|
|
Case Report Indian Pediatrics 2004; 41:1162-1164 |
|||||||||||||||||||||||||||||||||
S.M. Shinde
TABLE I Immunoglobin Level and CD4 & CD8 Values at Admission
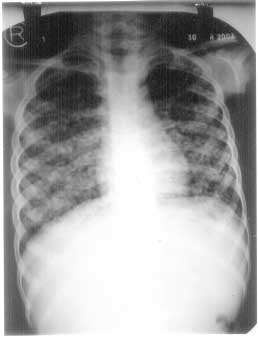
Discussion Cryptococcus grows in soil and in bird excreta especially of pigeons(4,5). Infection is acquired in most cases by inhalation of fungal spires(3). Cryptococcus neoformans has worldwide distribution and preferentially infects immunosuppressed hosts or patients with HIV infection(1). Prevalence data for India are not available, but in sub Saharan Africa 15-80% of all patients with AIDS develop cryptococcal infection(1). Most of the patients reported are adults, over the age of 40 years(6). As mentioned earlier it is rarely reported in children(5). However, none of the above reports pertain to the species Cryptococcus humicolus. In view of the miliary shadows on X-ray, dyspnea and hepatosplenomegaly our patient was first thought to have disseminated tuberculosis. Fungal culture was attempted because of no response to antitubercular therapy. To our surprise both blood and urine culture grew cryptococci. Liver biopsy, bone marrow biopsy and lymph node biopsy also showed significant number of cryptococci. The boy however, was negative for HIV on ELISA test. The treatment generally recommended for systemic cryptococcosis is amphotericin B with flucytosine(4,5,7,8). The lipid based amphotericin B is mostly preferred as it is said to be less nephrotoxic(7,8). However in view of financial constraints we used the cheaper non lipid based amphotericin B with fluconazole (flucytosine is not freely available in India)(9). We were worried initially, as response to therapy was poor and child continued to need intensive care support with oxygen and tube feeding for nearly 6 weeks. We were able to discharge him home (after 7 weeks of hospitalization) on fluconazole prophylaxis. Prior to the use of amphotericin B cryptococcal meningitis and disseminated disease were invariably fatal. However, with the availability of amphotericin B, flucytosine, fluconazole and other azoles, the mortality rate of cryptococcal disease has decreased upto 28% with various regimen(3). However, the cost and non availability of some of the drugs is a particular problem in our country. Acknowledgement Authors would like to thank Dr. Avinash Pradhan for interpreting the histology and Dr. Rama Manchanda for the hematological work up of the case. Grateful acknowledge-ment is also made to Dr. Sheila Bhave for her valuable help in drafting and editing the report. Contributors: SS drafted the report, carried out literature search and was the resident incharge of the patient. KV looked after the patient on day to day basis. AP decided the patient management and will act as guarantor. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||
|
|
![]()