed for the COVID-19 risk by the
district authorities [6].
What are current recommendations for immunization
services in the area beyond buffer zone and green zone?
All areas beyond the buffer zone and in the green
zone need to follow similar guidelines. In these areas, the health
facility-based immunization services should be provided to all the
beneficiaries. The outreach (modified) immunization sessions can also be
undertaken at a predetermined site having adequate space and in a
modified way. Such a modified outreach session is to be planned for less
than 500 people, with a number of beneficiaries not more than 10-15 per
session. Less than five persons should be present at the session site
while maintaining a distance of 1 meter from each other. Organization of
such sessions will be at the discretion of the district administration,
with clear planning for social distancing and hand washing at session
site [6].
Should children from containment or buffer zones be
vaccinated if they report for vaccination in a facility outside those
areas?
Since the residents of the containment or buffer
zones are considered as suspects, they should not be encouraged to go
out of containment zones, as per government instructions. Active
immunization activities are not allowed in such areas. However, when any
child from such areas reaches the healthcare facilities, he/she should
be offered immunization as per the requirement of the child.
What logistics are required while setting up
immunization practices during COVID-19 times?
The logistics may be divided into preparation of the
space, personnel, vaccine, maintaining the waiting area and post
vaccination care (Box I).
|
Box I Logistics for Immunization Preparedness
During COVID-19
Preparation of the vaccination area
• Exclusive vaccination sessions are
recommended in separate vaccination rooms. If the same floor/
building is used for other patients, provision should be made
for separate entry and exit paths for the prospective vaccinees
to avoid mixing with the general patients.
• Adequate well-ventilated seating space
having one meter distancing from another person should be
available. The area should have exhaust fans for adequate air
circulation, and windows should be kept open.
• Sanitizers, soap and running water
should be made available in adequate amounts at the entry point
of the vaccination area.
• Vaccination staff, having any Flu like
symptoms, should not be allowed to vaccinate.
• It is essential that the doctor and
supporting staff utilize adequate PPE. A mask (N95 mask
preferably and three-layered surgical mask when N95 is not
available), gloves, and face shield along with scrupulous hand
hygiene are likely to protect from aerosol generation by a
crying child.
• New clean gloves (non-sterile) should be
donned before each vaccination.
• Hand hygiene with alcohol-based hand
sanitizers containing minimum 60% alcohol, for a minimum 20
seconds is to be practiced before and after each vaccination.
Gloved hand should also be sanitized.
• COVID-19 awareness material should be
displayed in the vaccination area.
• Continuous training should be imparted to
the health care personnel engaged in vaccination practices.
Vaccinee logistics
• The vaccinee should preferably be called by
appointment although no opportunity should be missed for
vaccination.
• Overcrowding should be avoided. Physical
distancing of 1 meter should be observed.
• Utilize every healthcare visit for
immunization, provided there are no precautions/
contraindications and the interval between vaccines are
maintained as per published guidelines.
• Minimum number of attendants preferably
single (maximum two) should only be allowed in the premises.
• The accompanying individuals should be
screened for fever and respiratory symptoms and if symptomatic,
they should not be allowed in the vaccination area and should be
advised to get examined at the health care services.
• Attendants who are more than 60 years of
age or have comorbid conditions should be requested not to
accompany the vaccinee.
• All caretakers and children, except infants
should wear a triple layer mask and provision should be made for
providing these at the entrance of the vaccination area.
• The accompanying persons should be made
aware of the social distancing, hand washing/sanitizing and
respiratory hygiene during the visit.
Waiting area
• The number of waiting persons both
before and after the vaccination should not be more than the
capacity of the area while maintaining the distance of 1 m
between two persons.
• Post vaccination, the vaccinee must be
observed for 15 minutes for development of any immediate AEFI.
• This waiting period should be used for
group counselling. Key preventive messages pertaining to
precautions during COVID period, strengthening of hand hygiene,
social distancing, breastfeeding, dietary advice, and danger
signs could be discussed during this period.
• The informative written material can also
be kept in the waiting areas.
Logistics post vaccination
• The furniture used should be thoroughly
cleaned with appropriate sanitizers.
• Proper sanitization of the anthropometry
equipment should be ensured immediately after each use.
• The biomedical waste generated should be
disposed of at source.
• Digital payment is to be encouraged.
|
What should be done if certain due vaccines are
missed?
This is a common situation in the COVID-19 pandemic.
The parents have to be reassured that the vaccination schedule can be
resumed without any need to restart the series. Multiple vaccines in one
sitting and using the minimum permitted interval between two doses of
the same inactivated vaccine can be practiced to complete the schedule
in the shortest possible time.
The vaccination services should be restarted as early
as possible. Missed vaccines have put the society at an increased risk
of VPDs. Multiple epidemics of measles occurred in 2015 in Guinea
because of the interrupted immunization during the Ebola outbreak [7].
The vaccine provider should track the cohort of children who have missed
the vaccine and immunize them, as soon as the vaccination becomes
feasible. Public awareness should also be done to sensitize them about
the catch-up vaccination. The parents should be reassured; that there is
a window period in which the vaccines could be given; and once given, it
would have similar efficacy in future. Following principles need to be
followed:
• The birth dose of hepatitis B vaccine should be
administered within 24 hours of birth and OPV, and BCG vaccines
should be given as early as possible after birth. If for any reason
this is not done, these vaccines should be administered at the first
contact with the healthcare facility.
• The primary vaccination series and the vaccines
for outbreak prone diseases should be prioritized for example DPT,
hepatitis B, Hib, OPV/IPV, rotavirus, PCV, influenza, varicella and
MR/MMR. Postponing these vaccines is to be avoided.
• The pneumococcal and influenza vaccine should
also be given to the vulnerable groups.
• The age specific recommendations of giving
vaccines e.g. for pneumococcal, meningococcal and rotavirus vaccine
should be followed.
• Multiple vaccines can be administered in the
same session without fear of any increased adverse effects.
• Typhoid conjugate vaccines may be clubbed with
the influenza vaccine at 6 months or MR/MMR at 9 months.
• Inactivated JE vaccines (where applicable) can
be administered at 1 year.
• We may use the shortest acceptable interval
between two doses of the same vaccine if the prospective vaccinee
reports to a health facility; and is unlikely to come for follow-up.
For inactivated primary vaccines this is 28 minus 4 days i.e. 24
days.
• The vaccination of healthcare personnel should
be up to date in their age appropriate vaccinations.
• When missed (because of the logistic issues of
transport etc.), hepatitis A vaccines and HPV vaccines may be
administered after the priority vaccines have been given.
• When missed (because of the logistic issues of
transport etc.), the booster dose(s) may be given at the next
earliest available opportunity.
• If a child is in a healthcare facility for any
reason, and eligible for immunization, this opportunity should be
utilized for administering eligible vaccines.
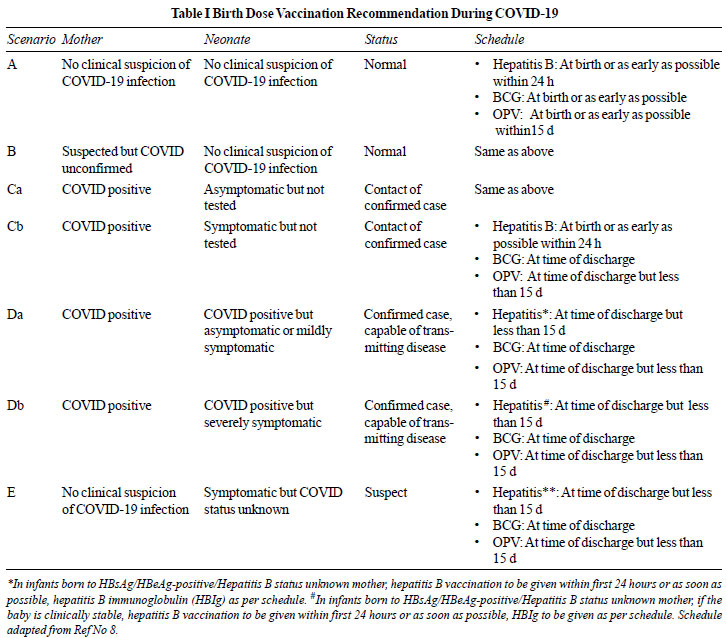
What schedule should be followed for vaccination at
birth?
The vaccination at birth depends upon the COVID-19
status of mother as well as the neonate, and the clinical condition of
the baby [8]. The recommendations are given in Table I.
What is to be done if the vaccinee is suspected or
diagnosed to have SARS-CoV-2 infection?
ACVIP recommends that if the prospective vaccinee has
been infected with COVID-19 or is under quarantine, the vaccination is
to be done only after the quarantine period is over and the clinical
condition of the baby is stable. If the child has any symptoms
suggestive of COVID-19 infection, vaccination is to be avoided till the
symptoms resolve. It is also emphasized that the presence of fever may
interfere in the differentiation between the disease progression and
vaccine induced adverse events. Therefore, it is best to wait for the
resolution of symptoms before vaccinating in COVID times. Standard
guidelines given in IAP guidebook on Immunization 2018-2019 (vaccination
in special situations) should be followed if children develop
‘Multisystem inflammatory syndrome’ during COVID infection and require
intravenous immunoglobulin or steroids [9]. It is not mandatory to
document a negative COVID test before vaccination.
Do Bacille-Calmette-Guérin (BCG) or MMR vaccines have
some role in controlling the ongoing COVID-19 pandemic?
Epidemiological studies have suggested a negative
association between national BCG vaccination policy and the prevalence
and mortality of COVID-19. Observational studies have also suggested
that countries with recent MMR campaigns or established MMR vaccinations
in their national programs have generally reported lower mortalities due
to COVID 19.
As of now, there is no evidence that BCG vaccine has
a protective role against occurrence of SARS-CoV-2 infection [10]. Based
on the current evidence, ACVIP does not recommend use of BCG or MMR
vaccine for the protection of individuals against COVID-19 infection
[10-12]. Various attributed potential nonspecific effects of the BCG
vaccine in preventing COVID-19 as of now remain a hypothesis, because of
multiple confounding factors [13]. Clinical trials are underway and the
recommendations would be updated once more evidence is available.
Disclaimer: These guidelines are meant for
practicing pediatricians in their office set up or hospital. These
guidelines are based on the available knowledge of COVID 19 as on date.
Any further guidance based on evolving scenarios will be issued
accordingly. Members are informed that these are only recommendations
and they should be taken in context with local advisories issued by
health authorities in the areas where the member provides medical
services.
Contributors: All authors conceived the idea,
reviewed the manuscript, analyzed and approved the manuscript.
Funding: None; Competing interests: None stated.
REFERENCES
1. Indian Academy of Pediatrics. Advisory Committee
on Vaccines and Immunization Practices (ACVIP). ACVIP Guidelines on
Immunization during COVID 19 Pandemic. Accessed September 25, 2020.
Available from: https://iapindia.org/pdf/1455-FINAL-ADVISORY-ACVIP-Guidelines-on-Immunisations-during-COVID-19-Pandemic-skd.pdf
2. Abbas K, Procter SR, van Zandvoort K, et al.
Routine childhood immunisation during the COVID-19 pandemic in Africa: A
benefit-risk analysis of health benefits versus excess risk of
SARS-CoV-2 infection. Lancet Glob Health. 2020;8:e1264-e72.
3. World Health Organization. Q&A on vaccination
during the COVID-19 pandemic. Accessed October 2, 2020. Available from:
https://www.euro.who.int/en/health-topics/disease-prevention/
vaccines-and-immunization/q-and-a-on-vaccination-during-the-COVID-19-pandemic.
4. Balasubramanian S, Shah A, Pemde HK, et al.
Indian Academy of Pediatrics (IAP) Advisory Committee on Vaccines and
Immunization Practices (ACVIP) Recommended Immunization Schedule
(2018-19) and Update on Immunization for Children Aged 0 Through 18
Years. Indian Pediatr. 2018;55:1066-74.
5. World Health Organization. Guiding principles for
immunization activities during the COVID-19 pandamic. Accessed September
25, 2020. Available from:
https://apps.who.int/iris/handle/10665/331590
6. Government of India. Ministry of Health and Family
Welfare. Immunization Services During and Post Covid-19 Outbreak.
Accessed September 25, 2020. Available from:
https://www.mohfw.gov.in/pdf/3Immunization Servicesduring
COVIDOutbreak Summary150520202. pdf
7. Suk JE, Jimenez AP, Kourouma M, Derrough T, Baldé
M, Honomou P. Post-Ebola measles outbreak in Lola, Guinea, January-June
2015. Emerg Infect Dis. 2016;22:1106-8.
8. Vaccination of Newborns in the Context of the
COVID-19 Pandemic, 19 May 2020 - PAHO/WHO. Pan American Health
Organization. Accessed October 2, 2020. Available from:
http://www.paho.org/en/documents/vaccination-newborns-context-COVID-19-pandemic-19-may-2020/
9. World Health Organization. Bacille Calmette-Guérin
(BCG) vaccination and COVID-19. Scientific Brief, 12 April 2020.
Accessed on October 9, 2020. Available from:
https://www.who.int/news-room/commentaries/detail/bacille-calmette-gu%C3%A9rin-(bcg)-vaccination-and-COVID-19
10. Indian Academy of Pediatrics (IAP). IAP Guidebook
on Immunization. Accessed October 9, 2020. Available from:
https://iapindia.org/iap-guidebook-on-immunization/
11. Vashishtha VM. Are BCG-induced non-specific
effects adequate to provide protection against COVID-19? [published
online ahead of print, 2020 Aug 07]. Hum Vaccin Immunother. 2020.
12. Deshpande S, Balaji S. MMR vaccine and COVID-19:
A myth or a low risk-high reward preventive measure? Indian Pediatr.
2020;57:773.
13. Dinleyici EC, Borrow R, Safadi MAP, van
Damme P, Munoz FM. Vaccines and routine immunization strategies during
the COVID-19 pandemic [published online ahead of print, 2020 Aug 26].
Hum Vaccin Immunother. 2020;1-8.
|
|
|
 |
|