From the Department of Pediatric Gastroenterology &
Nutrition, BSM Medical University, Dhaka, Bangladesh.
Correspondence to: Dr. A.S.M. Bazlul Karim,
Associate Professor of Pediatric Gastroenterology & Nutrition, BSM
Medical University, Shabagh, Dhaka, Bangladesh. E-Mail:
karimb@bangla.net
Manuscript received: June 18, 2003; Initial review
completed: December 9, 2003; Revision accepted: February 4, 2004.
Abstract:
Caroli’s disease is a rare communicating segmental
or diffuse dilatation of the intrahepatic biliary tree. Cholangitis,
liver cirrhosis and cholangiocarcinoma are its potential
complications. A case of Caroli’s disease in a boy of 6 years with
bilobal involvement presenting with intermittent abdominal pain, fever
and hepatomegaly is reported here.
Key words: Abdominal pain, Caroli’s disease.
Cystic diseases of the bile ducts are rare
congenital anomalies and are common in Japan and Asia. Most cases are
diagnosed in children less than 10 years of age(1). In 1958, Jacques
Caroli first described a rare congenital condition characterized by
non-obstructive saccular or fusiform multi-focal segmental dilatation
of the intra-hepatic bile ducts(2). The mode of inheritance is still
uncertain but in majority of cases it is transmitted in an autosomal-recessive
fashion(3) while in one family the mode of inheritance appeared to be
autosomal dominant(4). The main clinical features are recurrent
cholangitis and hepatomegaly(5).
Case Report
A six-year-old male boy presented with the
complaints of intermittent fever and right upper quadrant abdominal
pain for 3 years. Fever was associated with chills and rigor. There
was no remarkable past history. He is the second son of a first degree
consanguineous marriage and the other sib is healthy. On physical
examination he was found non-icteric and his liver edge was 10 cm from
the right costal margin in the mid-clavicular line. Liver consistency
was firm and it was not tender. Spleen was not palpable. Other
physical signs were unremarkable. Laboratory investigations showed
poly-morphonuclear leukocytosis with moderate elevation of ESR. Liver
function tests like ALT, bilirubin, PT, alkaline phosphatase and
albumin were within normal limit. Routine urine examination, kidney
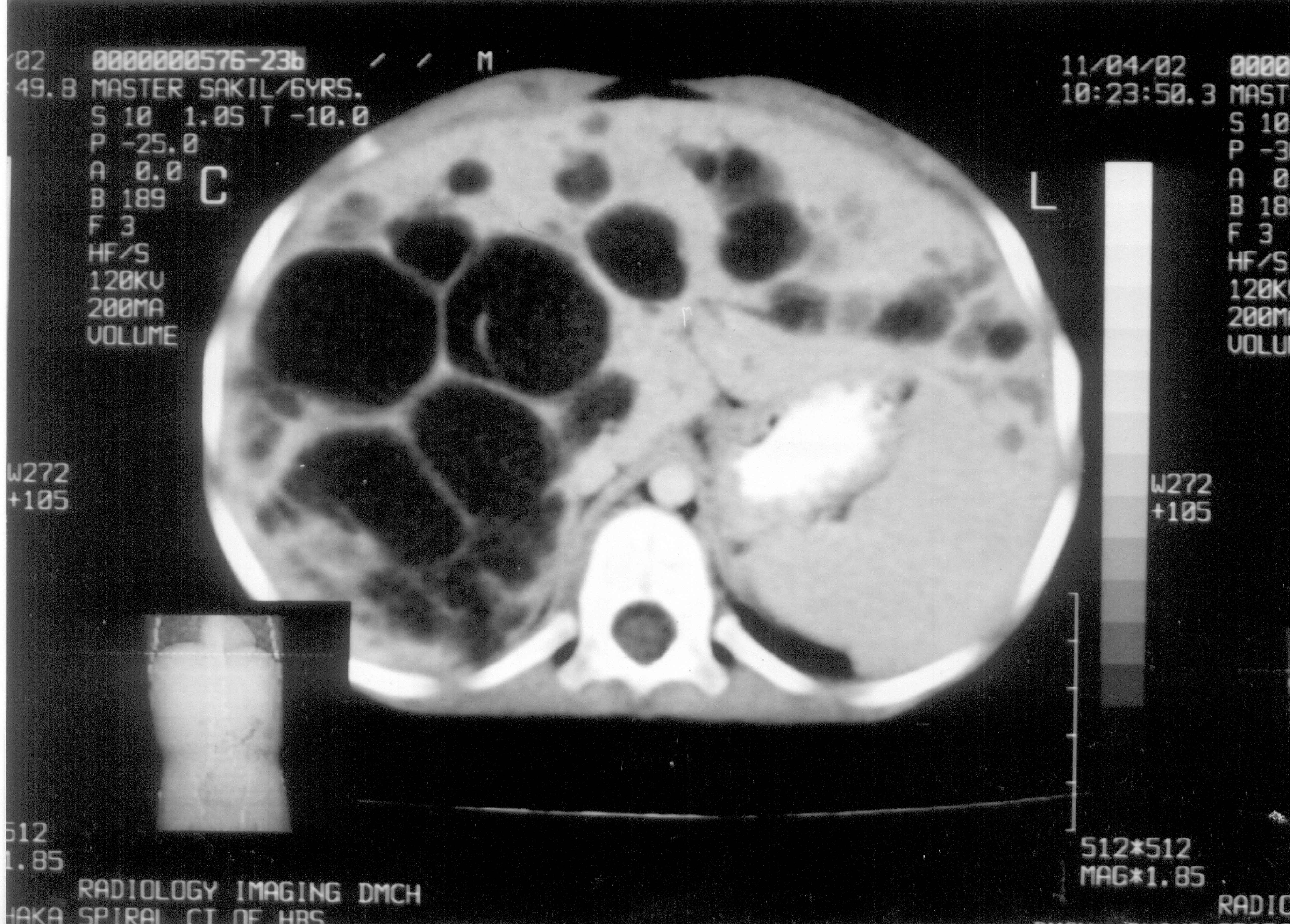
function tests and x-ray chest were normal. Ultrasound (US) and
computed tomography (CT) of abdomen (Fig. 1) showed multiple cystic
dilated bile ducts with bridge formation within the liver occupying
the both lobes but more in the right lobe. No feature of hepatic
fibrosis was seen and both the kidneys were normal. Cholangiography
though helpful, was not possible due to technical reason. Liver
biopsy, for exclusion of associated congenital hepatic fibrosis (CHF),
was not done because CT scan was not suggestive and there was absence
of clinical evidence of portal hypertension. A diagnosis of isolated
Caroli’s disease was made and the child was treated conservatively
with antibiotics. Partial hepatic lobectomy was advised but parents
did not agree. The parents were subsequently counseled, properly
advised and asked to come for regular follow-ups.
 |
|
Fig. 1. Contrast enhanced CT scan of liver
shows multiple intra-hepatic biliary dilatation, more in the
right lobe. |
Discussion
There are two forms of Caroli’s disease, one
associated with congenital hepatic fibrosis and a simpler form
occurring alone. The former, called Caroli’s syndrome is associated
with portal hypertension. The later, known as Caroli’s disease, may be
associated with autosomal recessive polycystic kidney disease(6) or
rarely with autosomal dominant polycystic kidney disease(7). Caroli’s
disease has also been reported in patient with choledochal cysts for
which reason some authorities classify it as a type of choledochal
cyst(8). Caroli’s disease may be localized to one lobe of liver or may
be diffuse. It results from an arrest in ductal plate remodeling at
the level of the larger intra-hepatic bile ducts(3).
Caroli’s disease usually presents with intermittent
abdominal pain and hepato-megaly. Cholangitis, cholelithiasis, bilary
abscess, septicemia, liver cirrhosis and cholangiocarcinoma are all
its potential complications. Malignant complication (cholangiocarcinoma)
occurs in approxi-mately 7% of cases(1) and is due to prolonged
exposure of the ductal epithelium to high concentration of
unconjugated secondary bile acids(9).
The diagnosis of Caroli’s disease rests on
demonstrating that the cystic lesions are in continuity with the
bilary tree. It can be done by imaging studies such as abdominal USG,
CT scan, isotope scan, ERCP, PTC and MRCP. These studies demonstrate
irregular cystic dilatation of the large proximal intra-hepatic bile
ducts with normal ducts in between.
The treatment of Caroli’s disease depends on the
clinical features and the location of the biliary abnormalities.
Cholangitis is treated with appropriate antibiotics. In case of
intrahepatic cholelithiasis litholytic therapy with urso-deoxy cholic
acid (UDCA) is indicated(10). When the ductal abnormalities are
localized to one lobe, lobectomy relieves symptoms and appears to
remove the risk of malignancy. In case of diffuse involvements of both
lobes of liver, treatment options include conservative management,
endo-scopic therapy (sphincterotomy for clearance of intra-hepatic
stone), internal biliary bypass procedures and in carefully selected
cases liver transplantation(3). Those who can not be operated
radically should have regular clinical follow ups including ultrasound
and liver biopsy as necessary. Further family studies are needed in
all cases to exclude the autosomal dominant mode of inheritance(4).
Abdominal pain is a common pediatric problem and
though it is a rare congenital anomaly one should keep in mind the
possi-bility of Caroli’s disease in its differential diagnosis
especially in children who present with intermittent fever and
hepatomegaly along with abdominal pain.
Funding: None.
Competing interests: None stated.
