|
|
|
Indian Pediatr 2014;51:
613-619 |
 |
INCLEN Diagnostic Tool
for Neuromotor Impairments (INDT-NMI) for Primary Care
Physician: Development and Validation
|
|
Sheffali Gulati, Satinder Aneja, Monica Juneja, Sharmila Mukherjee,
Vaishali Deshmukh, Donald Silberberg, Vinod K Bhutani, Jennifer M Pinto,
Maureen Durkin, Poma Tudu, Ravindra M Pandey, MKC Nair,
Narendra K Arora and INCLEN Study Group*
From the INCLEN TRUST International, New Delhi, India
Correspondence to: Dr Narendra K Arora,
Executive Director, The INCLEN Trust International, F1/5, Okhla
Industrial Area Phase 1, New Delhi, India.
Email: [email protected]
Received: April 03, 2013;
Initial review: July 05, 2013;
Accepted: April 22, 2014.
*INCLEN Study Group: Core Group: Alok
Thakkar, Arun Singh, Devendra Mishra, Gautam Bir Singh, Manju Mehta,
Manoja K Das, Nandita Babu, Paul S S Russell, Praveen Suman, Rajesh
Sagar, Ramesh Konanki, Rohit Saxena, Savita Sapra, Sunanda K Reddy,
Tanuj Dada. Extended Group: AK Niswade, Archisman Mohapatra, Arti
Maria, Atul Prasad, BC Das, Bhadresh Vyas, GVS Murthy, Gourie M Devi,
Harikumaran Nair, JC Gupta, KK Handa, Leena Sumaraj, Madhuri Kulkarni,
Muneer Masoodi, Poonam Natrajan, Rashmi Kumar, Rashna Dass, Rema Devi,
Sandeep Bavdekar, Santosh Mohanty, Saradha Suresh, Shobha Sharma,
Sujatha S Thyagu, Sunil Karande, TD Sharma, Vinod Aggarwal, Zia
Chaudhuri.
|
Objectives: To develop and validate a diagnostic tool for use by
primary care physicians for diagnosing neuro-motor impairment among 2-9
year old children in primary care settings.
Study design: Modified Delphi technique involving
national (n=49) and international (n=6) experts was used
for development of INDT-NMI. The tool was then validated through a cross
sectional study.
Setting: Neurology specialty clinics of three
tertiary care pediatric centers in New Delhi, India.
Participants: 454 children aged 2-9 years [mean
(SD) age: 60.4 (23.7) mo], selected through systematic random sampling,
underwent assessment for identification and classification of neuromotor
impairments (NMI).
Intervention: All study subjects were first
administered INDT-NMI (candidate test) by a trained physician followed
by expert assessment for NMI and other neurodevelopment disorders (NDD)
by team of two pediatric neurologists (Gold standard).
Results: According to expert evaluation, 171
(37.8%) children had neuromotor impairments. There were four categories
of subjects: NMI alone (n=66); NMI+other NDDs (n=105);
Other NDDs without NMI (n=225) and ‘Normal’ group (n=58).
Using expert evaluation as gold standard, overall sensitivity of the
INDT-NMI was 75.4% and specificity was 86.8%. INDT-NMI helped graduate
physicians to correctly classify 86.6% (112/129) children with NMI into
different types (cerebral palsy, neuromotor diseases and other NMI).
Graduate physicians assigned 40 children (8.8%) as ‘indeterminate’, 38
(95%) of whom had either NDD and/or NMI and thus merited referral.
Misclassification of NMI occurred in those with mild changes in muscle
tone, dystonia, or ataxia and associated NDDs.
Conclusion: Graduate primary care physicians with
a structured short training can administer the new tool and diagnose NMI
in 2-9 year old children with high validity. INDT-NMI requires further
evaluation in actual primary care settings.
Keywords: Cerebral palsy, Disability, Diagnosis, Neuromuscular
disorders, Resource constrained environments.
|
|
P
rimary care physicians frequently encounter
children with neuromotor impairments who have difficulties of movement,
posture and coordination in their day-to-day life. Neuromotor
impairments (NMI) include a continuum of disorders caused by a wide
variety of non-progressive and progressive conditions that affect
body functions, activities, and quality of life. Cerebral palsy (CP)
constitutes the bulk of NMI; progressive acquired or inherited
neuromuscular disorders (NMD), and other NMI (not satisfying the
definition of either CP or NMD) have to be considered in differential
diagnoses as the approach to management and outcome varies significantly
[1-3].
Pediatric neurologists, developmental pediatricians
and therapists with expertise in diagnosis and management must be able
to obtain a relevant history and perform focused musculoskeletal,
neurologic and functional physical examinations to diagnose NMI [4]. The
availability and access to such expertise in resource- constrained
environments like India and other developing countries is severely
restricted and thus significantly increases the gaps in identification,
and delivery of specific therapeutic and rehabilitative services for NMI
[5,6]. Availability of a diagnostic tool for use by primary care
physicians will considerably increase access to specific care and
rehabilitation of children with NMI. Currently no validated tool is
available for diagnosing NMI among 2-9 year old children in primary care
settings. The demand for such a tool is further enhanced in the light of
recently launched Rastriya Bal Swasthya Karyakram (RBSK) wherein
diagnosis and management of neuro-developmental disorders within primary
care settings is a core element of the program services [7].
To fill this gap, the INCLEN study group developed
and validated a diagnostic tool for NMI (INCLEN Diagnostic Tool for
Neuromotor Impairments: INDT-NMI) that employs standardized and uniform
diagnostic criteria for use in 2-9 year-old children. The tool is meant
to be used by graduate physicians after a structured short training in
primary care settings.
Methods
Study design: Modified Delphi process for
developing the tool, and diagnostic test evaluation by cross-sectional
study design
The study was part of the INCLEN program to estimate
the burden of Neuro-developmental Disorders (NDDs) in 2-9 year-old
children at five sites across the country. As part of the larger study,
specific diagnostic tools (for autism spectrum disorders [8], attention
deficit hyper-activity disorder [9], epilepsy [10] and NMI) were
developed and validated for use by different levels of health personnel.
INDT-NMI is to be applied by primary care physicians for the diagnosis
of NMI. The evaluation of INDT-NMI was conducted on 2-9 year-old
children attending the pediatric neurology outpatient clinic of three
public sector tertiary-care referral centers [All India Institute of
Medical Sciences (AIIMS), Lady Hardinge Medical College (LHMC), and
Maulana Azad Medical College (MAMC)] in New Delhi, India. The pediatric
neurology specialty clinics in these hospitals attract a mix of complex
neurology problems referred for diagnosis and management. Children of
either gender in the age group 2-9 years coming for the first time in
the pediatric neurology clinics of these hospitals were eligible for
inclusion in the study. Children were excluded from the study if they
had poor general condition (e.g. respiratory distress requiring
supplemental oxygen, peripheral circulatory collapse, altered sensorium,
or requiring care in intensive care), were not accompanied by primary
caregiver, and if care provider refused consent. The tool development
and validation exercise was conducted from June 2008 to April 2010.
Ethical approval was obtained from INCLEN review board and ethics
committees of all the sites.
Development of diagnostic tool: Candidate test:
As the first step, a consensus clinical criteria (CCC) for diagnosing
NMI was developed by group of national (n=49) and international (n=6)
experts consisting of pediatricians, developmental pediatricians, child
psy-chiatrists, pediatric neurologists, pediatric oto-rhino-laryngologists,
community physicians, clinical psycho-logists, special educators,
specialist nurses, speech therapists, occupational therapists, and
social scientists, for diagnosing NMI through a series of three 2-day
work-shops and web-based discussion using modified Delphi method. The
CCC was then converted in to a diagnostic tool, INDT-NMI, for use by
graduate physicians in primary care settings.
INDT-NMI is based on the definitions and
classification proposed for cerebral palsy [11] along with questions to
identify neuromuscular disorders (NMD) and other NMI that do not fit in
to definition of either of these conditions (for practical reasons and
simplification of the diagnostic process at primary level). The INDT-NMI
thus developed comprises of three sections. Section-I (Triage questions)
consists of four questions to elicit information from the
parents/primary caregiver of the child regarding attainment of selected
motor developmental milestones. Section-II (Observations):
Physician makes three observations for assessing hand function, gait and
muscle weakness. Section-III consists of six questions,
and the operator (graduate physician) does the neurological examination
necessary for confirmation of NMI. Thus final diagnosis of NMI is
derived through an algorithm based on interpretation of three sections (i.e.
13 questions/items) and information on age at onset of symptoms, course
of the illness and obvious clinical evidence of involvement of spinal
cord (i.e. pilonidal sinus, tuft of hair). This tool requires
approximately 20-25 minutes for assessing each child. Tool includes
specific neurologic examination with interpretation but examination of
cranial nerves and sensory neurologic system examination is not included
in the tool as these are not directly relevant for making diagnosis of
NMI. The final diagnosis informs whether the case has cerebral palsy
(CP), neuromuscular disorders (NMD), Other NMI (that does not fit in to
either CP or NMD), no NMI or an indeterminate clinical condition. The
tool (Web Appendix I) was prepared in English, translated
into Hindi and back translated to English before the study was
undertaken.
At each of the three institutions, diagnosis of NMI
was established by consensus of two pediatric neurologists with
expertise in diagnosis and management of children with NMI and other
NDDs. The clinical assessment included detailed history and physical
examination with access to radiological and other relevant
investigations whenever available.
Systematic random sampling of the children attending
pediatric neurology clinics was followed for enrolment of study
subjects. Daily, the principal investigator provided two
computer-generated random numbers to the study coordinator in a sealed
envelope. First random number (between 1 and 9) gave the serial number
of first child to be recruited in the clinic and second random number
was the nth number of patient (between 5 and 15 and represented interval
between subjects as they came up in neurology specialty OPD at central
registration) who was identified for the detailed evaluation. The
identified subjects so enrolled were assessed for eligibility by site
coordinator, and enrolled after obtaining written, informed consent
until the final sample size was achieved. If consent or inclusion
criterion was not achieved or if the child was not a first timer
attendee, (n+1) th child was enrolled. Subjects were recruited
till the desired sample size was obtained in each category.
At each study site, a team of pediatric neurologists
(at least two per site) with at least three years of experience in the
diagnosis and management of children with NMI and other NDDs, one study
coordinator and two graduate physicians (MBBS) undertook the study.
Subjects were first administered the INDT-NMI (candidate test) by a
graduate doctor (MBBS qualified) and later evaluated by the expert team
of pediatric neurologists (gold standard). The findings of
the graduate physician and expert group were separately placed in opaque
envelopes, sealed and handed over to the coordinator. Evaluators of one
category were blinded to the diagnosis of the other group. The children
were given prescription and instructions for additional investigations
as required and follow-up by the expert group. After initial assessment,
the subjects were not allowed to interact with the graduate physician to
avoid contamination and influence on the assessment of subsequently
recruited subjects.
A standardized training manual with detailed
instructions for administration of the tool was developed. Graduate
physicians at each center administered the questionnaire verbatim,
questioning the parents in the language they could understand (English
or Hindi). These individuals were trained during a one-day hands-on
structured workshop that included eight hours of didactic teaching and
simulated administration of the tool in five cases of neuro-motor
impairment. The training also involved interview skills and techniques
of neurological examination of children.
Sample size: We expected four categories
of subjects in whom INDT-NMI was to be evaluated: NMI alone, NMI along
with other NDD, Other NDDs without NMI and children without NMI or other
NDDs (Normal). Assuming sensitivity and specificity of INDT-NMI to be
85% with ±10% precision at 95% confidence level, sample size was
calculated to be 50 subjects in each category of patients. To account
for 10% drop-outs, it was decided to enroll at least 55 children in each
category. The sample size was calculated using Epi info software [12].
Statistical analysis: The data were
analyzed using STATA 10 software. The psychometric properties of
INDT-NMI were calculated against the assessment done by team of
pediatric neurologists (Gold standard).
Results
A total of 454 children (mean ± SD age: 60.4 ± 23.7)
were enrolled from three centers: AIIMS 354; MAMC 46; and LHMC 54. The
subjects included 308 (68%) boys and 146 (32%) girls; 40.3% (n=183)
were 24-48 month old, 43.2% (n=196) were aged between 49-84
months, and 16.5% (n=75) belonged to 85-108 month category.
According to expert evaluation, 66 children had NMI alone (CP=39; NMD
20; other NMI 7), 105 had NMI with other NDDs (CP 95; NMD 3; other NMI
7) 225 with Other NDDs without NMI, and 58 subjects were normal (without
NMI or any other NDD). Thus, 171 (38%) children had NMI (CP 134; NMD 23
and other NMI 14) and remaining 283 (62.3%) were without NMI. Out of 134
children with CP, 95 (70.9%) had one or more co-morbidities like
epilepsy, global developmental delay and intellectual disability.
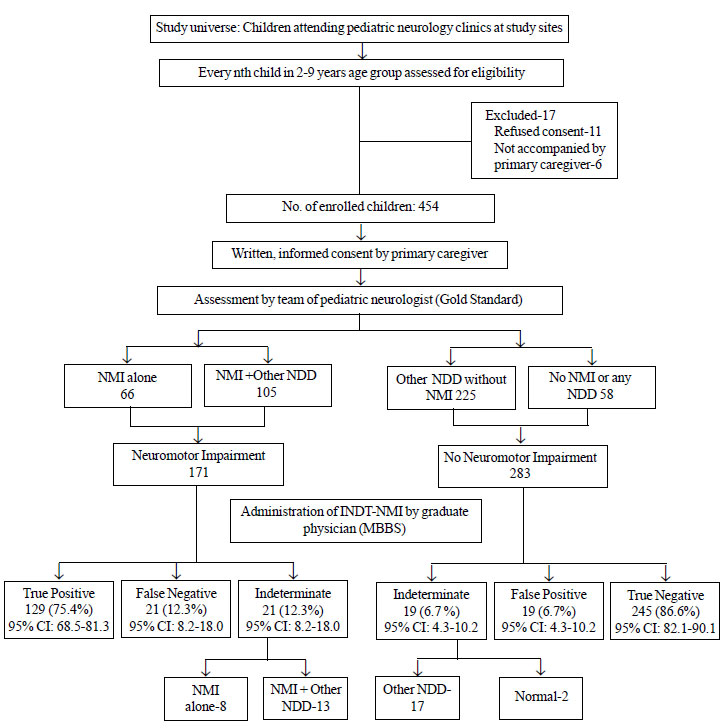
Using INDT-NMI, graduate physicians were able to
assign NMI (yes/no) label to 414 subjects: remaining 40 out of 454
(8.8%) subjects were categorized as ‘indeterminate’ (Fig.1).
The overall sensitivity of the tool was 75.4% (95% CI: 68.0-81.3) and
specificity was 86.6% (95% CI: 82.1-90.1). Out of 129 NMI cases detected
true positive, 112 (86.8%) were correctly classified by INDT-NMI to a
specific neuro-motor impairment type (CP, NMD or other NMI).
 |
|
NMI: Neuromotor Impairment; Other
Neurodevelopmental disability (NDD): include global
developmental delay/intellectual disability, autistic disorder,
and attention deficit/hyperactivity disorder, hearing
impairment, vision impairment and speech and language disorders.
Fig. 1 INCLEN Diagnostic Tool for
Neuromotor Impairment (INDT –NMI): Subject recruitment and
assessment.
|
Table I provides validity of the tool for
various groups of subjects without taking indeterminate cases in to
consideration. Sensitivity of the tool was between 89.7% and 83.7% for
two groups of NMI; while the specificity among normal children or those
with other NDDs was 96.4% and 91.8%, respectively.
TABLE I Psychometric Properties of INCLEN Diagnostic Tool for Neuro-motor Impairment (INDT-NMI)
(Analysis after excluding cases labeled as ‘INDETERMINATE’)*
|
Categorization as per |
Neuromotor
|
#Neuromotor |
NDDs
|
Children without
|
|
Candidate Test |
Impairment Alone |
Impairment +
|
without NMI#
|
NMI and NDDs
|
|
(N= 58) |
Other NDDs
|
(N=208)
|
(normal)#(N=56) |
|
Group-I |
(N=92) |
Group-III |
Group-IV |
|
|
Group-II |
|
|
|
Neuromotor impairment |
52 |
77 |
17 |
2 |
|
No neuro-motor impairment |
6 |
15 |
191 |
54 |
|
Sensitivity % (95% CI)
|
89.7 (78.8-96.1) |
83.7 (74.8- 90.6) |
_ |
_ |
|
Specificity % (95% CI) |
– |
– |
91.8 (87.3-95.2) |
96.4 (87.7-99.6) |
|
+Likelihood Ratio (Group 1 and III) |
11(6.9-17.4)
|
– Likelihood Ratio (Group 1 and III) |
0.1 (0.05-0.24) |
|
+Likelihood Ratio (Group 1 and IV) |
25.1 (6.4-98.2) |
– Likelihood Ratio (Group 1 and IV) |
0.1 (0.05-0.22) |
|
+Likelihood Ratio (Group I1 and III) |
10.2 (6.4-16.3) |
– Likelihood Ratio (Group I1 and III) |
0.1 (0.1-0.28) |
|
+Likelihood Ratio (Group I1 and IV) |
23.4 (5.9-91.7) |
– Likelihood Ratio (Group I1 and IV) |
0.1 (0.1-0.26) |
|
Figures in parenthesis are 95% CI; * Out of 454 subjects, 40
(8.8%) were categorized as indeterminate; 38/40 (95%) had NMI
with or without NDD and were referred for further workup.
Details of indeterminate cases are given in the text; #
These are the diagnostic categories as per expert evaluation
(Gold Standard). |
The expert (gold standard) diagnostic labels of 40
subjects categorized as ‘indeterminate’ by the INDT-NMI were: NMI alone
8; NMI + other NDD 13; NDD other than NMI 17; and Normal (without NMI or
any NDD) 2. Failure to identify hypotonia, mild spasticity, dystonia and
ataxia by the graduate physicians were the frequent reasons for NMI
cases being labeled as indeterminate. Twenty-one children (52.5%) had
intellectual disability/global development delay. Overall, out of 40
indeterminate cases, 38 (95%) had other NDDs with or without NMI;
remaining 2 children were from ‘Normal’ group and had moderate
undernutrition.
False negative cases had hypotonia (4
patients), spasticity (14 patients), ataxia (2 patients) and dystonia
(one patient). Over two-third of these (15/21) were associated with
other NDDs as well. The neuro- motor impairment was mild in most of these
children. There were 19 false positives: 17 with different NDDs
and 2 from normal category. Eleven of these children had varying degree
of intellectual disability and 2 had autism. Seizure disorder was also
present either as isolated condition (n=3) or with other NDDs (n=5).
Two children without any NDD had rickets (n=1) and moderate
under-nutrition (n=1). INDT-NMI categorized the false positives
as having CP in 17 cases and one each with NMD and other NMI.
Discussion
The diagnosis of neuro-motor impairments including
cerebral palsy is essentially clinical. In this study on development and
validation of a simple clinical tool (INDT-NMI), good psychometric
properties (sensitivity 75.4% and specificity 86.6%) were observed.
About 9% subjects were categorized as ‘indeterminate’ and most of these
(95%) were having either NMI or had another NDD.
The concept and definition of CP has changed over
years reflecting the evolving understanding of causative mechanisms and
varied manifestations [11,13-16]. To the best of our knowledge, no
validated tools for diagnosing and categorizing neuro-motor impairments
for children older than two years are available. Several assessment
tools are however, available to quantify and monitor developmental
milestones and skills in children with CP and other NMI after initial
diagnosis has been made and to assess the quality of life of patients
and their caregivers [17-20]. Tiered approach involving initial
community screening followed by diagnostic assignment by an expert have
been applied in epidemiologic studies [21-23]. Use of motor
developmental milestones to screen for delays and identify children with
CP has been evaluated in a group of high-risk, prematurely born infants
below two years of age [18-20]. Kuban, et al. [24] incorporated
selected components from standard neurological examination to an
algorithm for identifying cerebral palsy in 2-year-old children who were
born at extremely low gestational age, in a multi-centric
epidemiological study. The minimum threshold criteria for identifying
cerebral palsy were specified but the diagnosis of CP using this
algorithm was not validated using any reference standard assessment.
Similar to our study, efforts to strengthen primary care have been made
in China with recent validation of Chinese version of INFANIB for
assessing infants with neuromotor abnormalities in primary care setting
[25].
In the current study, over 86% of true positives were
correctly classified in to the various sub-types of NMI. Clinically, it
is important to differentiate CP from other neuromotor impairment and
neuromuscular disorders for deciding the line of investigations,
specific therapeutic and rehabilitative interventions, and counseling.
In our patients, 70% children with NMI had other co-morbidities like
epilepsy, global developmental delay and intellectual disabilities.
Similar findings have been described in other studies and therefore
there is need for a comprehensive assessment of all these subjects. In
any situation, once diagnosis of NMI is made in primary care,
physiotherapy can be initiated early while detailed specialist
assessment is underway. Triage questions of the INDT-NMI can potentially
be evaluated in future studies for screening of NMI in the community by
non-physician healthcare personnel.
Analysis of false positives and negatives indicated
that there is need to emphasize identification of mild changes in tone,
and dystonia through demonstration and actual hands-on practice during
training. This aspect may require extending the training by a few hours
and ensuring some patients with subtle findings for training of the
graduate physicians. Misclassification of a few moderately malnourished
children – who can have hypotonia – in to false positives is another
limitation of the tool. The performance of the tool may be better in the
hands of physicians with longer experience and among those who continue
to use it for some time. Another limitation of the study was that expert
groups adopted a clinical rather than a protocol based approach to
establish the NDD diagnosis and obtained special investigations as and
when these were considered relevant. The tool was evaluated in tertiary
care clinics while INDT-NMI is meant to be used in primary care
settings. The performance of INDT-NMI therefore needs to be
systematically evaluated in primary care of different geographic regions
and general practice environment for its diagnostic capability.
In conclusion, graduate primary care physicians with
a structured short training can administer the new tool and diagnose NMI
in 2-9 year old children with high validity. INDT-NMI requires further
evaluation in actual primary care settings. The tool will help early
diagnosis of NMI in primary care and institution of physiotherapy and
assignment to a specialist for detailed evaluation and management.
Contributors: All authors have contributed,
designed and approved the study. NKA will act as a guarantor for this
work.
Funding: Ministry of Social Justice and
Empowerment (National Trust), National Institute of Health (NIH-USA);
Fogarty International Center (FIH), Autism Speaks (USA); Competing
interests: None stated.
|
What is Already Known?
• The diagnosis of neuromotor impairments is
essentially clinical.
• Primary care physicians have limited
knowledge and skills to diagnose these conditions.
What This Study Adds?
• INDT-NMI is a simple diagnostic tool based
on algorithmic approach developed by a large group of experts
using modified Delphi technique.
• INDT-NMI demonstrated good sensitivity (75%) and
specificity (87%) to diagnose neuromotor impairments in
children.
|
References
1. Liptak GS, Murphy NA. Providing a primary care
medical home for children and youth with cerebral palsy. Council on
Children with Disabilities. Pediatrics. 2011; 128:e1321-9.
2. Strehle EM. Long-term management of children with
neuromuscular disorders. J Pediatr (Rio J). 2009; 85: 379-84.
3. Walker CW, Pickett CT. Motor impairment after
severe traumatic brain injury: A longitudinal multicenter study. J
Rehabil Res Dev. 2007; 44:975-82.
4. Mc Donald CM. Clinical approach to the diagnostic
evaluation of hereditary and acquired neuromuscular diseases. Phys Med
Rehabil Clin N Am. 2012; 23:495-563.
5. Jain R, Juneja M, Sairam S. Children with
developmental disabilities in India: age of initial concern and referral
for rehabilitation services, and reasons for delay in referral. J Child
Neurol. 2013; 28:455-60.
6. Aisen ML, Kerkovich D, Mast J, Mulroy S, Wren TA,
Kay RM, et al. Cerebral palsy: clinical care and neurological
rehabilitation. Lancet Neurol. 2011; 10:844-52.
7. Operational Guidelines, Rashtriya Bal Swathya
Karyakram (RBSK). Child Health Screening and early intervention services
under NRHM. Ministry of Health and Family Welfare. 2013. Available from:
http://www.unicef.org/india/7._Rastriya_Bal_Swaasthya_karyakaram.pdf.
Accessed January 25, 2013.
8. Juneja M, Mishra D, Russell Paul SS, Gulati S,
Deshmukh V, Tudu P, et al. INCLEN Diagnostic Tool for Autism
Spectrum Disorder (INDT-ASD): Development and Validation. Indian Pediatr.
2014;51:359-65.
9. Mukherjee S, Aneja S, Russell Paul SS, Gulati S,
Deshmukh V, Sagar S, et al. INCLEN Diagnostic Tool for Attention
Deficit Hyperactivity Disorder (INDT-ADHD): Development and Validation.
Indian Pediatr. 2014;51: 457-62.
10. Konanki R, Mishra D, Gulati S, Aneja S, Deshmukh
V, Silberberg D, et al. INCLEN Diagnostic Tool for Epilepsy (INDT-EPI)
for primary care physicians: Development and validation. Indian Pediatr.
2014; 51:539-43.
11. Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax
M, Damiano D, et al. A report: the definition and classification
of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007; 109:
8-14.
12. EPI Info 7. Center for Disease Control. Available
at http://wwwn.cdc.gov/epiinfo/ Accessed November 20, 2013.
13. Mac Keith RC, MacKenzie ICK, Polani PE. The
Little Club: memorandum on terminology and classification of cerebral
palsy. Cerebral Palsy Bulletin. 1959; 5:27-35.
14. Bax MCO. Terminology and classification of
cerebral palsy. Dev Med Child Neurol. 1964; 6:295-7.
15. Mutch L, Alberman E, Hagberg B, Kodama K, Perat
MV. Cerebral palsy epidemiology: Where are we now and where are we
going? Dev Med Child Neurol. 1992; 34:547-51.
16. Bax M, Goldstein M, Rosenbaum P, Leviton A,
Paneth N, Dan B, et al. Proposed definition and classification of
cerebral palsy. Dev Med Child Neurol. 2005;47:571-6.
17. Krigger KW. Cerebral Palsy: An Overview. Am Fam
Physician. 2006;73:91-100.
18. Allen MC, Alexander GR. Using motor milestones as
a multistep process to screen preterm infants for cerebral palsy. Dev
Med Child Neurol. 1997; 39:12-6.
19. Allen MC, Alexander GR. Screening for cerebral
palsy in preterm infants: delay criteria for motor milestone attainment.
J Perinatol. 1994;14:190-3.
20. Nickel RE, Renken CA, Gallenstein JS. The infant
motor screen. Dev Med Child Neurol. 1989; 31:35-42.
21. Rosenbaum PL, Missiuna C, Echeverria D, Knox SS.
Proposed motor development assessment protocol for epidemiological
studies in children. J Epidemiol Community Health. 2009; 63(suppl.
1):27-36.
22. World Health Organization (WHO). Research
Protocol for Measuring the Prevalence of Neurological Disorders in
Developing Countries. WHO: Geneva; 1981.
23. Kumar R, Bhave A, Bhargava R, Agarwal GG.
Prevalence and risk factors for neurological disorders in children aged
6 months to 2 years in northern India. Dev Med Child Neurol. 2013;
55:348-56.
24. Kuban KC, Allred EN, O’Shea M, Paneth N, Pagano
M, Leviton A, et al. An algorithm for identifying and classifying
cerebral palsy in young children. J Pediatr. 2008; 153: 466-72.
25. Liao W, Wen EY, Li C, Chang Q, Lv KL, Yang W, et
al. Predicting neurodevelopment outcomes for at-risk infants:
reliability and predictive validity using a Chinese version of the
INFANIB at 3, 7 and 10 months. BMC Pediatr. 2012; 12:72.
|
|
|
 |
|
