|
|
|
Indian Pediatr 2021;58:745-748 |
 |
Diagnostic Reliability of Salivary
C-Reactive Protein as an Alternative Noninvasive Biomarker of
Neonatal Sepsis
|
|
Satish Datla, Srinivasan Kitchanan, Giridhar Sethuraman
From Department of Neonatology, Chettinad Hospital and Research
Institute, Chettinad Health City, Kelambakkam, Chengalpattu, Tamil Nadu,
India.
Correspondence to: Dr Giridhar Sethuraman, Department of Neonatology,
Chettinad Hospital and Research Institute, Chettinad Health City, Rajiv
Gandhi IT highway, Kelambakkam, Chengalpattu, Tamil Nadu 603 103.
Email: [email protected]
Received: July 06, 2020;
Initial review: August 18, 2020;
Accepted: December 31, 2020.
Published online: January 28, 2021;
PII: S097475591600284
|
Objective: To assess if salivary C-reactive
protein (CRP) can be detected in neonatal sepsis and correlate the
levels of salivary and serum CRP. Methods: This analytical
cross-sectional study included all neonates
£28 days
of life with suspected sepsis or with perinatal risk factors for sepsis.
Saliva was collected using an absorbent swab and analyzed by
enzyme-linked immunosorbent assay, along with serum CRP. Results:
Salivary CRP was detectable in 135 subjects (99%). An increase was seen
in median (IQR) levels from 0.25 (0.13,0.3) ng/mL in clinical sepsis
group to 0.6 (0.3,1.4) ng/mL in screen positive/blood culture negative
group, and to 1.98 (0.54, 2.95) ng/mL in blood culture positive group.
There was a moderate positive correlation between salivary and serum CRP
(r=0.63, P value 0.01). On receiver-operator
characteristics curve, the area under the curve of salivary CRP for
predicting serum CRP ³10
mg/L was 0.861 (95% CI, 0.78 to 0.94; P <0.001), with the optimal
salivary CRP cut-off being 0.6 ng/mL. Conclusion: Salivary CRP
could be used as an alternative biomarker of neonatal sepsis.
Keywords: Detection, Elisa, Inflammation,
Sensitivity.
|
|
B lood culture is
currently the gold standard for diagnosing neonatal sepsis, but
various biomarkers in serum are commonly used for rapid
supportive diagnosis. Among them, serum C-reactive protein (CRP)
is the most extensively studied biomarker in neonates and is
found in various body fluids like serum and saliva [1,2].
Considering the difficulty with phlebotomy in neonates and the
potential problems caused by blood sampling, alternative fluids
like saliva could serve as an attractive non-invasive option for
detection of CRP. Salivary diagnostic assays have now been well
described in various systemic and oral diseases in adults [3,4].
However, translation into neonatal clinical practice is limited
and is mostly restricted to cortisol assessment as a stress
marker in term and preterm infants [5,6]. The present study was
thus planned to investigate if CRP is detectable in saliva, and
whether levels correlate with serum CRP, among neonates with
sepsis.
METHODS
This was a cross-sectional study conducted in
the neonatal intensive care unit of a tertiary care hospital in
over a period of 18 months (September, 2015 to January, 2017).
The study was approved by the Institute’s research ethics
committee.
Neonates (aged
£28 days) of
any gestational age, with clinical suspicion of neonatal sepsis
or with perinatal risk factors of sepsis, were included in the
study, after informed written consent. Neonates with major
congenital malfor-mations, oral infections and oral ulcers were
excluded from the study. Demographic findings, including
intrapartum maternal fever, presence of preterm and or prolonged
rupture of membranes, chorio-amnionitis, gestational age, sex,
antibiotic treatment, clinical features, and day of presentation
were recorded. All subjects underwent a sepsis workup including
serum CRP, complete blood counts, and blood culture, in addition
to other investi-gations as deemed necessary by the treating
physician. Serum CRP was measured using immuno-turbidimetric
method using Roche Cobas C series analyzer (Roche Diagnostics).
Neonates were then further classified into three groups: Group I
– blood culture and sepsis-screen positive sepsis, Group II –
blood culture negative but sepsis screen positive (serum CRP
³10
mg/L and one additional parameter - neutropenia based on
standardized age based charts or immature: total neutrophil
ratios > 0.2), and Group III - only clinical features or
perinatal risk factors.
Saliva was collected within 4 hours of
collection of the serum sample. Antibiotics were started only
after collection of the salivary sample. SalivaBio Infant’s Swab
(SIS) (Salimetrics), was used for this purpose [7]. Salivary
sampling was done 60 minutes before or after a feed or any oral
procedure. The 90 mm SIS was placed between the cheeks and the
lower gums after turning the infants head to one side. The swab
was left in place for 3 minutes and then removed. The swab was
then visually inspected and if found dry, re-introduced for an
additional 3 minutes, up to a maximum of two attempts. Only
clear saturated swabs were used. The swab was then introduced,
saturated end first, into a plunger removed 5 mL syringe and
then the re-introduced plunger was used to squeeze out saliva
into cryovials. The process was repeated till 0.5 mL volume of
saliva was obtained. If sample collected was inadequate, then
the saliva collection was repeated with a longer oral stay
period for the SIS. In case of any infant discomfort (gag, brow
bulge, nasolabial furrow etc.) noticed during procedure, it was
immediately discontinued and resumed after signs abated. After
collection, labelled cryovials were frozen at –20 oC
within 4 hours of collection. The saliva collection was done by
the treating team members, after structured training. Each
member was supervised during initial few sample collections, to
ensure standardization.
On the day of the analysis, saliva samples
were thawed and centrifuged. Samples were brought to room
temperature before the dilutions. The Salimetrics salivary CRP
enzyme immunoassay kit (Salimetrics), an indirect sandwich ELISA
kit, was used as per the manufacturer’s recommended protocol
[8]. All samples were assayed in duplicate, and the average of
the duplicates was used in the statistical analyses. Intra and
inter-assay coefficients of variation were less than 10% and
15%, respectively. The salivary CRP was estimated in the entire
cohort and also in the three groups of infants.
Assuming that salivary CRP has a minimum
expected sensitivity and specificity of 75% to predict serum CRP
³10
mg/L, and an expected prevalence of neonatal sepsis of 40% (as
per departmental statistics for the previous year), with an
absolute precision of 10% and 90% confidence level, the required
sample size was 128 subjects (STATA IC, ver. 13). To account for
5% non-response rate, a total of 136 subjects were included in
the final study.
Statistical analysis: Considering the
skewed distri-bution of serum and salivary CRP levels,
correlation was assessed using Spearman rank order (Spearman’s
rho) coefficient. The utility of salivary CRP in predicting
elevated seum CRP ( ³10
mg/L) was assessed by receiver operating characteristic (ROC)
curve analysis and an appropriate salivary CRP cut off value was
calculated. The sensitivity, specificity, predictive values and
likelihood ratios of salivary CRP at the derived cut-off were
calculated for predicting serum CRP
³10 mg/L and
positive blood culture. P value <0.05 was considered
statistically significant. IBM SPSS version 22 (SPSS Inc.) was
used for statistical analyses.
RESULTS
A total of 182 neonates satisfied the
inclusion criteria. 32 neonates were excluded because of refusal
of consent or already receiving antibiotics. Adequate salivary
sample could not be obtained in 9 neonates and in 5, the samples
were not analyzed because of contamination. Thus,136 neonates
were included in the final analysis. The median (IQR)
birthweight was 1.98 (1.34,2.57) kg and gestational age was 34.5
(32,37) weeks. Early onset sepsis ( £3
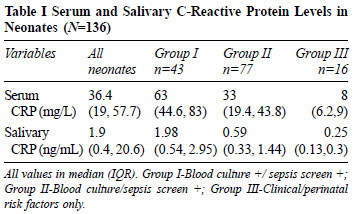
days) was seen in 88 (64.7%) of the population. Salivary CRP was
detectable in 135 (99%) neonates and the levels increased
significantly from Group III to Group I neonates (Table I).
There was a moderate and statistically
significant positive correlation between salivary and serum CRP
values in the entire study population (r=0.63; P
=0.01) and in Group I (r=0.63; P =0.01) and Group
II neonates (r =0.5; P =0.01).
The area under the ROC curve for salivary CRP
to predict serum CRP ³10
mg/L was 0.861 (95% CI, 0.78 - 0.94, P<0.01), indicating good
predictive validity. Based on the co-ordinates of the ROC
curve, the cut-off of 0.6 ng/mL was chosen as the optimal
salivary CRP cut-off value for predicting serum CRP
³10 mg/L.
Salivary CRP ³0.6
ng/mL had a 77% sensitivity, 94% specificity, 99% positive
predictive value and 35% negative predictive value, for
predicting a serum CRP level of
³10 mg/L; and
75% sensitivity, 58% specificity, 44% positive predictive value
and 85% negative predictive value, for predicting a positive
blood culture.
DISCUSSION
We found that CRP can be detected in saliva
of neonates with sepsis, and increases significantly in those
with elevated serum CRP, compared to those with only suspicion
of sepsis but with non-elevated biomarkers (group 3). We also
found a moderate positive correlation of salivary CRP with serum
CRP in these neonates.
There is limited previous data on the
diagnostic utility of salivary CRP in neonatal inflammatory
conditions and its comparison with serum CRP. Iyengar, et al.
[9] showed that salivary CRP was detected in 97% of neonates
with inflammatory states, especially post-operative. The levels
also moderately correlated with serum CRP levels. Omran, et al.
[10] found a significant difference between salivary CRP values
in septic and healthy infants, with a moderate correlation
between salivary and serum CRP. The levels of salivary CRP in
our study was different from previous reports [9,10]. Some of
the observed differences may be explained by variation in
population characteristics. Our study population included both
preterm and term infants, whereas others had included mainly
post-operative neonates (only 12 with sepsis) [9], or had
recruited only term infants [10]. Another reason could be the
use of different assay methods and pre-processing techniques. We
used a highly sensitive salivary CRP assay [8] and a validated
saliva collection method [7]. A significant positive correlation
between salivary and serum CRP was also seen by these authors
[9,10]. Both adult and pediatric population studies have shown a
good correlation between salivary CRP and serum CRP levels, in a
variety of clinical conditions [11]. Although positive
correlation is reassuring, this is insufficient to advocate
salivary CRP as a replacement for serum CRP, considering the
population characteristics of our study. More studies in
neonates, across a variety of inflammatory conditions, showing
similar correlation, are required, in order to change practice.
Proper collection of saliva is important for
ensuring accuracy using salivary diagnostics and is even more
challenging in neonates. Previous researchers [9,10] had used an
improvised 1 mL syringe attached to low-wall suction, to collect
saliva, a method previously described by Dietz, et al. [12]. We
found this method difficult to use in very low birth weight
infants as it frequently resulted in blood mixed saliva, related
to mucosal trauma. Hence, we used the SIS for saliva collection,
which has been previously validated for salivary analytes [7].
We found that by using a proper technique, maximal
uncontami-nated saliva recovery was possible with less patient
discomfort.
We found that infants with negative sepsis
screen/ blood culture, with only clinical signs or perinatal
risk factors of sepsis also had detectable salivary CRP levels
(range of 0.11-1.39 ng/mL). This possibly indicates a normal
physiological increase in salivary CRP levels to detectable
range, in the initial days of life, similar to serum CRP. To our
knowledge, there is no previous published normative data on
salivary CRP levels in healthy infants. Extrapolation from adult
studies could also be fallacious due to the differing population
characteristics, and variation in salivary CRP levels among
studies, with reported levels ranging from 0.03-24.2 ng/mL
[13,14]. Further large studies are necessary to identify
normative ranges of salivary CRP in healthy neonates of
different gestational ages. The performance of salivary CRP
during serial analysis, and also against the ‘gold standard’
blood culture, was not done in our study. Also, we did not
normalize salivary CRP concentration for salivary flow rate and
protein concentration, because previous data on the utility of
this and the ideal normalization method in neonates was lacking.
These areas should also be addressed in future trials.
Our study suggests that salivary CRP could be
used as an alternative biomarker to serum CRP in neonatal
sepsis. However, widespread usage in neonates will require
further research into saliva collection methodo-logy,
standardization of assay procedure, establishing normative
values and determining cost effectiveness. As of now, it appears
a very useful diagnostic surrogate for blood sampling.
Ethics clearance: Chettinad Academy of
Research and Education Institutional Human Ethics Committee; No.
121/25/09/2015, dated September 04, 2015.
Contributors: SD: conducted the study
experiments, performed data collection and analysis; and wrote
the final manuscript; SK: contributed to statistical analysis
and critical evaluation of the final manuscript; GS: conceived
and supervised the study, verified the statistical analysis,
contributed to the critical evaluation of the final manuscript
approved the final version of the manuscript.
Funding: None; Competing interests:
None stated.
|
WHAT THIS STUDY ADDS?
• Salivary CRP could be used as an alternative
biomarker for neonatal sepsis as it increases in septic
neonates and positively correlates with serum CRP.
|
REFERENCES
1. Hedegaard SS, Wisborg K, Hvas AM.
Diagnostic utility of biomarkers for neonatal sepsis-A
systematic review. Infect Dis. 2015;47:117-24.
2. Benitz WE, Han MY, Madan A, Ramachandra P.
Serial serum C-reactive protein levels in the diagnosis of
neonatal infection. Pediatrics. 1998;102:E41.
3. Kaczor-Urbanowicz KE, Martin Carreras-Presas
C, Aro K, Tu M, Garcia-Godoy F, Wong DT. Saliva diagnostics -
Current views and directions. Exp Biol Med (Maywood).
2017;242:459-72.
4. Cuevas-Córdoba B, Santiago-García J.
Saliva: A fluid of study for OMICS. OMICS. 2014;18:87-97.
5. Francis SJ, Walker RF, Riad-Fahmy D,
Hughes D, Murphy JF, Gray OP Assessment of adrenocortical
activity in term newborn infants using salivary cortisol
determinations. J Pediatr. 1987;111:129-33.
6. Mörelius E, He HG, Shorey S. Salivary
cortisol reactivity in preterm infants in neonatal intensive
care: An integrative review. Int J Environ Res Public Health.
2016;13:337.
7. Salimetrics. Collection Methods: SalivaBio
Infant’s Swab (SIS). Accessed July 4, 2020. Available from:
https://salimetrics.com/wp-content/uploads/2018/02/
infant-swab-saliva-collection-instructions.pdf
8. Salimetrics. Salivary Elisa Kit
(generation II). Accessed July 4, 2020. Available from:
https://salimetrics.com/wp-content/uploads/2017/05/c-reactive-protein-saliva-elisa-kit.pdf
9. Iyengar A, Paulus JK, Gerlanc DJ, Maron
JL. Detection and potential utility of C-reactive protein in
saliva of neonates. Front Pediatr. 2014;2:131.
10. Omran A, Maaroof A, Saleh MH, Abdelwahab
A. Salivary C-reactive protein, mean platelet volume and
neutrophil lymphocyte ratio as diagnostic markers for neonatal
sepsis. J Pediatr (Rio J). 2018;94:82-87.
11. Pay JB, Shaw AM. Towards salivary
C-reactive protein as a viable biomarker of systemic
inflammation. Clin Biochem. 2019;68:1-8.
12. Dietz JA, Johnson KL, Wick HC, Bianchi
DW, Maron JL, Optimal techniques for mRNA extraction from
neonatal salivary supernatant. Neonatology. 2012;101:55-60.
13. Mohamed R, Campbell JL, Cooper-White J,
Dimeski G, Punyadeera C. The impact of saliva collection and
processing methods on CRP, IgE, and myoglobin immunoassays. Clin
Transl Med. 2012;1:19.
14. Ouellet-Morin I, Danese A, Williams B,
Arseneault L. Validation of a high-sensitivity assay for
C-reactive protein in human saliva. Brain Behav Immun.
2011;25:640-6.
|
|
|
 |
|