|
Personal Practice Indian Pediatrics 2000;37: 504-514 |
||||||||||||
|
Scorpion Sting |
||||||||||||
|
S. Mahadevan
Scorpion sting is an acute life-threatening, time-limiting medical emergency of villagers(1). Reliable statistics are not readily available for this common rural accident. Numerous enveno-mations are unreported and true incidence is not known. Case fatality rates of 3-22% were reported among children hospitalized for scorpion stings in India, Saudi Arabia and South Africa(2-6). Among the 86 species of scorpions in India, Mesobuthus tamulus and Palamneus swammer-dami are of medical importance(7). Dominant clinical effects following the sting vary from species to species. Cardiovascular effects are particularly prominent following the stings by Indian red scorpion (Mesobuthus tamulus)(8). By elucidating the natural history of this condition, observant physicians like Bawaskar and Bawaskar set the stage for a rational therapy to follow. Their landmark study in rural Maharashtra reported first the effects of Prazosin in victims of scorpion sting(9). This article considers the pathophysiology, clinical picture and therapy of scorpion venom poisoning in children.
Scorpions live in warm dry regions throughout India. They inhabit commonly the crevices of dwellings, underground burrows, under logs or debris, paddy husk, sugarcane fields, coconut and banana plantations. Their distribution is more in regions with abundant red soil(10). Scorpions may be found outside their natural range of distribution when inadvertently transported with other items such as luggage. Scorpions retreat in the crevices of dwellings during the day only to emerge at night; thus most stings are reported at night. Scorpion stings increase dramatically in summer months and are lowest in winter. Scorpion stings are primarily due to accidental contact with scorpion. They use their stings only when roughly handled or trodded on. Scorpion does not always inject venom when it stings since it can control its ejacula-tion; thus the sting is total, partial or non-existent. Scorpions capable of inflicting fatal stings in humans are all members of families Buthus and Scorpionidae(7). Reports from Bellary, Rayalaseema, rural Maharashtra, Pondicherry and Chennai have documented such fatalities in children and adults (3,11,12).
Various reports on clinical effects, bio-chemistry of scorpion venom, extrapolation of animal studies to clinical setting, autopsy studies and therapeutic interventions have contributed to our understanding of scorpion envenomation.
Effect
of Venom on Ion Channels, Alpha Receptors and Myocardium Voltage dependant ion channels are altered by the venom. The side chains of scorpion venom are positively charged. This is important in their ability to bind to specific membrane channels. Alpha (of Buthus sp.) and beta (of Centruoides sp.) toxins act on sodium channel. Scyllatoxin, charybdotoxin of Leiurus species and Tityus toxin act primary on potassium channels(15,16). The toxin acts by opening sodium channel at presynaptic nerve terminals and inhibiting calcium dependant potassium channels. Autonomic storm is thus initiated. Alpha receptors stimulation by the toxin plays a major role, resulting in hypertension, tachycardia, myocardial dysfunction, pulmo-nary edema and cool extremities(17). Raised angiotensin I levels have also been documented which further facilitate the sympathetic outflow through conversion to angiotensin II(18). Excess catecholamines cause accumulation of endothelins and vasoconstriction. The unopposed effects of alpha receptors stimulation lead to suppression of insulin secretion, hyperglycemia, hyperkalemia, free fatty acids and free radicals accumulation injurious to myocardium. Cardiac sarcolemmal defects, depletion of glycogen content of heart, liver and skeletal muscles were observed in experimental animals with acute myocarditis produced by Indian red scorpion venom(19-22).
Effect
of Venom on Hemopoietic System, Brain and Lungs Some species of scorpion (Tityus discrepans) cause abundant microthrombi in rabbit lungs. It is suggested that these clotting alterations are fundamental to produce acute lung injury and increased alveolocapillary membrane permeability(26).
Effect
of Venom on Skin, Kidney, Liver and Pancreas
Scorpion
Venom and Systemic Inflammatory Response
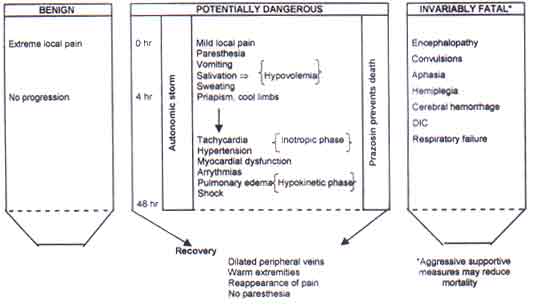
Species differences, venom dose/weight relationship determine the toxicity and clinical picture. Changes in body temperature may increase the sensitivity of venom and influence the course of toxicity(33). In India, Israel, Brazil and Mexico cardiac manifestations are common; in Iran tissue necrosis and hemolysis; in South Africa and USA neurological features and in Trinidad acute pancreatitis dominate the picture(5,6,8,34-39). Symptoms after scorpion sting progress to a maximal severity in about five hours and subside within a day or two. The evolution of clinical features seen in our context is depicted in Fig. 1.
Pain
Autonomic
Storm Tachycardia seen within 4 hours persist for 24-72 hours. Tachycardia, hypertension, myocardial dysfunction, pulmonary edema and shock is spectrum of one process viz., auto-nomic storm. They are not different syndromes. Vomiting and palmoplantar sweating precede development of myocardial injury. Marked tachycardia, S3 gallop and ice-cold extremities are seen in these children. Hypertension lasts for 4-8 hours in many due to outpouring of catecholamines from adrenal stimulation; it is prolonged in some due to direct stimulation of sympathetic centers in medulla. Hypertensive stress on myocardium, direct myocyte toxicity and catecholamines induced injury contribute to rhythm disturb-ances and LV failure in a significant proportion of children. Hypotension and bradycardia can be encountered within 1-2 hours of sting due to cholinergic stimulation; hypotension and tachycardia later (4-48 h) indicate severe LV dysfunction. During recovery stage (48-72 h) hypotension can be seen; but the extremities are warm with good volume pulse and child is otherwise well.This state, due to an exhausted catecholamine stores awaiting replenishment, requires no intervention with dopamine agonists. Fluid loss due to vomiting, salivation and perspiration complicate the clinical course and hemodynamic abnormalities in many children. Pulmonary edema may develop within 30 minutes to three hours after a sting due to myocardial dysfunction. Development of symptoms associated with pulmonary edema is variable but may be rapid. Tachypnea or intractable cough at admission could mean pulmonary edema in evolution. Close monitoring is indeed vital to detect and treat pulmonary edema. Children appear pale (‘ashen pallor of skin’) with clammy skin and have tachycardia with elevated blood pressure, retractions, nasal flaring and grunting. Pink frothy sputum as classically described in adults is not always present in children. Some children land into acute pulmonary edema while showing apparent signs of recovery. Death within 30 minutes in some of these children is due to ventricular arrythmias. Non-cardiac pulmonary edema due to ARDS is commonly reported from Brazil (Tityus serrulatus scorpion)(40). In majority of children changes in chest X-ray suggestive of pulmonary edema are seen even within 3 hours of sting. These children are not tachypneic surprisingly, though some of them become symptomatic in the next 6 hours. Normal cardiac silhouette with pulmonary vascular congestion, straight non-branching lines in upper lung field that run diagnolly towards hilum and horizontal non-branching lines in periphery of lower lung indicating inter-lobular septal edema are seen. Electrocardiographic changes frequently seen are peaked T waves in V2-6, ST segment elevation in leads I, aVL, increased QR duration (ventricular activation time) and LVH by votlage criteria. Low voltage complexes throughout the record and left anterior hemiblock indicate poor prognosis(8). Echocardiography reveals left ventricular systolic dysfunction in these children. Left ventricular dilatation with regional wall motion abnormalities are also seen infrequently(41). Central nervous system manifestations are infrequently encountered. They are however invariably fatal. Encephalopathy, convulsions within 1-2 hours of sting, acute rise in arterial blood pressure with rupture of unprotected perforating arteries, cerebral hemorrhage, stroke and central respiratory failure have been reported(42-25). This acute rise in BP needs rapid correction to prevent cerebrovascular accident. It has been documented that symptoms of methamphetamine toxicity mimicked scorpion envenomation in an infant(46). A high incidence of acute pancreatitis was reported from Trinidad and Israel following scorpion sting. The pain was colicky or continuous, lasted from 10 minutes to 24 hours and recovery was uneventful. Cases of acute edematous, hemorrhagic pancreatitis and pancreatic pseudocysts have been earlier described(28,47).
Prazosin–a competitive post-synaptic alpha1, adreno-receptor antagonist–should be the first line of management, since alpha receptors stimulation plays a major role in the evoluation of clinical spectrum(9,48). Prazosin suppresses sympathetic outflow and activates venom-inhibited potassium channels. It decreases the preload, afterload and blood pressure without increasing the heart rate. Prazosin counters vasoconstriction induced by endothelins through accumulation of cyclic GMP (cGMP). Prazosin by inhibiting phospho-diesterase enzyme and by inhibiting the formation of inositol triphosphate makes this possible. cGMP, a second messenger of nitric oxide in vascular endothelium (eNOS) and myocardium prevents further myocardial injury. The metabolic and hormonal effects of alpha receptors stimulation are reversed by prazosin. Thus prazosin is a cellular and pharmacologic antidote to the actions of scorpion venom and it is also cardioprotective. Prazosin is available as scored 1 mg tablet. Sustained release tablets are not recommended in this condition. The dose recommended is 30 microgram/kg/dose. This is given as an immediate measure in all with evidence of autonomic storm. It should not be given as prophylaxis in children when pain is the only symptom. In case of vomiting, it can be administered through nasogastric tube. After giving prazosin, mother should be advised not to lift the child to prevent the effects of ‘First dose phenomenon’ due to prazosin. Oral hydration and milk feeds must be encouraged. If needed, intravenous maintenance fluids should be given to correct dehydration due to excessive sweating and vomiting. Prazosin can be given irrespective of blood pressure provided there is no hypovolemia. Blood pressure, pulse rate and respiration must be monitored every 30 minutes for 3 hours, every hour for next 6 hours and later every 4 hours till improvement. Prazosin should be repeated in the same dose at the end of 3 hours according to clinical response and later every 6 hours till extremities are warm, dry and peripheral veins are visible easily. The time lapse between the sting and administration of prazosin for symptoms of autonomic storm determines the outcome(4,8,48). No more than four doses have been required in majority of children treated at our center. Benzodiazepines (Diazepam) is often useful to quieten a child restless after scorpion sting. Benzodiazepines in concert with GABA open chloride ion channel. This effect of diazepam antagonises the scorpion toxins’ ability to stimulate specific ion channel.
Pain
and Fluid Management The loss of fluid due to profuse sweating and vomiting is usually overlooked. So oral fluids whenever feasible must be encouraged. When children present with tachypnea and altered sensorium, parenteral fluids (N/5 saline) are required. Fluid requirements need to be balanced carefully. In children with pulmonary edema, CVP monitoring is essential. The use of a combination of insulin and alphablocker with NaHCO3 resulted in reversal of all electrocardiographic changes (rhythm disturbances, conduction defects, ischemia and infarction like pattern) to sinus rhythm in experimental animals(51). Bawaskar reported similar changes with oral prazosin in his patients(48).
Treatment
of Pulmonary Edema In children with pulmonary edema with or without hypertension, management should be directed towards relieving afterload without compromising preload. The use of diuretics to minimize or reduce fluid overload seems a reasonable measure but only when renal water excretion is impaired. Otherwise the best way to prevent fluid overload is to maintain an adequate cardiac output. Thus dobutamine support (5-15 mg/kg/min) with vasodilatation through sodium nitroprusside (0.3-5 mg/kg/min) or nitroglycerine (5 mg/min) infusate is preferred in this situation. Prazosin is to be given one hour before termination of sodium nitroprusside (SNP) drip. If SNP is not available, one can use isosorbide dinitrate 10 mg every 10 minutes sublingually as an emergency measure. Morphine, a standard therapy in pulmonary edema, should be avoided in scorpion sting, since narcotics worsen dysrythmias in these children. Occasionally, children with scorpion sting present with multi-organ failure. A systemic inflammatory response is presumably the cause; however our knowledge on the pathogenesis of such a state is still incomplete. Presence of respiratory failure with or without CNS disturbances in the presence of hypertension or complicating those children with pulmonary edema should be aggressively treated with early ventilation, afterload reduction, careful sedation and acid-base correction.
Scorpion
Antivenom
Unhelpful
Treatment
Children are more often stung by scorpion due to their exploratory nature. Presumably only the more serious cases reach us but we gain the impression that in children the mortality is quite high. It is believed that children are more likely to die than adults since they receive a toxic dose on toxin to weight scale. I am of the view that morbidity due to scorpion sting is high in children but outcome is good with low mortality because venom acts on healthy myocardium which recovers fast and tolerates well the autonomic storm. Even controlled animal studies indicate that adults rats were more susceptible to venom than young rats (LD50 of B. tamulus toxin 1.3 ± 0.4 vs 2.2 ± 0.24 mg/kg in young ones)(62). Deaths in children are more often due to irrational therapy or failure to monitor closely and treat effectively pulmonary edema. The usefulness of prazosin therapy in this condition was scientifically established in mid-eighties in India. The experimental evidence of Gueron confirmed the clinical experience of Bawaskar and Bawaskar (Personal communica-tion). It is however not clear as to why the use of prazosin was not put into practice at all centers. The reasons for this may be many viz., lack of awareness, or lack of published data from different settings. In the pre-prazosin era (1961-1983), 25-30% fatality due to pulmonary edema was reported in scorpion victims from Western India. Since the use of prazosin (1984 onwards) the mortality in these victims is reduced to less than 1%(1,8,48). Case fatality rate in children due to scorpion sting has declined from 13% to 3% at our center after prazosin was introduced as the first line of management(4). Clinical acceptance of prazosin for scorpion sting now exists. There must be no delay in administration of prazosin. Pediatricians should also not hesitate to treat pulmonary edema effectively with sodium nitroprusside or nitroglycerin infusate and dobutamine support wherever appropriate.
The following preventive measures can be considered:
There is now professional confidence for successful management of scorpion sting in India even without antivenom. Prazosin regimen–rational, scientific, cardioprotective, cheap, easily available and free from anaphylaxis should be the first line of treatment in scorpion sting. The time lapse between the sting and administration of prazosin for autonomic storm determines the outcome. Unhelpful treatment, often practised, should be avoided.
Contributor: SM reviewed the literature and drafted the paper.
|
![]()