|
|
|
Indian Pediatr 2021;58:537-541 |
 |
Effectiveness of
School-Based Interventions in Reducing Unintentional Childhood
Injuries: A Cluster Randomized Trial
|
|
Ramesh Holla 1, BB Darshan1,
Bhaskaran Unnikrishnan1,
Nithin Kumar1, Anju Sinha2,
Rekha Thapar1,
P Prasanna Mithra1, Vaman
Kulkarni1, Archana Ganapathy1,
Himani Kotian1
From Departments of 1Community Medicine, Kasturba Medical College,
Mangalore (Manipal Academy of Higher Education), Karnataka; and
2Division of Reproductive, Maternal and Child Health, Indian Council of
Medical Research, Ansari Nagar, New Delhi.
Correspondence to: Dr Ramesh Holla, Associate Professor, Department
of Community Medicine, Kasturba Medical College, Mangalore (Manipal
Academy of Higher Education), Karnataka, India.
Email:
[email protected]
Received: November 09, 2020;
Initial review: December 15, 2020;
Accepted: February 04, 2021
Published online:
February 19, 2021;
PII: S097475591600292
Trial registration: CTRI/2018/02/011765
|
Objective: To evaluate the effectiveness of
school-based interventions in promoting child safety and reducing
unintentional childhood injuries.
Methods: This cluster randomized trial with 1:1
allocation of clusters to intervention and control arm was conducted in
the public and private schools of Dakshina Kannada district, Karnataka,
over a period of 10 months. Study participants included children from
standard 5-7 in schools selected for the study. 10 schools that
could accommodate 1100 students each, were randomly allocated to the
interventional and control arm. A comprehensive child safety and
injury prevention module was developed based on the opinions of school
teachers through focus group discussions. This module was periodically
taught to the students of intervention arm by the teachers. The children
in control arm did not receive any intervention. Outcome was assessed by
determining the incidence of unintentional injuries and type of injuries
from the questionnaire used at the baseline, and at the end of three,
six, and ten months.
Results: Unintentional injuries declined
progressively from baseline until the end of the study in both the
interventional arm (from 52.9% to 2.5%) and control arm (from 44.7% to
32%) [AOR (95% CI) 0.458 (0.405-0.518); P value <0.001]. The
decline in incidence of injuries in the interventional arm was higher
than that in the control arm (50.4% vs 12.7%; P <0.001).
Conclusion: School based educational intervention
using child safety and injury prevention modules is effective in
reducing unintentional injuries among school children over a 10-month
period.
Keywords : Education, Fall, Prevention, School health.
|
|
U nintentional injuries
specifically cause up to
950,000 deaths among children under 18
years annually [1] and more than half of
these deaths are reported from Sub-Saharan Africa and South Asia
[2]. Aside from mortality, accidental injuries can also lead to
long-lasting emotional, physical, behavioral and developmental
disabilities in children, which in turn could adversely affect
the health and socio economic aspects of a nation [3].
Prevention of injuries has been classified
into three strata of primary, secondary and tertiary prevention,
as per a model suggested by World Health Organization [4]. The
above-suggested WHO model can be incorporated while designing an
effective school-based injury-prevention program. This can be
used to address the policies and procedures, capacity building
of school teachers, the physical environment of the school, and
the curriculum in a coordinated manner.
There is little existing evidence to prove
that educational interventions alone are sufficient in reducing
the incidence of unintentional injuries [5]. Further studies are
required to evaluate the impact of school-based interventions on
injury occurrence as current studies only show a weak
association between the two [5]. Thus, this study was conducted
to evaluate the effectiveness of school-based interventions in
promoting child safety and reducing unintentional injuries.
METHODS
The study was conducted in the public and
private schools of Dakshina Kannada district, Karnataka, over a
period of 10 months from July, 2017 to March, 2018. It was a
cluster randomized trial with 1:1 allocation of clusters into
intervention arm and control arm, where schools are considered
as clusters. After excluding schools based on their willingness
to participate and existing participation in any child safety
and injury prevention program, randomization of schools was done
to accommodate 10 schools in the intervention arm and 10 schools
in the control arm by simple random method. Due representation
was provided to both public and private schools in both arms.
The study participants included 1100 children from standard 5-7
in the schools selected for the study. We assumed there
would be 40 students in each section of these standards. By
enrolling all the students of a particular section, we would be
enrolling 120 students from each cluster for the study.
Selection of a section for a particular class was done by
adopting simple random technique.
The sample size for the study was calculated
by considering a prevalence of 23% childhood injuries as per a
previous study [6]. The proposed intervention was considered
effective if it reduced the incidence of injury to 15%. Hence,
to account for the 8% reduction as significant at 90% power, 5%
level of significance and at two-sided test, the sample size was
calculated to be 503 in each arm. As it was a cluster-randomized
trial, we presumed a design effect of 2 and the sample size was
1006. As we anticipated a maximum of 10% loss during the
follow-up period of 10 months; the final sample size was
calculated to be 1107 in each arm.
A comprehensive child safety and injury
prevention module was then developed based on the opinions of
school teachers from both urban and rural settings through focus
group discussions. Later, subject experts validated the contents
of the module. This comprehensive pictorial module consisted of
child safety and measures to be taken by the children for the
prevention of unintentional childhood injuries due to road
traffic accidents, fall, burns, drowning, poisoning, animal
related and other domestic causes.
Two teachers (including one physical
training/sports teacher) from each school of the interventional
arm were trained using this module. The teachers then taught the
children on a periodic and regular basis for the duration of the
study, using an instruction manual for modular teaching (25-30
hours on an average was spent per school). The students in the
control arm received the comprehensive modular training after
the end of the final data collection. While imparting this
modular training, emphasis was given for child safety and injury
prevention strategies to be inculcated by the children.
The tool used for data collection was a
semi-structured questionnaire developed based on World Health
Organization guidelines for conducting community surveys on
injuries and violence [7]. This captured the incidence of
unintentional injuries and the type of injuries among
schoolchildren of both arms in the preceding three months. The
same questionnaire was administered for both the groups at
baseline, and at three, six, and ten months of the study.
Outcome was assessed by the same set of investigators at each
point of time in both intervention and control arm students.
Clearance was obtained from the institutional
ethics committee and permission was taken from the Block
Education Office. Due clearance was also obtained from the
school principals where the study was conducted. As the study
participants were children younger than 18 years, a written
informed consent was obtained from their parents before
enrolment into the study. Assent from the students were also
obtained. Confidentiality and anonymity was maintained
throughout the study.
Statistical analysis: All the data
collected in the field were managed at the central coordinating
site. The variables were coded and entered into Statistical
Package for Social Sciences Version 25.0 (IBM Corp). Descriptive
statistics and inferential statistics (Z test for difference in
two proportions, and generalized estimation equations (GEE) was
used to test the overall effectiveness of the inter-vention
across the groups with time) were used to express the results.
P<0.05 was considered statistically significant.
RESULTS
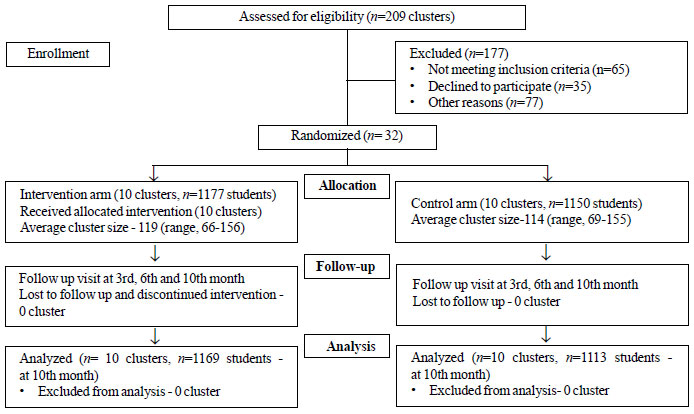
Out of 2327 children who were enrolled into
the study at baseline, 1177 children were in the interventional
arm and 1150 were in the control arm (Fig. 1). The
baseline data is provided in Table I.
 |
|
Fig. 1 Flow diagram of the
study.
|
Table I Baseline Characteristics of Study Participants (N=2327)
| Characteristics |
Intervention group |
Control group |
|
(n=1177) |
(n= 1150) |
| Male sex |
658 (55.9) |
500 (43.5) |
| Class |
|
|
| 5th |
367 (31.2) |
362 (31.5) |
| 6th |
306 (26.0) |
501 (43.5) |
| 7th |
504 (42.8) |
287 (25.0) |
| Urban locality |
656 (55.7) |
314 (27.3) |
| Government school |
507 (43.1) |
408 (35.5) |
| Values in no.(%). |
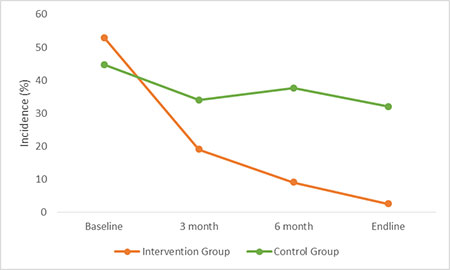
Incidence of unintentional childhood injuries
among schoolchildren of interventional and control group during
the study period is shown in Table II. Nearly half of the
study participants of the intervention (52.9%) and control
(44.7%) group had injuries in the preceding 3 months at the
baseline. The incidence of injuries declined progressively from
baseline until the end of the study among children in both the
groups [Adjusted OR (95% CI) 0.46 (0.40-0.52; P <0.001] (Fig.
2).
Table II Incidence of Unintentional Childhood Injuries
| Unintentional injury |
Intervention group |
Control group |
| Baseline |
623 (52.9) |
514 (44.7) |
| 3 mo |
224 /1179 (19.0) |
382/1123 (34.0) |
| 6 mo |
107/1184 (9.0) |
442/1175 (37.6) |
| End line |
29/1169 (2.5) |
356/1113 (32.0) |
| Incidence based on
generalized estimating equations (GEEs). Values in n/N
(%). Adjusted OR (95% CI)=0.45 (0.40-0.52), P<0.001. |
 |
|
Fig. 2 Trends in incidence of unintentional
childhood injuries over 10 months.
|
The extent of decline in incidence of
injuries from the start of the study till the end in the
interventional arm was higher than in the control arm (50.4% vs
12.7%; P<0.001).
Various causes of unintentional childhood
injuries across both groups throughout the duration of the study
is depicted in Suppl. Table I. Fall was the most common
cause of injury among children of interventional (56.8%) and
control group (46.7%) at baseline. Decline in the incidence of
unintentional injuries was observed in both the groups across
all categories.
DISCUSSION
We found that the incidence of unintentional
injuries among students in both the control arm and
interventional arm decreased compared to baseline incidence.
However, the extent of decrease was much greater in the
inter-ventional arm. While comparing incidences in both groups
across specific categories, the number of children who sustained
injuries from road traffic accidents, falls and others decreased
to a larger extent in the interventional group compared to the
control group with the biggest reduction noted in falls.
A randomized pre-test and post-test
comparative design study, ‘Think First for Kids’ [8] conducted
among grade 1, 2 and 3 students, evaluated the outcome of an
injury prevention program. The results of this study showed that
students in the interventional group had lesser self-reported
high-risk behaviors, and increased knowledge about ‘safe’
behaviors to avoid injuries as compared to students in the
control arm. In another study in rural China [9], a multi-level
educational interventional model (open letter about security
instruction distributed to parents, children’s injury-avoidance
poster put up at schools, and multimedia resource-aids for
health education) improved knowledge and safety attitudes among
students in the intervention arm as compared to the control arm.
It is interesting to note that the incidence
of unintentional injuries decreased among children in the
control group as well. We hypothesize that this could be due to
a combination of various factors. This includes the learning
curve of the child after experiencing an unintentional injury
and knowledge gained over time from other sources such as
parents or public health awareness campaigns.
From our study we also noted that the biggest
reduction in unintentional injuries was in the category of falls
among children in the interventional arm. The educational module
imparted knowledge on safe behaviors at home and while playing
outdoors. There were pictorial representations of scenarios
which most-likely lead to falls such as playing on escalator and
climbing trees. Another study by Morrongiello and Matheis [10]
used a similar educational intervention and it was shown to
reduce falls, particularly in the playground, through the
‘practice what you preach’ project. Children had less
risk-taking behavior and more safe practices after the
intervention.
Unintentional injuries due to road traffic
accidents also considerably reduced in the interventional group
as compared to the control group. Pictorial representations of
Dos and Don’ts related to Road safety was used to educate
children every week. Another public school based educational
intervention to improve attitudes, increase knowledge and change
unsafe road practices was implemented in four schools in Mexico
among 219 children and teenagers [11]. A significant improvement
in the attitude, practices and knowledge of involved students
were seen. The number of students suffering from burns decreased
significantly in the interventional group while it remained
constant in the control group, showing the effectiveness of the
educational module in this area. A cluster randomized controlled
trial evaluating an injury prevention program "Risk Watch’ in 20
primary schools among 459 children aged 7-10 years in
Nottingham, UK showed similar results [12]. At the end of this
one-year injury prevention program, it was effective in
increasing few aspects of children’s knowledge of fire and burn
prevention skills, although it had little effect on
self-reported safety behaviors, unlike our study.
The main limitation of our study is that it
is a single centric study and had a short duration of follow-up.
The results obtained regarding the prevention of unintentional
injuries among children using educational interventions cannot
be extrapolated until further multi-centric studies show the
same results. As this school based intervention using child
safety and injury prevention module was found to be effective in
reducing the incidence of unintentional injuries; this modular
intervention can be considered for incorporating it in the
school curriculum, after obtaining evidence from well-planned
multi-centric studies incorpo-rating a longer follow-up.
To conclude, the school based educational
inter-ventions using the child safety and injury prevention
module have significantly reduced the incidence of unintentional
injuries among children in the intervention arm when compared to
students of control arm where such educational interventions
were not given.
Acknowledgements: Mr. Laxminarayana
Acharya and Ms. Mamatha, Medical Social Workers and Ms. Shika J,
Data Entry Operator for successful completion of the project.
Note: Supplementary material related to
this study is available with the online version at
www.indianpediatrics.net
Ethics clearance: Institutional
Ethics Committee of Kasturba Medical College, Mangalore; No. IEC
KMC MLR 12-14/285, dated 17 December, 2014.
Contributors: RH, DB: Concept and design,
analysis, inter-pretation of data, drafting the article; BUK:
Concept and design, interpretation of data, drafting the
article, revising it critically; VK, NK: Interpretation of data,
revising it critically for important intellectual content; RT,
PM: Study design, interpretation of data, revising it critically
for important intellectual content; AS: Revising the manuscript
critically for important intellectual content and critical
interpretation of the data captured; AG: Analysis of the data,
drafting the manuscript and proof reading; HK: Data analysis and
critical revision of the results. All authors approved the final
version of manuscript, and are accountable for all aspects
related to the study.
Funding: Indian Council of Medical Research;
Competing interests: None stated.
|
WHAT THIS STUDY ADDS?
• A school-based educational intervention is
effective in reducing the incidence of unintentional
childhood injuries among school children.
|
REFERENCES
1. Orton E, Whitehead J, Mhizha-Murira J, et
al. School-based education programmes for the prevention of
unintentional injuries in children and young people. Cochrane
Database Syst Rev. 2016;12:CD010246.
2. Mahapatra T. Public health perspectives on
childhood injuries around the world: A Commentary. Ann Trop Med
Public Health 2015;8:233-4.
3. Sinha AP, Sarma S, Kamal R, Gupta P,
Amritanshu. Prevention of unintentional childhood injuries in
India: An Indian Council of Medical Research (ICMR) initiative.
EC Paediatrics. 2020;9:143-48.
4. Barcelos RS, Del-Ponte B, Santos IS.
Interventions to reduce accidents in childhood: a systematic
review. J Pediatr (Rio J). 2018;94:351-67.
5. Centers for Disease Control and
Prevention. School Health Guidelines to Prevent Unintentional
Injuries and Violence. MMWR Recomm Rep. 2001;50:1-73.
6. Mahalakshmy T, Dongre AR, Kalaiselvan G.
Epidemio-logy of childhood injuries in rural Puducherry, South
India. Indian J Pediatr. 2011;78:821-5.
7. Seth D, editor. Guidelines for Conducting
Community Surveys on Injuries and Violence. World Health
Orga-nization. Available from:
https://apps.who.int/iris/handle/10665/42975
8. Gresham LS, Zirkle DL, Tolchin S, Jones C,
Maroufi A, Miranda J. Partnering for injury prevention:
evaluation of a curriculum-based intervention program among
elementary school children. J Pediatr Nurs. 2001;16:79-87.
9. Cao BL, Shi XQ, Qi YH, et al. Effect of a
multi-level education intervention model on knowledge and
attitudes of accidental injuries in rural children in Zunyi,
Southwest China. Int J Environ Res Public Health. 2015;12:
3903-14.
10. Morrongiello BA, Mark L. Practice what
you preach: Induced hypocrisy as an intervention strategy to
reduce children’s intentions to risk take on playgrounds. J
Pediatr Psychol. 2008;33:1117-28.
11. Treviño-Siller S, Pacheco-Magaña LE,
Bonilla-Fernández P, et al. An educational intervention in road
safety among children and teenagers in Mexico. Traffic Inj Prev.
2017;18:164-170.
12. Kendrick D, Groom L, Stewart J, et al.
Risk watch: Cluster randomised controlled trial evaluating an
injury prevention program. Inj Prev. 2007;13:93-8.
|
|
|
 |
|
