|
|
|
Indian Pediatr 2021;58:
576-583 |
 |
Integrating
Child Protection and Mental Health Concerns in the
Early Childhood Care and Development Program in
India
|
|
Chaitra G Krishna, 1
Sheila Ramaswamy,1
Shekhar Seshadri2
From 1SAMVAD (Support, Advocacy & Mental Health
Interventions for Children in Vulnerable
Circumstances and Distress), Department of Child &
Adolescent Psychiatry; and 2Department of Child and
Adolescent Psychiatry, National Institute of Mental
Health & Neurosciences (NIMHANS); Bangalore,
Karnataka.
Correspondence to: Dr Shekhar Seshadri, Senior
Professor, Department of Child and Adolescent
Psychiatry, and Associate Dean, Behavioral Sciences,
National Institute of Mental Health and
Neurosciences (NIMHANS), Bangalore 560 029,
Karnataka, India.
[email protected]
Published online: February 25, 2021;
PII: S097475591600299
|
|
T he term
‘child protection’ refers to preventing
and responding to violence, exploitation, abuse
and neglect of young children. Article 19 of
the United Nations Convention of Children’s Rights
(UNCRC/CRC), 1989 provides children a specific right
to protection [1]. About 13.5% of India’s
population, 16.45 crore children, are in the age
group 0-6 years [2]. According to a national study
conducted by Ministry of Women and Child Development
(MoWCD), on child abuse in India, 66% are reported
to be physically abused, 50% have faced one or more
forms of sexual abuse and emotional abuse [2,3]. As
per the National Crime Records Bureau’s 2017 report
on crime against children, a total of 129032 cases
were recorded, including kidnapping and abduction,
sexual offences and murder [4]. A total of 32,608
child sexual abuse cases were recorded in 2017
alone, including for children below 5 years of age
[5] and a total of 78,000 orphan and vulnerable
children are residing in child care institutions
under the Integrated Child Protection Scheme (ICPS)
[6]. Child protection is thus becoming an increasing
concern in India, creating new imperatives to
address it amongst all children, but particularly
children below 6 years of age, who due to their age
and developmental abilities are rendered more
vulnerable than older child populations.
Due to paucity of age-specific
data, it is unclear as to what proportion of abused
children are between 0 to 6 years of age. Many
behaviors such as defiance, anxiety to new
situations, which are considered pathological in
older children, constitute normal development in
young children. Thus, it is difficult to
differentiate between normal and pathological
behaviors, making mental health diagnosis in young
children difficult [7]. Due to their developmental
age, and their lower verbal communication skills,
they are also hindered from reporting experiences
[8], consequently rendering them more vulnerable
than older children, to traumatic death and injury
caused due to abuse and neglect [9-11].
There is now considerable
evidence to show that adverse experiences in early
childhood also have a negative impact on young
children’s overall development and so, if not
addressed, may lead to adverse outcomes in later
years. For instance, children’s exposure to frequent
and prolonged abuse, neglect, violence, substance
abuse in caregivers, family and economic stressors,
and poor attachment relations negatively impacts
their mental health, neurodevelopment, psychosocial
development and academic functioning [14-17]. Mental
health is impacted by increasing the risk of
internalizing and externalizing problems such as
anxiety, depression and suicide [18,19], antisocial
behavior and psychopathy [20], substance abuse, and
legal problems in their adult life [21-23]. The
risks of adverse childhood experiences also combine
with the disciplinary strategies used with children,
including all forms of corporal punishment, to
result in increased risk of negative behavioral,
cognitive, psychosocial, and emotio-nal outcomes
among children [24].
Since critical brain development
occurs in the early years of life [25], it is
important to note that child protection in early
childhood critically involves, but is not restricted
to, abuse and neglect. Child protection in early
childhood also entails protection from the adverse
influences of unmet developmental needs along with
the other interventions. According to the Adverse
childhood experiences studies, the relationship
between adverse childhood experiences and negative
health indicators begins early in childhood; child
care service providers thus have an opportunity to
provide interventions that prevent long-term
negative health consequences [26]. Child protection,
therefore involves addressing risks relating to
neglect, (physical, sexual and emotional) abuse, and
absence of opportunities (for learning and
development).
INTEGRATING CHILD PROTECTION INTO EARLY CHILDHOOD
CARE AND DEVELOPMENT PROGRAMS
Early Childhood Care and
Development (ECCD) programs across the world majorly
focus on nutrition and early stimulation along with
other health interventions such as immunization,
hygiene, educational and support measures for
caregivers to ensure consistent care and support for
children. Even though ECCD programs work with
multiple departments, they have limited
colla-boration with child mental health and child
protection systems [27].
While there are child protection
programs around the world, those working
specifically in the context of early childhood, are
relatively limited. For those that do work in the
area of early childhood, there are very few that
integrate ECCD issues with child protection.
Examples of integrated programming include UNICEF’s
programme guidance for early childhood development
[28] and Plan International’s development of program
models and tools to integrate child protection into
ECCD, as reflected in their exploratory studies in
Uganda, Bolivia and Timor-Leste [29]. Save the
Children, has also attempted, in few of their
programs, to integrate child protection into ECCD
but while they focus on orphans and vulnerable
children, they do not have a mental health component
[30].
There are examples of child
violence prevention programs, which have been
successfully implemented both in developed and
developing countries [29,31-35], through parents,
nurses or community health worker in the primary
health care system. These have focused, and
legitimately so, mostly on positive parenting,
monitoring for prevention child maltreatment
(through home visits by community health care
workers), mother–child therapy interventions,
provision of primary health care services and safe
spaces for children to grow and play. However, these
programs have worked largely in family settings–an
approach that India could draw upon but that would
not be entirely applicable to its context, because
the socio-economic situation of many vulnerable
children often does not allow for family members to
be present for the child. Therein lies the
importance, in the Indian context, of the role of
the ECCD workers and the need to integrate child
protection into the government preschool system.
The key objectives of ECCD and
child protection programs are to ensure
age-appropriate development, early stimulation and
primary prevention. The World Health Organization’s
Nurturing care framework also recommends providing
for the children’s physical and emotional needs,
protection from harm along with learning and
development opportunities as its central tenet [36].
Given that ECCD programs qualify as a universal
intervention, their coverage tends to be wide, and
ECCD workers and educators are ideally placed to
implement protection strategies to assist children
at risk of abuse and neglect [37]. Thus, ECCD
programs may serve as effective vehicles to protect
children from adversities.
Furthermore, as erstwhile
described, exacerbated by poverty and other
vulnerabilities, mental health needs of children
from adverse circumstances are high – placing
children at increased risk of continued child
protection problems. Thus, it is imperative for
integrated ECCD and child protection programs to
include child mental health interventions.
Effectively addressing emotional and behavioral
problems that are consequences of protection issues,
would be critical to the successful implementation
of early childhood care and protection services and
programs [9].
We, herein, address the question
of how to integrate child protection and mental
health interventions into existing ECCD programs by
describing the experience of a pilot project in the
Indian context. It provides the rationale,
methodology and content of service delivery for
integrating child protection and mental health
interventions into the existing ECCD program, the
Integrated Child Development Scheme (ICDS),
highlighting emerging concerns and challenges and
drawing from the interventions to show how some of
these were addressed. We also discuss how child care
service providers, particularly pediatricians, can
play a pivotal role in this endeavor.
Experience With a Pilot Project
Prior to this pilot project a
large community-based child and adolescent mental
health service project, had been implemented by us.
The community-based project had executed a resource
mapping and needs assessment for community child and
adolescent mental health services [4], prior to the
start of its activities. With the objective of
promoting early stimulation and optimum development
in children, activities such as implementation of
early stimulation, training and capacity of
Anganwadi workers on early stimulation (child
protection was not a prominent focus of the program
at the time) were conducted. The observations and
experiences of our work are available elsewhere (www.nimhans
childproject.in).
Subsequently this experience was
used to develop a pilot project that focused
exclusively on ECCD inter-ventions, to include child
mental health and protection interventions. In order
to obtain a more specific under-standing of how ICDS
staff view child protection issues, an additional
assessment was done prior to this project, and the
findings incorporated into the design and content of
the interventions.
Context of Intervention
The potential of the integrated
child development scheme: The ICDS
provides a huge opportunity to incorporate
protection components into ECCD because of its
universal coverage agenda, particularly in
socio-economically deprived communities where some
of the most vulnerable children reside. Also, the
anganwadi worker, the key worker in the ICDS scheme,
conducts non-formal education and early stimulation
activities for a given group of children, on a daily
basis, over a relatively long time period (such as a
year). This provides a perfect platform, not only
for early screening and referral for developmental
delays, emotional and beha-vioral and protection
issues, but also to engage children in personal
safety awareness programs.
Protection programs, policies and
laws relevant to young children: As a signatory
to the UNCRC, the Indian Government established a
statutory body, the National Commission for
Protection of Child Rights (NCPCR), in 2007, and
more importantly, the Ministry of Women and Child
Development, launched the Integrated Child
Protection Scheme (ICPS) in 2009. The ICPS
translates into programs, the vision of a secure
environment for all children, as envisaged in the
Juvenile Justice (Care and Protection of Children)
Act, 2015, which in turn is based on principles of
‘protection of child rights’ and ‘best interest of
the child’. It aims at building a protective
environment for children in difficult circumstances,
as well as other vulnerable children, by bringing
together various child protection schemes under one
roof and integrating additional interventions for
protecting children and preventing harm [39].
India has enacted another key law
with regard to child protection – The Protection of
Child Sexual Offences (POCSO) Act 2012 which aims to
effectively address sexual abuse and sexual
exploitation of children. The act defines various
forms of sexual abuse, focuses on mandatory
reporting issues, stringent punishment graded as per
the gravity of the offence, and requisite
child-friendly court processes [40].
Despite the existing range of
ECCD programs and services, there are gaps and
challenges, at knowledge, skill and policy levels,
leading to inadequate realization of child
protection laws and policies. Some of the challenges
observed during the course of our child mental
health and protection work in recent years include:
limited understanding of child protection and
psycho-social issues within child protection system,
lack of focus on protection services for young
children, inadequate knowledge and skills to
identify and address protection concerns, especially
in young children and paucity of systematic and
standardized materials and protocols for child
protection response.
ICDS staff knowledge and skills
in child development and protection issues:
Based on the needs assessment exercise conducted
with anganwadi workers within the ICDS, for a deeper
understanding on the staff’s perspectives on young
child protection, various issues emerged (which also
reflect the general lacunae in the child protection
system in the country). Anganwadi workers have not
been trained in the use of systematic assessments in
child protection, nor in assessment of child mental
health and development issues.
Young children in anganwadis:
The children in the Anganwadis are drawn from
vulnerable homes and communities. Their families
were characterized by low socio-economic status,
residence in urban slums, sub-stance abuse in
caregivers, domestic violence, violence and conflict
(extending through neighbor-hoods). The primary
caregivers were frequently day laborers, so they
were absent for most of the day i.e. as such
children’s interactions with primary caregivers were
limited to a couple of hours a day. Consequently,
they spent the maximum number of hours at the
anganwadi, with the anganwadi worker serving as a
key caregiver.
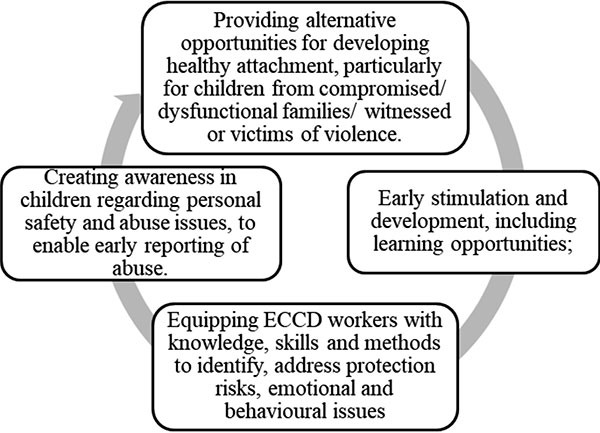
Conceptual framework:
Based on the available literature, a comprehensive
framework for integration would entail the
following: i) early stimulation and
development, including provision for learning
opportunities; ii) providing alternative
opportunities for developing healthy attachment,
particularly for children who are from compromised
or dysfunctional families; iii) creating
awareness in children regarding personal safety and
abuse issues to enable early reporting of abuse
experiences; and iv) equipping ECCD workers
with knowledge, skills and methods to identify
protection risks in young children. Including
emotional and behavioural issues, and to address
them, depending upon the severity.
The aim of the intervention was
to integrate mental health and protection services
for young children between the ages of 0 to 6 years
into the existing the ICDS program.
Methodology
As shown in Fig.1, we used
a multi-pronged approach to provide com-munity-based
mental health and protection services for promotive,
preventive and curative care through direct service
delivery for children, and training and
capacity-building of anganwadi workers.
 |
|
Fig. 1 Conceptual
framework for integration of child
protection and mental health with early
childhood care and development.
|
The interventions were
implemented in anganwadis in which the ICDS is
implemented, in vulnerable urban communities the
Bangalore. Anganwadis from the five (urban slums)
near our center were selected. From amongst these,
anganwadis were selected, which had greater
number of children, and more than one center in the
same location were selected – in order to ensure
that a greater number of children would be reached
through a single visit.
Results
In all, during the 7 months, the
interventions were carried out in 31 Anganwadi
centers (Table I). Based on the
context of intervention and the conceptual
framework, two types of interventions were
implemented to integrate child mental health and
protection into the ICDS program, through i) direct
services for children and ii) capacity building
initiatives for ICDS staff.
Table I Interventions and Coverage
| Outcomes |
Coverage |
|
Number of anganwadis and anganwadi workers
reached |
31 |
| Number of individual
assessments done for examining |
237 |
| developmental, mental
health and protection issues |
|
|
Number of group sessions conducted with the
anganwadi
|
190 |
| children |
|
| Number of children
reached through group activities |
276 |
|
One day training workshops for anganwadi
workers |
4 |
|
Number of weekly training sessions for
anganwadi workers |
89 |
Direct services for children:
This was carried out in two distinct steps viz.,
individual assessment of development, mental health
and protection issues in anganwadi children, and
group activities for children in anganwadis.
An assessment proforma comprising
of questions on child development, emotional and
behavioral issues and protection concerns was
developed (available at:
https://www.nimhanschildproject.in/anganwadis-phcs/).
It was based on existing clinical assessment
proformas at the department of child and adolescent
psychiatry in a tertiary care facility. The proforma
has also drawn from the community-based programs
previously executed by the authors, particularly in
young child institutions, where children orphan and
abandoned children, with serious child protection
issues, reside. This assessment was not primarily
aimed at arriving at a diagnosis, but mainly geared
to help child care service providers to identify and
understand children’s problems and vulnerabilities,
with a view to helping them to access appropriate
inter-ventions. Due to the variation in
developmental abilities and needs, the proforma was
adapted to three sub-groups of children under the
age of 6 years: 0 to 1 year, 1 to 3 years and 3 to 6
years.
The assessments were conducted in
the anganwadi. An average of 20 minutes was spent
engaging with the child and about 15 minutes with
the anganwadi worker, for completion of an
individual child’s assessment. To ensure that the
assessments were accurate i.e., that they truly
reflected children’s developmental abilities,
allowing them to respond freely, ice-breakers and
group activities were used to build rapport with
children Developmental checklists were filled out by
observing the child and asking him/her to perform
simple tasks and activities that would allow for
assessment of develop-mental skills and abilities.
Information about the child’s family context and
related protection issues was gathered by
interviewing anganwadi workers and helpers.
Following each assessment, for
mild to moderate developmental, mental health and
protection issues, the anganwadi worker was provided
with first level inputs including what the Anganwadi
worker may do to help the child, and how she could
counsel the parents. For complex issues (such as
developmental disabilities) requiring specialized
assistance, the anganwadi worker was assisted to
refer the child to the dept. of child and adolescent
psychiatry of a tertiary care facility and/or to the
concerned child welfare committee.
Group activities were conducted
with the anganwadi children along with anganwadi
workers (also as part of their capacity building
through demonstration and on-the-job training).
These group sessions with children, focused on
domains of development, mental health and
protection, and comprised of the following:
Activities for promotion of early stimulation and
optimum develop-ment in the five key areas of child
development (physical, social, speech and language,
cognitive and emotional development). including fine
motor activities to develop pre-writing skills;
Activities for socio-emotional develop-ment, with a
focus on helping children recognize and manage
emotions, and develop empathy; and, Activities for
child sexual abuse prevention and personal safety.
Capacity building of anganwadi
workers: This was done using capacity building
workshops and on-the-job training.
One of the key objectives of the
intervention was to build the knowledge and skills
of the anganwadi workers in the areas of child
development, mental health and protection. The
specific training objectives included enabling
anganwadi workers to: Understand the context of
child abuse and neglect, including physical,
emotional and sexual abuse; Identify and provide
first level and emergency responses and necessary
referrals in the context of child abuse and neglect;
Administer the assessment proforma to child
developmental, protection and mental health needs
and issues in individual children; Use personal
safety and sexual abuse prevention module with
preschoolers; and, identify and manage (including
refer) emotional and behavioral problems,
develop-mental and protection issues among young
children.
The training content is detailed
in Box I. It was delivered using creative
participatory and experiential methods, such as role
play, case discussions, simulation games,
demonstrations, brain-storming, pile sorting/
listing – so that the learning was made fun and
interesting, but also to enable workers to learn
necessary methodologies for use with young children.
|
Box I Training Content
for Integrated Child Development, Mental
Health and Protection Programming
Children and childhood
Setting the tone:
Re-connecting with childhood
Child development basics
Power and rights
Child development
Physical development
Speech and language
development
Cognitive development
Social development
Emotional development
(Including demonstration of early
stimulation activities in five domains of
developmentand development of low-cost early
stimulation materials)
Identifying problems and
contexts: the child’s experience and inner
voice
Understanding the child’s
experience and inner voice
Identifying and
understanding child’s behavior using the
context, experience and inner voice
framework
Understanding and
responding to common emotional and behavior
problems in early childhood
Different methods of
responding to emotional and behavioral
concerns
Managing the aggressive
and oppositional child
Management of children
with temper tantrums
Identifying and
understanding an ADHD child
Conceptual understanding
of child protection in early childhood
Introduction to child
protection issues specific to early
childhood
Introducing government
systems and programs available for child
protection
Understanding child
sexual abuse in early childhood
Child sexual abuse basics
First level psychosocial
responses for sexually abused children
Introduction to the child
sexual abuse prevention module
Practicing the child
sexual abuse prevention module
Assessing children for
developmental, mental health and protection
issues in early childhood
Assessment of child
development issues in early childhood
Assessment of emotional
and behavioral problems in early childhood
Assessment of child
protection issues in early childhood
*The content is available as a training
manual at:
https://www.nimhanschildproject.in/training-and-capacity-building/training-manuals-materials-for-child-care-service-providers/
|
Over a 7-month period, training
and capacity building activities were conducted
through 4 one-day workshops, which were held once in
two months, at the tertiary care facility that the
project was based out of. Other times, weekly
sessions were held on an on-going basis, for
clusters of anganwadis (4 to 12 Anganwadi
workers) located near each other. This enabled
Anganwadi workers to avoid travelling long distances
to attend training; and it allowed them to complete
their morning tasks com-fortably in order to free up
their time for the afternoon session. The training
team ensured that a friendly, light-hearted learning
environment was created in the Anganwadi and in
workshops.
Alongside the training, daily
field visits were used by the team, to provide
on-the-job support to the anganwadi workers. This
included demonstrations on conducting activities for
early stimulation and development, and for personal
safety and abuse prevention, administration of the
assessment proforma and management of common
emotional and behavioral problems in young children.
Additionally, revision and recap of some of the
training workshops/sessions were also done in
one-on-one sessions with anganwadi teachers, to help
them link theory and practice issues in the field.
Development of activities and
materials for use with children: In order to
provide Anganwadi workers with standardized methods
in their direct work with children, several
materials have been developed for intervention
purposes. Some of these materials were also
translated into the local language. The materials
include the following: activity book for
socio-emotional develop-ment in pre-school children;
child sexual abuse and personal safety module -
activity-based awareness and learning for
preschoolers and children with developmental
disabilities; early stimulation and development
activity books and flip charts (for use with
parents, teachers and caregivers); Stories for
preschoolers on themes of loss and grief, separation
anxiety and attachment, etc. (material available at:
https://www. nimhanschildproject.
in/interventions/pre-school-0-to-6-years/).
Given the contextual challenges
of the anganwadi workers, the team developed and
adopted several types of strategies, throughout its
implementation processes, so as to provide for a
more enabling learning and work culture and
environment for the workers (Box II).
|
Box II Specific Strategies
Adopted for Capacity Building of Anganwadi
Workers
Use of creative methods
in training, also to understand importance
of child-friendly methods
• Shorter and more
focused learning with an element of
continuity and follow up.
• Contents were tailored
to the learning abilities of the Anganwadi
workers.
• Minimal use of lecture
methods; increased use of experiential,
creative and participatory methods,
• Creation of a sense of
anticipation and enthusiasm amongst the
workers, and also gave them a sense of the
importance of methodology in child work.
Connection, not
correctional approaches
• Listening, recognizing
and validating the Anganwadi workers’
experiences and concerns.
• Assurance that the
intent was to reduce, not increase their
work burden.
• Assurance that the
objectives were neither to criticize nor
report but to understand and support their
work, to enhance what they are already
doing, so as to benefit children.
Helping workers with time
management
• Helping with time
management and enabling balance between
administrative responsibilities and child
work.
• Enabling daily
schedules to allow time for direct work and
non-formal education activities with
children.
Motivational strategies
• Creation of WhatsApp
group as a shared learning platform to allow
for peer learning and appreciation of new
techniques and creativity.
• Encouragement of
posting of videos for visual (peer)
learning.
• Creation of a book of
children’s songs for early stimulation (with
the names of the Anganwadi workers who
contributed).
Revision and review
• Encouragement to
initiate new activities that help translate
theory into concept.
• Competitions wherein
Anganwadi workers were asked to create and
share low cost aids for early stimulation
(with prizes/rewards for some of the most
creative efforts–but in a spirit of fun and
friendship).
• No criticism or blame
was laid on a worker who was unable to do
‘homework’ activities.
• Appreciation for workers who
implemented ‘homework’ activities’, with an
emphasis on the positive aspects of the
activity designed.
|
Process outcomes of interventions:
Since our interventions were not part of a research
study, no measures were used to examine the
effectiveness of the interventions we provided.
However, based on observations and feedback received
from anganwadi workers, some critical qualitative
process outcomes, mainly in terms of anganwadi
workers’ attitudes and learning were found. The
anganwadi workers over come their initial
reluctance, appreciated learning relevant skills and
interventions, and became more aware of the child
protections risks and interventions.
LESSONS LEARNT
As evidenced by the gaps in
literature, there is little data on young child
protection and mental health issues in developing
contexts, including in India. It is critical
therefore for research and intervention studies to
be undertaken in non-clinical, community settings to
better understand health, protection and
developmental issues in some of the most vulnerable
children in our country i.e. those who are least
likely to access protection and mental health
services. Whether for action research or
programmatic interventions, the existing ECCD
program, namely the ICDS, with its coverage and
reach, provides the best chance that a low resource
country such as India has, to protect its most
vulnerable children.
While a great many systemic
measures and changes are required to enable the ICDS
to gear itself to integrated programming that
straddles child development, pro-tection and mental
health, child health experts, who are already
available within the secondary and tertiary levels
of healthcare, can initiate transformations through
the approaches they bring to child services.
Pediatricians usually see children and families
regularly and over a long period, thus having the
advantage of trust and a personal relationship that
allows them to gain a deeper knowledge of the
child’s background, including family systems and
dynamics. The relationship pediatricians have with
the children and parents is devoid of the stigma
usually associated with mental health and child
protection professionals, thus causing parents and
caregivers to be more open and receptive to their
suggestions and inputs [41]. Consequently, they are
well-placed to pick up on child protection concerns
and provide recommendations and/or referrals to
child protection systems [42]. Pediatricians can
also lead the way in child protection in India,
including to provide capacity building support to
the ICDS.
The training courses conducted by
job training centers who provide capacity building
programs to anganwadi workers require major
re-examination and over-hauls, so that they develop
integrated conceptual frameworks and interventions
that cater to the critical domains of early
childhood development, protection and mental health,
and use pedagogies that are appropriate to those who
work with young children–the use of creative and
participatory methodologies in training programs are
more likely to be translated into practice at field
level, in direct work with children.
It is true that anganwadi workers
experience a great many challenges and thus work
under extraordinarily difficult conditions. It is
understandable that high workloads, and lack of
health insurance, to serve as demotivating factors
for them. This is why methodology is as critical as
the content – more so perhaps in this context. The
challenge is not so much about the potential
opportunities these programs and systems provide for
the integration of protection services for young
children, rather how best to plan an intervention
through which the capacities of the service
providers could be developed by navigating through
their many challenges.
We have begun work with state
departments on sharing the models and methods
described in this paper. In conclusion, experiences
from our pilot project suggest that an empathic
approach, that acknowledges the anganwadi workers
challenges and limitations, and takes them into
consideration in program design, would be the way
forward. The use of less conventional approaches
that are built into local traditions and cultures,
creating community-based forums that workers are
keen to be a part of, is a key strategy for making
space and time for their capacity building and for
their work with children. We have begun work with
state departments on sharing the models and methods
described in this paper. In addition to the
commitment of the ICDS scheme and its functionaries,
further work, research and experiences across the
country will determine the scalability of these
methods.
Funding: United Nation
Children’s Fund (UNICEF), India; Competing
interests: None stated.
REFERENCES
1. The United Nations. Convention
on the Rights of the Child. Treaty Series 1989;
1577, 3. Accessed Apr 2, 2020. Available from:
https://www.ohchr.org/documents/professionalinter
est/crc.pdf %0A%0A
2. Statistical Report on Children
of India. Ministry of Women & Child Development.
Governement of India. Children in India 2018 -A
Statistical Appraisal. Accessed Apr 26, 2020.
Available from:
http://mospi.nic.in/sites/default/files/publi
cation_reports/Children%20in%20India%202018%20%E2
%80%93%20A%20Statistical%20 Appraisal_26oct18.pdf
3. Seth R. Protection of children
from abuse and neglect in India. JMAJ. 2013;56;5.
4. National Crime Records Bureau.
Crime in India. Ministry of Home Affairs. Government
of India. Accessed Apr 25, 2020. Available from:
https://ncrb.gov.in/crime-in-india-table-addtional-table-and-chapter-contents?field_date_
value%5 Bvalue%5D%5Byear%5D=2017&field_select_
table_title_ of_ crim_value= 6&items_per_page=All
5. Ministry of Women and Child
Development. PIB: Cases Filed Under POCSO. 2019.
Accessed Apr 25, 2020. Available from:
https://pib.gov.in/newsite/pmreleases.aspx?mincode=
64
6. Ministry of Women and Child
Development G. PIB: Ministry of Women & Child
Development -Year End Review 2018. 2019. Accessed
April 25, 2020. Available from:
https://pib.gov.in/newsite/pmreleases.aspx?mincode=64
7. Koot, H.M., Van Den Oord,
E.J.C.G., Verhulst, F.C. et al. Behavioral and
Emotional Problems in Young Preschoolers:
Cross-Cultural Testing of the Validity of the Child
Behavior Checklist/2-3. J Abnorm Child Psychol.
1997;25:183-96.
8. World Health Organization.
Child abuse and neglect. Accessed April 5, 2020.
Available from: http://www. who.int/violence_injury_prevention
9. Osofsky JD, Lieberman AF. A
call for integrating a mental health perspective
into systems of care for abused and neglected
infants and young children. Am Psychol. 2011;
66:120-8.
10. Margolin G, Gordis EB.
Children’s Exposure to Violence in the Family and
Community. Curr Dir Psychol Sci. 2004; 13:152-5.
11. Runyan D, May-Chahal C, Ikeda
R, Hassan F, Ramiro L. Child abuse and neglect by
parents and other caregivers. World Rep Violence
Heal. 2002;57-86.
12. Prado EL, Dewey KG. Nutrition
and brain development in early life. Nutr Rev.
2014;72:267-84.
13. Baker-Henningham H, Lopez-Boo
F. Early childhood stimulation interventions in
developing countries: A comprehensive literature
review. IZA Discussion Paper No. 5282. 2010.
Accessed February 25, 2020. Available from:https://papers.ssrn.com/sol3/papers.cfm?abstract_
id= 1700451
14. Saarela JM. Time Does Not
Heal All Wounds: Mortality Following the Death of a
Parent. J Marriage Fam. 2011; 73:236-49.
15. Wade M, Zeanah CH, Fox NA,
Tibu F, Ciolan LE, Nelson CA. Stress sensitization
among severely neglected children and protection by
social enrichment. Nat Commu. 2019; 10:57-71.
16. Mills R, Alati R, O’Callaghan
M, et al. Child abuse and neglect and cognitive
function at 14 years of age: Findings from a birth
cohort. Pediatrics. 2011;127:4-10.
17. Teicher MH, Samson JA,
Anderson CM, Ohashi K. The effects of childhood
maltreatment on brain structure, function and
connectivity. Nature Rev Neurosc. 2016;17: 652-66.
18. Smith M, Mcisaac J-L. Adverse
Childhood Experiences: Early Childhood Educators
Awareness and Perceived Support [Internet]. Mount
Saint Vincent University; 2019. Accessed August 16,
2020. Available from: http://ec.msvu. ca/xmlui/handle/10587/2090
19. Jimenez ME, Wade R Jr, Lin Y,
Morrow LM, Reichman NE. Adverse experiences in early
childhood and kindergarten outcomes. Pediatrics.
2016;137:e20151839.
20. Kolla NJ, Malcolm C, Attard
S, Arenovich T, Blackwood N, Hodgins S. Childhood
maltreatment and aggressive behavior in violent
offenders with psychopathy. Can J Psychiatry.
2013;58:487-94.
21. Putnam FW. The Impact of
Trauma on Child Development. Juv Fam Court J.
2006;57:1-11.
22. Young JC, Widom CS. Long-term
effects of child abuse and neglect on emotion
processing in adulthood. Child Abuse Negl.
2014;38:1369-81.
23. Storr CL, Nicholas Ialongo
SS, Anthony JC, Breslau N. Childhood antecedents of
exposure to traumatic events and posttraumatic
stress disorder. Am J Psychiatry. 2007;164: 119-25.
24. Sege RD, Siegel BS. Effective
discipline to raise healthy children.
Pediatrics.2018;142:e20183112.
25. Tierney AL, Nelson CA. Brain
Development and the Role of Experience in the Early
Years. Zero Three. 2009;30:9-13.
26. Flaherty EG, Thompson R,
Litrownik AJ, et al. Effect of early childhood
adversity on child health. Arch Pediatr Adolesc Med.
2006;160:1232-8.
27. Lannen P, Ziswiler M.
Potential and perils of the early years: The need to
integrate violence prevention and early child
development (ECD+). Aggression Violent Beh. 2014;19:
625-8.
28. United Nation Children’s Fund
(UNICEF). Programme guidance for early childhood
development. 2017 Accessed April 05, 2020. Available
from: https://www.unicef.org/early
childhood/files/FINAL_ECD_Programme_Guidance._
September._2017.pdf
29. Enhancing child protection
through early childhood care and development | Plan
International. Accessed April 12, 2020. Available
from:
https://plan-international.org/publications/enhancing-child-protection-through-early-childhood-care-and-development
30. Save the Children. Early
Childhood Care and Development (ECCD) Various
Modalities of Delivering Early Cognitive Stimulation
Programs for 0-6 year olds. 2016. Accessed March 24,
2020. Available from: https://resourcecentre.save
thechildren.net/node/10016/pdf/alt._eccd_models_
final_0. pdf
31. Prinz RJ, Sanders MR, Shapiro
CJ, Whitaker DJ, Lutzker JR. Population-based
prevention of child maltreatment: The U.S. triple P
system population trial. Prev Sci. 2009;10:1-12.
32. MacMillan HL, Wathen CN,
Barlow J, Fergusson DM, Leventhal JM, Taussig HN.
Interventions to prevent child maltreatment and
associated impairment. Lancet. 2009;373:250-66.
33. Mikton C. Two challenges to
importing evidence-based child maltreatment
prevention programs developed in high-income
countries to low- and middle-income countries:
Generali-zability and affordability. 2012. Accessed
August 15, 2020. Available from:
https://uwe-repository.worktribe.com/output
/954731/two-challengesto-importing-evidence-based-child-maltreatment-prevention-programs-developed-in-high-income-countries-to-low-and-middle-income-countries-generalizability-and-affordability
34. Skeen S, Tomlinson M. A
public health approach to preventing child abuse in
low- and middle-income countries: A call for action.
Int J Psychol. 2013;48:108-16.
35. Puffer ES, Green EP, Chase
RM, et al. Parents make the difference: a
randomized-controlled trial of a parenting
intervention in Liberia. Glob Ment Heal. 2015;2:e15.
36. Jeong J, Franchett E,
Yousafzai AK. World Health Organization
Recommendations on Caregiving Inter-ventions to
Support Early Child Development in the First Three
Years of Life: Report of the Systematic Review of
Evidence. 2018. Accessed August 25, 2020. Available
from: https://www.who. int/maternal_child_adolescent/guidelines/SR_Caregivin_
interventions_ECD_Jeong_Final_05Mar2020_rev.pdf? ua=1
37. Fenton A. Using a Strengths
Approach to Early Childhood Teacher Preparation in
Child Protection using Work-Integrated Education.
Asia-Pacific J Coop Educ. 2013; 14: 3:157-69.
38. Kapil U. Integrated Child
Development Services (ICDS) scheme/ : A program for
holistic development of children in India. Indian J
Pediatr. 2002;69:597-601.
39. Child Related Legislation |
Ministry of Women & Child Development | Government
of India. Juvenile Justice (Care and Protection Of
Children) Act, 2015 [Internet]. Accessed September
14, 2020. Available from:
https://wcd.nic.in/acts/
juvenile-justice-care-and-protection-children-act-2015
40. Protection of The Protection
of Children from Sexual Offences Act, 2012
[Internet]. Ministry of Women & Child Development,
Government of India. Accessed April 2, 2020.
Available from: https://wcd.nic.in/act/2315
41. Dubowitz H. Pediatrician’s
role in preventing child maltreatment. Pediatr Clin
North Am. 1990;37:989-1002.
42. Keeshin BR, Dubowitz H. Childhood neglect:
The role of the paediatrician. Paediatr Child
Health. 2013;18:e39-43.
|
|
|
 |
|
