|
|
Brief Reports Indian Pediatrics 2006;43:889-894 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Do the Length-based (Broselowâ) Tape, APLS, Argall and Nelson’s Formulae Accurately Estimate Weight of Indian Children? |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
A. Varghese, V.K. Vasudevan, S. Lewin, C.K. Indumathi, C. Dinakar and S.D. Subba Rao From the Department of Pediatrics, St. John’s
Medical College Hospital, Bangalore, Correspondence to: Dr. S.D. Subba Rao, Professor, Pediatrics, St. John’s Medical College Hospital, Bangalore, Karnataka 560 034, India. E-mail: [email protected] Manuscript received: May 31, 2005, Initial review
completed: July 28, 2005;
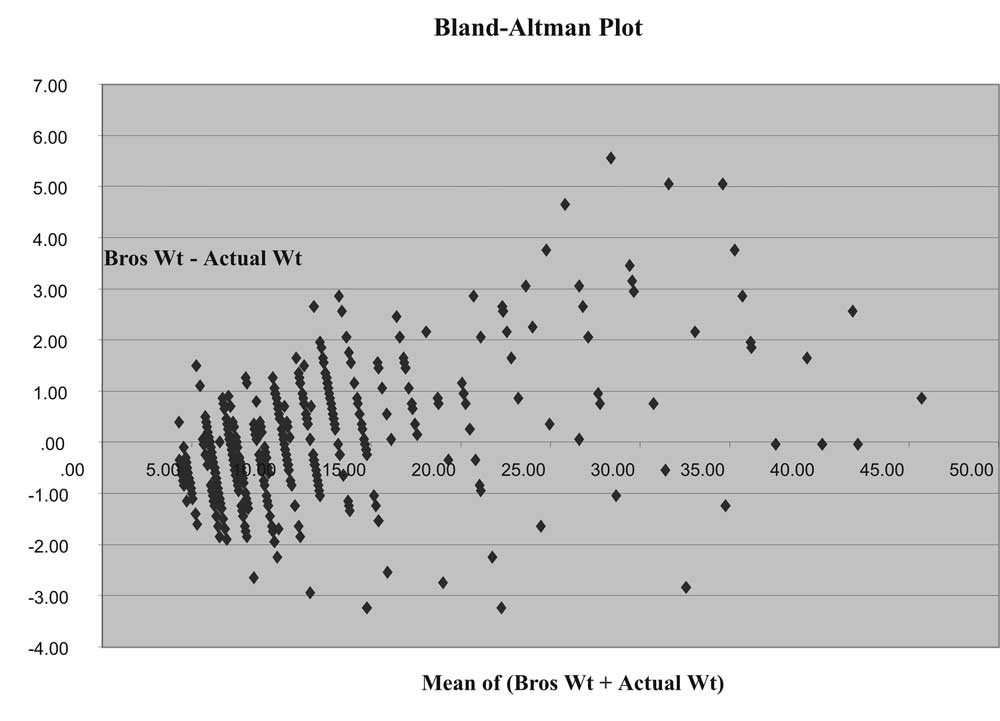
In pediatric emergencies, drug doses and intervention decisions are often based on estimated body weights(1,2). Inaccurate weight estimations may cause non-responsiveness or increased adverse events and toxicity to interventions(3). The measured weight of a child is considered the gold standard but it is often impractical to weigh the child in these situations. In emergency settings, there is an increased likelihood of error in estimating age-derived weights for children(4,5). Most use common age-dependent weight formulae [Nelson Textbook of Pediatrics (Nelson Formula)(6), Advanced Pediatric Life Support (APLS)(7) and Argall’s modification(8)]. These have been derived and validated in western pediatric population(9,10). It is a concern that these methods based on age probably overestimate weights of Indian children hence over-estimating doses. The Broselow® Tape (Broselow® Pediatric Emergency Tape, 2002 Edition A, Drs. James Broselow and Robert Luten, Armstrong Medical Industries, 575 Knightsbridge Parkway, Lincolnshire, IL 60069, USA) was developed using height/weight correlations from Western data. This validated tape estimates weight (hence intervention doses/sizes) of the supine child based on length(11,12). The tape has a series of color-coded zones (boxes) with details of all necessary doses and sizes for emergency interventions. One end of the tape has a red arrow and this end is placed at the head end of the supine child with the tape lying alongside the child. The foot end of the child indicates the colored box with printed out estimated doses/sizes of fluids, drugs and equipment. This eliminates memorization and mathematical errors and one can concentrate more on other emergency treatment. Though recommended in India(13), there are no Indian publications that have validated the Broselow® Tape in an Indian pediatric population. In addition, cost remains a stumbling block to its acceptability. The fact that this tape is length based and not dependent upon the age of the child makes it more likely to be valid for our pediatric population. The primary objective of this study was to validate the length-based (Broselow®) tape in our pediatric population. Secondary objectives include validation of other common age-based formulae (Nelson, APLS, Argall’s) and their accuracy in estimating weight and intervention doses/sizes for Indian children in an emergency. Subjects and Methods This was a cross-sectional hospital based study done on a sample of 500 children attending the pediatric outpatient department requiring non-emergency care. The sample was collected over a period of 6 months, from August 2003 to January 2004. The Institutional Ethics Review Board cleared the protocol and informed consent was taken from parents/legal guardians. The Unit team (SL, ICK, CD) was responsible for all children. Inclusion criteria were all children 1 mo to 12 yr age whose legal guardians consented to the study measurements (weight and height/length). Exclusion criteria included all children requiring emergency care, uncooperative, unstable and critically ill, length >145 cm or weight >35 kg (pre-requisites for using Broselow® Tape) and refusal of consent. Children needing acute care were excluded as we thought that time taken for obtaining informed consent and carrying out the measurements could be detrimental to immediate care. Sample size was calculated based on effect size of 0.2, beta of 0.2 and one-tailed alpha of 0.005 using the formula for a predicted ‘r’ of 0.15. During sampling, children were alternatively selected based on sex. Measurements of weights and lengths of children were to the nearest 0.1 kg and 0.1 cm respectively. This was by two trained and inter-observer validated investigators (AV, VKV). The same investigator did all measurements and estimates on a given child. Weights were taken first using an electronic weighing scale (IPA Devices) for those less than 20 kg and a lever scale (Avery India) for those greater than 20 kg. Length / height were measured using an infantometer (Tower Scales) and a standing scale (Avery India) respectively. Recumbent length was measured for children <2 yr and standing height for those equal or >2 yr. These measurements were compared to Broselow® Tape estimates. For each child, the tape’s color code system was noted for three chosen dosages and equipment sizes (adrenaline first bolus dose 0.1 mL/kg 1:10000; Fluid bolus 20 mL/kg; and, Endotracheal size in mm = 4 + Age (yr)/4). These three parameters were chosen since they represent the commonest interventions in resuscitation and represent a wide spectrum of potential errors. Following documentation of age, weights were also calculated using Nelson’s Formula [3-12 mo: (age in mo + 9)/2; 1-6 yr: age in yr × 2 + 8; 7-12 yr: (age in yr × 7-5) / 2]; APLS Method (1-10 yr): 2 × (age in yr + 4); and, Argall’s Modification: (2 + age in yr) × 3] (6-8). The adrenaline dose, fluid bolus and endotracheal size were calculated based on weights estimated by these three methods. The same parameters by Broselow Tape were documented. Estimates from all four were then compared with those derived from actual measured weights. A Pearson correlation between weights, adrenaline dose, fluid bolus and endotracheal tube size by all estimation methods and actual weight was followed by Bland-Altman Plots to determine the mean bias and standard deviations(8). For all measurements those calculated on actual weights were considered gold standards(8). Analysis was performed using SPSS statistical software with a P value <0.05 considered significant. Results Five hundred children were assessed and age ranged from 0.1 yr to 11.4 yr, with a mean of 1.39 and Standard deviation of 2.14. Majority of children (51%) were under 6 months, and only 7.8 % of children were above 5 years. The M: F ratio was 1:0.98. Weights ranged from 2.50-32.0 kg with a mean of 8.19 kg. Most children (N = 458) were <15 kg and in the age range of 0.1-6.7 yrs. The Pearson Correlation for each pair of data was tabulated. All differences were statistically significant (P <0.0001). Bland-Altman Plots compared differences between all methods. Good correlation was demonstrable only between actual weight measured and Broselow tape estimates (Fig. 1). Mean differences with standard deviation were tabulated (Table I).
TABLE I Mean Bias and 95% CI From Actual Weight and Measures of Adrenaline Dose, Fluid Bolus and Endotracheal Tube Size as Determined by Broselow Tape, Nelson, Argall’s and APLS Formulae
wt = weight; Adr = adrenaline; ET= endotracheal tube. Weight correlations It was clear from the magnitude of the correlation that the strength of the relationship between the Broselow® Tape and actual weights of Indian children (across all weights) is a near perfect positive correlation (r = 0.974) with a mean bias <0.04 kg. This correlation was also seen to a lesser degree with Argall’s modification, combined Nelson’s formulae and the APLS formulae. Argall and APLS methods overestimate weight by greater than 2-3 kg. Weight <15 kg, equal and >15 kg correlations: However, children <15 kg and equal and >15 kg as two separate study subgroups showed different relationships. Broselow Tape shows a good positive correlation for children weighing <15 kg and this correlation is marginally less perfect when children are equal or >15 kg. Broselow Tape has an overall minimal overestimation compared with actual weights (Mean differences 0.034 ± 1.185 kg). In the <15 kg group the mean difference is 0.080 ± 0.96. Nelson’s formulae for estimation of weight shows moderate to weak correlation when used for subgroups, 1-6 yr and 7-12 yr age and weighing equal to and >15 kg. In children <15 kg and <3-12 mo age, Nelson’s formulae reveal a moderate positive correlation (r = 0.603). Nelson’s formulae when studied in their subgroups do not correlate well with actual weights of Indian children. In the case of weight estimations, Bland-Altman Plots illustrated that APLS and Nelson’s formulae (1-6 yrs, 7-12 yrs) tended to overestimate weight with maximum discrepancy seen in the 7-12 yr Nelson formula (Mean difference 5.204 ± 4.272 kg). Adrenaline doses Broselow Tape remains the best method in estimation of Adrenaline bolus dose in <15 kg (Mean differences 0.009 ± 0.103 mL) and Nelson’s formula showed maximum difference in >15 kg (Mean difference 1.4 ± 1.71 mL). Fluid bolus Broselow compares well with fluids needed based on actual weight <15 kg (Mean difference 0.97 ± 20.4 mL). APLS and Argall tend to overestimate fluid bolus (Mean differences range from 30 to 53 mL ± 29-87 mL). Maximum overestimation occurred in Nelson formula for >15 kg (Mean difference 297.52 ± 343.05 mL). Endotracheal tube size The comparison was between the traditional age related formulae and a Broselow estimate. Broselow tended to underestimate endotracheal tube size by up to 0.5. Discussion Most methods to calculate estimated weight from age or height/length are based on western pediatric populations. Age-based weight estimation formulae were expected to overestimate weight in Indian children. Similar to studies in western populations (8,9,11), this study suggests that Broselow® Tape predicts actual weight most accurately in comparison with all other methods. However, there was a tendency for the loss of accuracy of estimation as the child’s weight increased, especially above 15 kg. A similar significantly decreasing accuracy trend has been previously documented using the Broselow® Tape, but in children greater than 25 kg(9). From the results it is evident that all formulae tend to overestimate the weight especially in the higher weight range (15 kg). In comparison British studies(8) on APLS and Broselow® Tape underestimate actual weight. Broselow tape was fairly accurate in the selection of ET, though it tended to slightly underestimate the size. European and US studies, in contrast, report it as being an accurate means to assess endotracheal tube size(11,12). A major limitation of the study to our mind is the skewing of the sample towards younger ages and weights with inadequate representation of children above 15 kg. In addition, lack of ready availability of Broselow® Tape in India and its relatively higher cost (around USD 55) may restrict its use. In conclusion, a Length-based Pediatric Emergency Tape (Broselow®) correlates well with an overall emergency intervention decision-making process in our setting. This is especially validated in the age group 0.1-6.7 yr weighing <15 kg. The Broselow® Tape estimates for Adrenaline, Fluid bolus and Endotracheal tube size in Indian children <6 years is validated and it shows less bias than usual age-based estimations currently in use. Larger numbers need to be studied to validate the same in the subpopulation >15 kg. Contributors: AV and VKV responsible for concept, design, acquisition of data. SL was involved in concept, design, analysis, interpretation, drafting and final approval. ICK and CD: Concept, design, training, inter-observer validation, drafting. SDSR: analysis, interpretation. All authors approved the final version. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()