|
|
|
Indian Pediatr 2021;58:548-552 |
 |
Effect of a Home Safety
Supervisory Program on Occurrence of Childhood Injuries: A
Cluster Randomized Controlled Trial
|
|
Anice George, 1 Renu G,2
Sheela Shetty1
From 1Manipal College of Nursing, Manipal Academy of Higher Education
(MAHE), Manipal, Karnataka; 2Crescent College of Nursing, Kannur,
Kerala.
Correspondence to: Dr Anice George, Dean, Manipal College of Nursing,
MAHE, Manipal, Karnataka, India.
Email:
[email protected]
Received: July 10, 2020;
Initial review: September 22, 2020;
Accepted: February 16, 2021.
Published online: February 19, 2021;
PII: S097475591600294
Trial registration: CTRI/2018/04/019386
|
Objectives: To evaluate the effect of home safety
supervisory program on improvement in childhood safety, self-reported
home hazard of caregivers, and caregivers’ supervisory attitude.
Design: Randomized controlled trial.
Setting and Subject: Caregivers of children
between 2 to 5 years of age residing in selected villages in Karnataka.
Intervention: Intervention group was administered
Home safety supervisory program (HSSP), whereas the control group
received teaching on child care.
Results: The intervention group had a significant
reduction in the frequency of childhood injuries when compared with the
control group [MD (95% CI) 8.96 vs 3.37], after the administration of
Home safety supervisory program. There was a significant difference in
the mean baseline scores of caregivers self-reported home hazard
practices between the two groups (P<0.001), and improvement in
the supervisory attitudes of caregivers in the intervention group (P<0.001).
Conclusion: Appropriate and effective home hazard
reduction teaching reduces home injuries in children. The improved
awareness of caregivers in child safety, and child supervision
emphasizes the importance of this program.
Keywords: Adult supervision, Home hazard, Injuries, Prevention.
|
|
I
njuries at home
constitute a significant number of
childhood injuries, as children spend longer period
of time in the home and also due to the many
hazards that may be present [1,2]. The common injuries for
younger children typically occurring at home are burns [3],
falls [4] and poisoning [2,3,5,6].
Children those who are left unsupervised or
inadequately supervised may come across with physical, mental,
or social negative outcomes [7,8]. Lack of super-vision has been
associated with unintentional childhood injuries ranging from
minor to ones with fatal severity. In cases of inadequate
supervision, multiple factors interact with each other to either
increase or decrease the risk of injury among children [8,9].
In India, unintentional injuries which are
preventable, is a major public health problem that
disproportionately affects children. The data on childhood
injury in the hos-pital and emergency departments are very
poorly main-tained and the broader portion of iceberg of issues
is not reported [10].
Unintentional injuries in children are a
combined and interrelated product of human behavior, environment
and other demographic factors. We planned to develop and
implement an intervention and evaluate the effect of a home
safety supervisory program (HSSP) on caregivers of children
below 5 years of age, on childhood super-visory practices.
METHODS
After clearance from the institutional
ethical committee, a cluster randomized controlled trial was
conducted to assess the effectiveness of HSSP in 10 villages in
Udupi district, Karnataka.
Cluster randomization technique was used,
wherein villages were considered as clusters and houses in the
village as cluster units. A random allocation was carried out at
the level of selection of villages to the intervention and
control group. Individual houses or selection of cluster units
were done by an external person who was not involved in the
study. Selection of the villages was done using probability
proportional to size. In EPI methodo-logy, which is
carried out after creating a cumulative list of community
population and selecting systematic sample of clusters with a
random start [11]. After identifying the villages, a
randomization process was done to select the villages to the
experimental and control group. This was done using tossing of
coin. The villages were randomized into intervention group (5
cluster) and control group (5 cluster). From each cluster, 13
cluster units (houses) consisting of children between the age
group of 2 to 5 years were selected. Home safety supervisory
program was administered to intervention group cluster and the
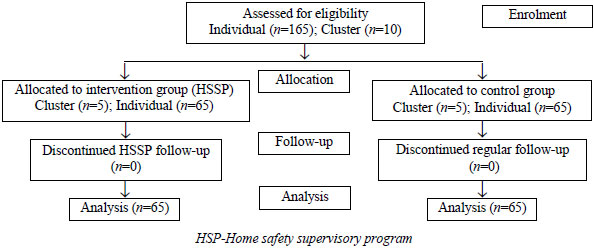
control group received teaching on child care. Fig. 1
shows the consort flow chart of participant selection.
 |
|
Fig. 1 CONSORT flow chart of the
study.
|
The sample size in the RCT is based on
comparison of means which was calculated on the basis of pilot
study finding. A total of 130 families were included in the
study (65 each in intervention and control group) who met the
following inclusion criteria: Houses consisting of at least one
child belonging to the age group of 2 to 5 years, care-givers’
of children (2 to 5 years) who can read, write and understand
English or Kannada (local language) and care-givers’ who care
for the children for at least 6-8 hours a day.
A demographic proforma was used to collect
basic information about the child and caregiver, age and gender
of the child, birth order, and type of family. Risk behavior
assessment questionnaire is a self-prepared 20-item
questionnaire to collect information from the caregivers
regarding events of injury in the past three months among their
children.
A home hazard assessment self-report
questionnaire was in the local language used to assess the
presence of home injury hazards as reported by caregivers during
a personal interview. This questionnaire was prepared by the
researcher and established validity and reliability. It
consisted of 27 items categorized under following areas: burns,
cut/injury, fall, drowning, suffocation/chocking and poisoning.
A higher score indicates more hazards at home that can cause
injury to the child. Observed home hazard (OHH) inventory was
used by the researcher to personally observe the home hazards in
the house which was researcher developed instrument based on the
practices in the local area. Caregiver supervisory attitudes
(CSA) is a five-point Likert scale 25-item questionnaire to
assess the caregiver’s child supervision practices. All the
instruments underwent validity and reliability studies. The
tools were later translated to local language and retranslation
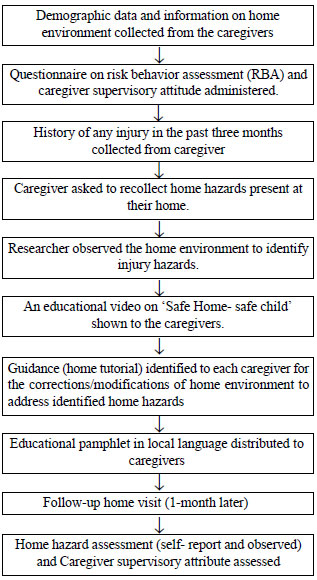
was done to make sure the accuracy. The schematic representation
of the study is shown in Fig. 2.
 |
|
Fig. 2 Schematic representation of the study
description.
|
The home safety supervisory program for
caregivers (HSSP) is the intervention developed for
caregivers of children aged 2 to 5 years in intervention group.
The program consisted of a video on ‘Safe home; Safe child,’ a
poster on ‘Safe home; Safe child’ and an individual home visit.
Health teaching on care of children between 2 to 5 years of age
was administered to the caregivers in the control group. The
contents of the health teaching included nutritional needs,
hygienic needs, safety needs and normal growth and development.
RESULTS
The sociodemographic characteristics of 130
enrolled children depicts that most (41.6%) of the children in
intervention group were in the age group of 3 to <4 whereas
43.1% of children in the control group belonged to 2 to <3 years
of age. Most of the children were first born in both the
intervention and control groups (53.8% and 49.2%, respectively).
In both the groups, the number of siblings for the indexed child
was 1 to 3 (52.3% in intervention and 58.4% in control group).
Table I shows the baseline characteristics of the
children. Table II shows the distribution of childhood
injuries in previous three months (baseline) and during one
month follow-up in both the groups.
Table I Baseline Sociodemographic Characteristics of Children and Caregivers in the Two Groups
| Variables |
Intervention group |
Control group |
| (n=65) |
(n=65) |
|
| Age (y)a |
3.3 (0.89) |
3.3 (0.97) |
| Male |
36 (55) |
31 (47) |
| Nuclear family |
42 (64) |
47 (72) |
| Caregiver mother |
52 (80) |
50 (76) |
| Caregiver age (y)a |
33.5 (10.5) |
34.2 (11.3) |
| Values no. (%) or amean
(SD). |
The children in the intervention group showed
a significant reduction in the injury pattern when compared with
those that of control group (P=0.02). A significant
change was observed in the mean scores of home safety practices
of caregivers in the intervention group whereas only minimal
change was seen in the mean scores of home safety practices of
caregivers in the control group. A significant difference in the
mean follow-up scores of caregivers self-reported home hazard
practices between the intervention and control group was noted.
At the same time, no significant difference was found in the
mean baseline and follow-up comparison of control groups.
The intervention with HSSP was an effective
method to reduce the home hazard practices as reported by the
caregivers as the mean difference observed from the baseline to
follow-up in the intervention group (6.48) was higher as
compared to that in the control group (0.18). A significant
improvement was found in the mean difference of caregivers’
supervisory attitude scores within the intervention group from
baseline to follow-up. At the same time, no significant
difference was found in the mean baseline and follow-up
comparison of control groups.
DISCUSSION
Many published studies reported that the
majority of injures occurs for children between the age of one
to four years [12,13]. In this study the mean age of children
experiencing home injuries was 3.3 years.
Interventions for caregivers are very
effective in reducing the injuries among children [14]. There
are two different strategies in interventions. They are active
and passive. One of the active strategy is training [15-16].
Injuries among children at home can be maximally reduced by
giving training or education for caregivers [17]. The results of
the present study revealed that such an intervention had a
significant reduction in the overall injury status of children.
An educational program in combination with
the distribution of a barrier or playpen was found to have a
significant decrease in burns injury among children post
intervention [18]. There is evidence that caregiver super-vision
may reduce the risk and severity of childhood injuries [19] and
protect children who have injury risk factors [9].
An educational intervention was found to have
improved the home safety practices of families with young
children with significant increase in the percentage of homes
deemed ‘safe’ after the fall intervention counseling [16,20].
The findings of a systematic review reported that parenting
interventions, provided within the home using multi-faceted
interventions may be effective in reducing child injury [21,22].
As the injury history in the study was
collected retrospectively, there might be varations while
reporting by the caregivers. There could be observer bias in the
present study as the observed home hazard safety practices was
assessed by the researcher.
The external validity of the study can be
improved by increasing the sample size and representation of
sample. A follow up of one year will make sure the retention of
practices.
The intervention in the study aimed at
increasing the caregivers awareness about home injuries and
various home safety practices, which inturn contributes to the
overall health and wellbeing of the children. Further the study
emphasizes that the intervention should be directed towards the
caregivers to have the change in the behaviour of children and
themselves and also to improve the home environment.
Surveillance of childhood injury and caregiver awareness would
help to bring down the unintentional injuries among children.
Ethics clearance: Institutional Ethics
Committee of Kasturba Medical College and Kasturba Hospital,
Manipal; No. IEC193/2018, dated March, 2018.
Contributors: AG: concept and design
development, data collection, writing the first draft and
consecutive revisions of the manuscript; RG: concept and design
development, development of the instruments, preparation and
consecutive revisions of the manuscript; SS: data collection,
data analysis and preparation and consecutive revisions of the
manuscript. All authors approved the final version of
manuscript, and are accountable for all aspects related to the
study.
Funding: Indian Council for Medical
Research (ICMR), New Delhi; Competing interest: None
stated.
| |
|
WHAT IS ALREADY KNOWN?
•
Children below five years are prone for injury. They
spend maximum time at home. Caregivers are responsible
for the supervision of children.
WHAT THIS STUDY ADDS?
•
The present study evaluated the effectiveness of a
home supervisory program. This study also identified the
attitudes of caregivers after the intervention.
|
REFERENCES
1. Mahalakshmy T, Dongre AR, Kalaiselvan G.
Epidemio-logy of childhood injuries in rural Puducherry, South
India. Indian J Pediatr. 2011;78:821-5.
2. Zia N, Khan UR, Razzak JA, Puvanachandra
P, Hyder AA. Understanding unintentional childhood home
injuries: Pilot surveillance data from Karachi, Pakistan. BMC
Reseach Notes. 2012;5:37.
3. Theurer WM, Bhavsar AK. Prevention of
unintentional childhood injury. American Family Physician.
2013;87: 502-9.
4. Jagnoor J, Bassani DG, Keay L, et al.
Unintentional injury deaths among children younger than 5 years
of age in India: A nationally representative study. Injury
Prevent. 2011;17: 151-5.
5. Sznajder M, Janvrin MP, Albonico V, et al.
Evaluation of the effectiveness of an injury prevention kit
delivery for toddlers in four French cities. Archives de
Pediatrie. 2003; 10:510-6.
6. Rai A, Khalil S, Batra P, et al.
Electrical injuries in urban children in New Delhi. Pediatric
Emerg Care. 2013;29: 342-5.
7. Aizer A. Home alone: Supervision after
school and child behavior. J Public Econ. 2004;88:1835-48.
8. Morrongiello BA, Pickett W, Berg RL, et
al. Adult super-vision and pediatric injuries in the
agricultural worksite. Accident Anal Preven. 2008;40:1149-56.
9. Schwebel DC, Brezausek CM, Ramey SL, Ramey
CT. Interactions between child behavior patterns and parenting:
implications for children’s unintentional injury risk. J Pediatr
Psychol. 2004;29:93-104.
10. Renu G, George A. Childhood injury an
iceberg of pheno-menon. IOSR J Dental and Medical Sciences.
2014;13:18-23.
11. Renu G, Kamath A. Community household
survey using EPI cluster sampling style. Indian J Public Health
Res Dev. 2020;10:590-4.
12. Kypri K, Chalmers DJ, Langley JD, Wright
CS. Child injury morbidity in New Zealand, 1987-1996. J Paediatr
Child Hlth. 2001;37:227-34.
13. Kypri K, Chalmers, DJ, Langley JD, Wright
CS. Child injury mortality in New Zealand 1986-95. J Paediat
Child Hlth. 2000;36:431-9.
14. Abbassinia M BM, Afshari M. Effectiveness
of inter-ventions in the prevention of home injuries among
children under 5 years of age: A systematic review. Arch Trauma
Res. 2019;8:190-97.
15. Simpson JC, Nicholls J. Preventing
unintentional child-hood injury at home: Injury circumstances
and inter-ventions. Int J Injury Control Safety Prom.
2012;19:141-51.
16. King WJ, Klassen TP, LeBlanc J, et al.
The effectiveness of a home visit to prevent childhood injury.
Pediatrics. 2001; 108:382-8.
17. Morrongiello BA CM, Brison RJ.
Identifying predictors of medically-attended injuries to young
children: do child or parent behavioural attributes matter?
Injury Prevention. 2009;15:220-5.
18. Jetten P, Chamania S, van Tulder M.
Evaluation of a community-based prevention program for domestic
burns of young children in India. Burns. 2011;37:139-44.
19. Schwebel DC, Brezausek CM. Chronic
maternal depre-ssion and children’s injury risk. J Pediatr
Psychol. 2008;33:1108-16.
20. Rehmani R, Leblanc JC. Home visits reduce
the number of hazards for childhood home injuries in Karachi,
Pakistan: A randomized controlled trial. Intern J Emer Med.
2010; 3:333-9.
21. Kendrick D, Barlow J, Hampshire A,
Stewart-Brown S, Polnay L. Parenting interventions and the
prevention of unintentional injuries in childhood: Systematic
review and meta-analysis. Child Care Hlth Dev. 2008;34:682-95.
22. Barbara A. Morrongiello SH, Melissa Bell, et al. Super-vising
for home safety program: A randomized controlled trial (RCT)
testing community-based group delivery. J Pediatric Psychol.
2017;42:768-78.
|
|
|
 |
|
