|
|
Images in Clinical Practice Indian Pediatrics 2002; 39:400 |
||||
|
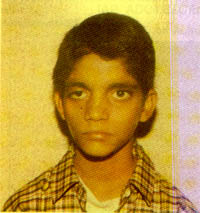
Aarskog Syndrome |
||||
|
Aarskog Syndrome is a common syndrome of proportionate short stature described by Aarskog in 1970. The facial dysmorphic features are subtle but together give a characteristic appearance. Shawl scrotum without hypoplastic genitalia in a child with short stature is quite diagnostic of Aarskog syndrome but may be absent in 20% of cases and the appearance is lost in postpubertal boys. Most patients are of normal or low normal intelligence, however, mild and moderate mental retardation may be present in upto 30% of cases. Height initially is less than third centile, but there is usually some catch-up growth during puberty, which may be delayed in some cases. Aarskog syndrome is an X linked disorder and the responsible gene is faciogenital dysplasia (FGD1) gene on Xp11.21.
Vandana Chaddha,
Correspondence to: |
![]()