In this prospective cohort study, data
were collected from various hospitals voluntarily enrolled
in the NNF COVID-19 registry, which was initiated in April,
2020. Neonates born to women with SARS-CoV-2 infection
within two weeks prior to or two days after delivery and
neonates with confirmed SARS-CoV-2 infection within 28 days
of life were eligible for enrolment in the study. COVID
status of mothers and neonates was assessed by
nasopharyngeal RT-PCR in all participating hospitals.
SARS-CoV-2 infected neonates were defined
as those with a positive SARS-CoV-2 quantitative RT-PCR test
in nasopharyngeal swab within 28 days of birth [5].
SARS-CoV-2 infected mothers were defined as
those with a positive SARS-CoV-2 quantitative RT-PCR test in
the nasopharyngeal sample during the peripartum period [5]. Perinatal transmission was defined as
positive naso-pharyngeal RT-PCR in a neonate in the first 72
hours after birth [6,7]. This included intrauterine and
intrapartum transmission. Testing was avoided in the first
12 hours to minimize false positives due to superficial
colonization. Horizontal transmission was considered in a
neonate with negative RT-PCR within the first 72 hours who
sub-sequently tested positive any time after 72 hours of
birth irrespective of the mother’s SARS-CoV-2 status [6,7].
Mothers were either tested at admission
or referred for admission because of the SARS-CoV-2 positive
reports. Testing and management were as per the Indian
Council for Medical Research (ICMR) and NNF guide-lines, and
local standard operating procedures [8,9]. SARS-CoV-2 status
of the neonate was tested as per NNF guidelines and local
institutional protocols, which in most centres was done
within the first 72 hours after birth or when the neonate
was symptomatic and admitted to the neonatal unit [8]. All
neonates were monitored for clinical symptoms for the first
seven days after birth and for as long as the mother was
admitted to the hospital. Data on mothers and neonates was
available till disposition from the hospital.
Data collection: Data was
prospectively submitted to the registry by the participating
hospitals in a web-based secure platform (https://innc.org/covid).
All the registered hospitals received a short message alert
every week on the number of enrolled cases and data
complete-ness. Twenty percent of the enrolled cases from
each participating centre were randomly cross-checked for
data quality. A closed group of clinical leads from
partici-pating hospitals was formalized for secure,
encrypted communication. This group managed the updates to
the database, day-to-day problems in data management, the
progress of the registry, and sharing of education and
communication. Any inconsistency in data was high-lighted to
the respective hospital lead for verification.
The data included baseline
characteristics of the mothers, mode of delivery, type of
feeding, rooming-in with mother or isolation from mother,
clinical features, diagnosis, and neonatal outcomes. The
clinical status of patients was classified as per guidelines
from the Ministry of Health and Family Welfare, Government
of India [10].
Statistical analyses: Descriptive
statistics were used, and comparisons were made using the
chi-square test for categorical variables and the Student
t-test or Mann-Whitney U test as appropriate for continuous
variables.
A P-value of <0.05 was considered significant.
The web-based COVID-19 registry received
a total of 1733 entries for mothers and their neonates.
Almost all (1730/1733) of the enrolled mother-infant dyads
were from tertiary care hospitals, 1649 (95%) from public
sector hospitals, and 82 (5%) from private hospitals. We
excluded 22 entries where both mothers and neonates were
negative but were referred because of suspicion of
SARS-CoV-2 infection, and 1711 mother-infant dyads were
enrolled in this study. Most of the mothers (94.5%) were
asymptomatic, and only 1% were critically ill. Cesarean
section was the mode of delivery in 68%.
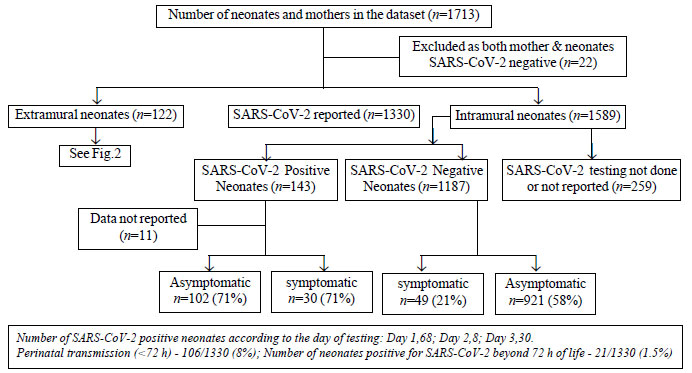
Of the 1711 enrolled neonates, 1589 were
intramural, while 122 were extramural births. The extramural
infants were referred to the participating hospitals for
either symptomatic status or for SARS-CoV-2 positive status
of the mother. Figure 1 gives a study flow for intramural
neonates enrolled in the registry. Out of 1589 intramural
infants, SARS-CoV-2 testing was either not done or not
reported in 259, so we excluded them from the analysis.
Amongst 1330 tested neonates, 143 (10.8%) were SARS-CoV-2
positive. Of these, 68 (5.1%) tested positive on day one (Fig.
1 and 2). Amongst the intramural newborn infants,
106 (8%) were positive for SARS-CoV-2 within 72 hours
(perinatal transmission) and 21 (1.5%) beyond 72 hours
(horizontal transmission) of birth. The risk of transmission
was not associated with the mode of delivery or type of
feeding. The risk of transmission of SARS-CoV-2 from mother
to neonate was marginally higher if the baby was roomed-in
with the mother (RR 1.16, 95% CI 1.1-2.4; P=0.01).
Tables I and II compare the SARS-CoV-2 positive
and negative infants born to SARS-CoV-2 positive mothers.
The demographic para-meters in both the groups were not
different except for the prematurity rate, which was higher
in SARS-CoV-2 positive group. SARS-CoV-2 positive neonates
were five times more likely to be symptomatic and twice more
likely to need resuscitation. They had significantly higher
probability of having sepsis and septic shock. SARS-CoV-2
positive neonates were more likely to have abnormal
radiological findings and need respiratory support. They
were also more likely to have received surfactant, steroids
and inotropes. The risk of mortality was however not
significantly different between the two groups. No
significant association was noted between mother’s
symptomatic status and baby’s SARS-CoV-2 positivity, need
for resuscitation, and symptoms.
| Parameters |
|
SARS-CoV-2 |
RR (95% CI) |
|
Positive |
Negative |
|
|
(n=39) |
(n=65) |
|
| Symptomatic |
13/27 (48) |
6/36 (16.6) |
2.9 (1.2-6.6)d |
| RDS |
13 (33.3) |
8 (12.2) |
2.7 (1.2-5.9)c |
| Pneumonia |
6 (15.4) |
1 (1.5) |
10.1 (1.2- 81)c |
| Seizures |
4 (10.2) |
1 (1.5) |
6.6 (0.7-57)d |
| Septic Shock |
6 (15.4) |
1 (1.5) |
10 (1.2-80)d |
| DIC |
3 (7.7) |
0 |
12.1 (0.6-229)e |
| Encephalopathy |
1 (2.6) |
1 (1.5) |
1.6 (0.1-25.8)e |
| Diarrhoea |
2 (5.1) |
2 (3.1) |
1.6 (0.2-11.3)e |
| Other morbidities |
11 (28) |
2 (3.1) |
9.1 (2.1-39)b |
| Abnormal CXR |
16 (11.2) |
7 (0.6) |
18.9 (7.9- 45.3)a |
| Oxygen therapy |
10 (25.6) |
4 (6.1) |
4.1 (1.4-12.3)c |
| CPAP |
3 (7.7) |
3 (4.6) |
1.7 (0.3-8.2)e |
| Ventilation |
7 (17.9) |
1 (1.5) |
11.6 (1.5-91)c |
| Inotropes |
5 (12.8) |
1 (1.5) |
7.7 (0.9-64)e |
| Corticosteroids |
2 (5.1) |
0 |
8.2 (0.4-167)e |
| IVIG |
2 (5.1) |
0 |
8.2 (0.4-167)e |
| Mortality |
1 (2.6) |
1 (1.5) |
1.6 (0.1-25.8)e |
| CXR: chest X-ray;
IVIG: intravenous immunoglobulin; CPAP: continuous
positive airway pressure; RDS: respiratory distress
syndrome; DIC: disseminated intravascular
coagulation. aP<0.001; bP=0.001; cP<0.01; dP<0.05;
eNot significant. |
There were 17 neonates in the registry,
who were positive for SARS-CoV-2, but their mothers were
reported negative. Five of these neonates were positive
within 72 hours of life, and the remaining tested positive
beyond 72 hours of birth. In this sub-group, 3 (17.6%)
needed resuscitation at birth, 3 (17.6%) had pneumonia, 5
(29%) had respiratory distress, and 4 (23.5%) had sepsis.
One (5.9%) infant had encephalopathy, and 3 (17.6%) had
seizures.
DISCUSSION
In this large registry of neonates born
to SARS-CoV-2 positive mothers, we report the incidence of
neonatal infection, type of symptoms, and neonatal outcomes.
Neonates acquired infection most commonly in the first 72 h
after birth. The 5.1% neonates who tested positive on day
one may have acquired the infection intrauterine or
intrapartum. Those neonates who tested positive on days two
or three may also have been due to intrauterine transmission
but could have acquired the infection postnatally from
mother, other family members, or healthcare providers. In
the absence of serial testing and testing of various body
fluids from mother, it is not possible to pinpoint the
timing of acquisition. It is also to be noted that many
neonates were tested for the first time on day three as per
the local protocols, and the absence of testing on the first
day after birth could have led to misclassification of the
type of infection. We found a significantly higher incidence
of perinatal transmission than that reported in a recent
review [10].
This study highlights that SARS-CoV-2
positive neonates are more likely to be symptomatic, more
likely to have respiratory symptoms, and other neonatal
morbidities. However, the mortality is not increased
significantly. In a systematic review by Raschetti, et al.
[4], the median age at diagnosis was five days, and 55% of
neonates were symptomatic [4]. Common symptoms reported
include respiratory distress, fever, and those related to
gastrointestinal illness. Most of the infected neonates were
not reported to need any respiratory support and had a good
outcome after a median duration of hospitalization of 10
days. In our study cohort, 21% (30/143) of SARS-CoV-2
positive intramural neonates were symptomatic, and the most
common symptoms included respiratory distress and
sepsis-like features. However, fever and gastrointestinal
symptoms were not commonly reported. The prematurity rate of
20.7% in our cohort was significant and similar to what was
reported by the UK registry [11]. This raises concerns about
the possibility of increased risk of premature labor in
SARS-CoV-2 positive pregnant women. The incidence of
symptomatic infection reported by us is lower than that
reported in the previous reviews [4,12-13] and an Indian
case series [14], but similar to that reported by Anand, et
al. [15]. This can be explained by possible selection bias
inherent in the type of studies - case reports and case
series- included in the systematic reviews.
Another important finding in our cohort
is that SARS-CoV-2 infected neonates were significantly more
likely to need resuscitation, be symptomatic, need NICU
admi-ssion, have abnormal chest X-rays, and need
respiratory support. Previous studies have reported a high
incidence of NICU admissions in SARS-CoV-2 positive neonates
or neonates born to SARS-CoV-2 infected mothers [4]. Some of
the variations in NICU admission rates may be due to local
protocols for admission and isolation rather than due to the
illness per se. Prematurity is an obvious confounder for
higher respiratory and other morbidities in the SARS-CoV-2
positive group, and we did not adjust for prematurity rates.
However, the difference in prematurity rates is unlikely to
explain the magnitude of differences in morbidities.
We found a marginally higher incidence of
infection in neonates who were roomed-in with mother.
However, we did not find any association with breastfeeding.
Similar findings have been reported by Raschetti, et al.
[4], wherein
lack of mother–neonate separation from birth was associated
with late SARS-CoV-2 infections, while breastfeeding was not
associated with increased risk. Recent systematic reviews
have found a very low rate of detection of SARS-CoV-2 RNA in
breastmilk, with a much higher prevalence of antibodies to
the virus in the breastmilk [16,17]. The World Health
Organization recommends that neonates should be roomed-in
with mother and exclusively breastfed while following
pre-cautions to limit the spread of SARS-CoV-2 infection to
neonates [18]. A higher incidence of neonatal infection in
infants roomed-in with mothers is likely due to incomplete
adherence to the suggested precautions. Salvatore, et al.
found no perinatal transmission in a cohort of 116
SARS-CoV-2 positive pregnant women from three New York
hospitals with rooming-in and breastfeeding, if correct
hygine precautions, maternal masking and parental education
were undertaken [19]. Similarly, Anand, et al. [15] report a
low risk of transmission of infection from mother to baby
with rooming-in and breastfeeding. This is important
information for families to be aware of, along with the
finding that infection is asymptomatic in the majority of
neonates, and the outcome is largely favorable.
Mean-while, more research is needed to evaluate measures to
prevent postnatal transmission to neonates and improve
adherence to currently prescribed precautions.
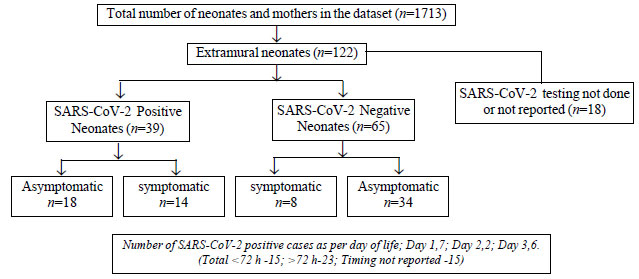
We also report on extramural neonates
referred to tertiary care hospitals following contact with
an infected adult in the family or for other morbidities.
SARS-CoV-2 positivity was more likely if these neonates were
sympto-matic at admission. The repertoire of symptoms was
similar to symptomatic intramural neonates. The high
incidence of infection in neonates who are symptomatic at
presentation underscores the need for universal testing
guidelines for this category of neonates [20].
This large registry was created for the
new COVID-19 disease within a short span of time after the
WHO’s announcement of the pandemic and data was contributed
by 20 hospitals on a voluntary basis across the country. The
most important limitation, as highlighted above, was
non-uniformity in age at testing of neonates born to
SARS-CoV-2 positive mothers. As this was a registry-based
study, testing of other biological sources like amniotic
fluid, placenta, blood, or breastmilk was not pursued. We
also did not test for the presence of specific antibodies in
the neonatal blood to look for intrauterine infection as
suggested by a recent guideline to classify the type of
neonatal infection [7].
We did not capture data for neonates with the
possibility of multi-system inflam-matory syndrome in
children (MIS-C) following SARS-CoV-2 infection, which is
recently being reported [21].
In conclusion, our study provides
important data on neonatal infection, clinical features, and
outcomes in neonates born to SARS-CoV-2 positive women. This
information can be used to make informed decisions and
policies on neonatal SARS-CoV-2 testing, healthcare
organization for neonates born to SARS-CoV-2 positive women,
and counseling of families regarding various management
options.
Acknowledgements: Bodhgire
Sachin and Aradhana Mishra, Government Medical College,
Aurangabad, Maharashtra; Tanmay Sar and Bilkish Islam,
Nil Ratan Sircar Medical College, Kolkata, West Bengal;
Vivek Kumar and Dhirendra Prasad Yadav, Department of
Pediatrics, All India Institute of Medical Sciences, New
Delhi; Md Zakiulla and Purbasha Mishra, All India
Institute of Medical Sciences, Bhubaneswar, Odisha.
Contributors: KM: initiated and wrote
the proposal for the registry and created a data collection
form, analyzed the data, and finalized the first draft of
the manuscript; BT, SM and PK: facilitated the creation of
the data registry on web-portal hosted by the Indian
Neonatal Collaborative (INCC), India; BT: coordinated data
collection and helped to extract relevant data from the
portal; SM: wrote the introduction and methods sections,
helped in biostatistics and approved the final draft of the
manuscript; DC: reviewed the analysis, results section and
wrote an interpretation of data and discussion; AD: approved
the proposal, encouraged and coordinated hospitals’
participation through National Neonatology Forum, India and
reviewed the final draft of the manuscript; PK: approved the
proposal, created a registry on the portal, encouraged
hospitals’ participation and approved the final draft of the
manuscript. All the remaining Collaborators contributed
significantly towards data collection and sharing from their
respective institutes, and also reviewed and approved the
final draft of the manuscript.
Funding: None; Competing interest:
None stated.
ANNEXURE
Members of the National Neonatology Forum
(NNF) COVID-19 Registry Group
Writing Group
Kiran More, Sidra Medicine Hospital,
Doha, Qatar; Deepak Chawla, Government Medical
College, Chandigarh; Srinivas Murki, Paramitha
Children Hospital, Hyderabad, Telangana; Baswaraj Tandur,
Princess Durru Shehvar Children’s and General Hospital;
Ashok K Deorari, All India Institute of Medical Sciences,
New Delhi; Praveen Kumar, Postgraduate Institute of
Medical Education and Research, Chandigarh.
Investigators
Suchitra Dontamala, Gandhi Hospital
and Medical College, Hyderabad, Telangana;
Mangalabharathi Sundaram, Institute of Obstetrics and
Gynecology, Madras Medical College, Chennai, Tamilnadu;
M Anitha, Chengalpattu Medical College and Hospital,
Chengalpattu, Tamilnadu; Deshmukh Laxmikant,
Government Medical College, Aurangabad, Maharashtra;
Asim Kumar Mallick, Nilratan Sircar Medical College and
Hospital, Kolkata, West Bengal; Jagjit Singh Dalal,
Pt. B.D. Sharma Postgraduate Institute of Medical Sciences,
Rohtak, Haryana; Ankit Verma, Department of
Pediatrics, All India Institute of Medical Sciences, New
Delhi; Vinay Kumar R, SNR Hospital, Kolar, Karnataka;
Shilpa Kalane, Deenanath Mangeshkar Hospital, Pune,
Maharashtra; Ratan K Das, IMS and SUM Hospital,
Bhubaneswar, Odisha; Tapas Kumar Som, All India
Institute of Medical Sciences, Bhubaneswar, Odisha;
Somosri Ray, Medical College and Hospital, Kolkata, West
Bengal; Manish Mittal, Cocoon Hospital, Jaipur,
Rajasthan; Ashish Mehta, Arpan Newborn care Centre,
Ahmedabad, Gujarat; Chandra Kumar Natarajan, Kanchi
Kamakoti Childs Trust Hospital, Chennai, Tamilnadu;
Abhishek Aradhya, Ovum Woman and Child Specialty
Hospital, Hoskote, Karnataka; Niraj Patel, Shree
Navajivan Children Hospital, Rajkot, Gujarat.
Co-Investigators
JN George and Srikanth Sandanala,
Gandhi Medical College and hospital, Hyderabad, Telangana;
Mohammed Sajjid and Vijaya Subramanian, Institute of
Obstetrics and Gynecology, Madras Medical College, Chennai;
Manikumar S, Chengal-pattu Medical College and Hospitals,
Chengalpattu, Tamil Nadu; Debasis Maity, Nil Ratan
Sircar Medical College, Kolkata, West Bengal; Sandeep
Jhajra Dayanand, Pt. BD Sharma Postgraduate Institute of
Medical Sciences, Rohtak; Balasundar, Nodal Officer,
SNR Hospital, Kolar, Karnataka; Rajan V Joshi,
Department of Paediatrics, Deenanath Mangeshkar Hospital,
Pune, Maharashtra; Pankaj Kumar Mohanty and Tanushree
Sahoo, All India Institute of Medical Sciences,
Bhubaneswar, Odisha; Dinesh Munian, Medical College
and Hospital, Kolkata, West Bengal; Binoy Shah, Arpan
Newborn care Centre, Ahmedabad, Gujarat; Vaanathi
Vijayakumar, Kanchi Kamakoti Childs Trust Hospital,
Chennai, Tamil Nadu.
|
WHAT IS Already KNOWN?
• Limited
evidence exists on the perinatal transmission and
the management of severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) infection among newborns,
especially from the developing world.
WHAT THIS STUDY ADDS?
•
Our data confirms
perinatal transmission of SARS-CoV-2 and suggests
increased morbidity in infected infants.
Breastfeeding and rooming-in seem to be safe but
require compliance with additional precautions.
|
REFERENCES
1. COVID19 India. Accessed 20 April,
2021. Available at https://www.mohfw.gov.in/
2. Guan WJ, Ni ZY, Hu Y, et al. Clinical
characteristics of coronavirus disease 2019 in China. N Engl
J Med. 2020; 382:1708-720.
3. Fox NS, Melka S. COVID-19 in pregnant
women: Case series from one large New York city obstetrical
practice. Am J Perinatol. 2020;37:1002-04.
4. Raschetti R, Vivanti AJ,
Vauloup-Fellous C, et al. Synthesis and systematic review of
reported neonatal SARS-CoV-2 infections. Nature
Communications. 2020;11: 5164.
5. Sheth S, Shah N, Bhandari V. Outcomes
in COVID-19 positive neonates and possibility of viral
vertical trans-mission: A narrative review. Am J Perinatol.
2020;37: 1208-16.
6. Blumberg DA, Underwood MA, Hedriana
HL, et al. Vertical Transmission of SARS-CoV-2: What is the
Optimal Definition? Am J Perinatol. 2020;37:769-72.
7. Shah PS, Diambomba Y, Acharya G, et
al. Classification system and case definition for SARS-CoV-2
infection in pregnant women, fetuses, and neonates. Acta
Obstet Gynecol Scand. 2020;99:565-68.
8. Chawla D, Chirla D, Dalwai S, et al.
Perinatal-Neonatal Management of COVID-19 Infection -
Guidelines of the Federation of Obstetric and Gynaecological
Societies of India (FOGSI), National Neonatology Forum of
India (NNF), and Indian Academy of Pediatrics (IAP). Indian
Pediatr. 2020;57:536-48.
9. Ministry of Health and Family Welfare.
Guidelines for Management of COVID-19. Accessed January 05,
2021. Available at https://www.mohfw.gov.in
10. Dhir SK, Kumar J,Meena J, Kumar P.
Clinical features and outcome of SARS-CoV-2 infection in
neonates: A systematic review. J Trop Pediatr. 2020 Aug 28:
fmaa059.
11. Gale C, Quigley MA, Placzek A, et al.
Characteristics and outcomes of neonatal SARS-cov-2
infection in the UK: A prospective national cohort study
using active surveillance. Lancet Child Adolesc Health.
2021;5:113-121.
12. Kotlyar AM, Grechukhina O, Chen A, et
al. Vertical transmission of coronavirus disease 2019: A
systematic review and meta-analysis. Am J Obstet Gynecol.
2021; 224: 35-53.
13. Walker KF, O’Donoghue K, Grace N, et
al. Maternal transmission of SARS-COV-2 to the neonate, and
possible routes for such transmission: A systematic review
and critical analysis. BJOG. 2020;127:1324-36.
14. Nanavati R, Mascarenhas D, Goyal M,
et al. A single-center observational study on clinical
features and outcomes of 21 SARS-cov-2-infected neonates
from India. Eur J Pediatr. 2021;1-12.
15. Anand P, Yadav A, Debata P, et al.
Clinical profile, viral load, management and outcome of
neonates born to COVID 19 positive mothers: A tertiary care
centre experience from India. Eur J Pediatr.
2021;180:547-59.
16. Kumar J, Meena J, Yadav A, et al.
SARS-CoV-2 detection in human milk: A systematic review. J
Matern Fetal Neonatal Med. 2021 Feb 8;1-8.
17. Zhu F, Zozaya C, Zhou Q, et al.
SARS-CoV-2 genome and antibodies in breastmilk : A
systematic review and meta-analysis. Arch Dis Child Fetal
Neonatal Ed. 2021 Feb 9; 0-F1-F8.
18. World Health Organization.
Breastfeeding and COVID-19. Scientific Brief. 23 June 2020.
Accessed December 25, 2020. Available at:
https://www.who.int/opublications/i/item/WHO-2019-nCoV-Sci_Brief-Breastfeeding-2020.1
19. Salvatore CM, Han JY, Acker
KP, et al. Neonatal manage-ment and outcomes during the
COVID-19 pan-demic: an observation cohort study. Lancet
Child Adolesc Health. 2020;4:721-27.
20. Sivanandan S, Chawla D, Kumar P,
Deorari AK, National Neonatology Forum India. COVID-19 in
neonates: A call for standardized testing. Indian Pediatr.
2020;57: 1166-71.
21. Nakra NA, Blumberg DA, Herrera-Guerra
A, et al. Multi-System Inflammatory syndrome in children
(MIS-C) following SARS-CoV-2 infection: Review of clinical
presentation, hypothetical pathogenesis, and proposed
management. Children (Basel). 2020;7:69.