|
|
Personal Practice Indian Pediatrics 2005; 42:559-568 |
||||||
|
Chest Physiotherapy in Pediatric Practice |
||||||
|
A. Balachandran
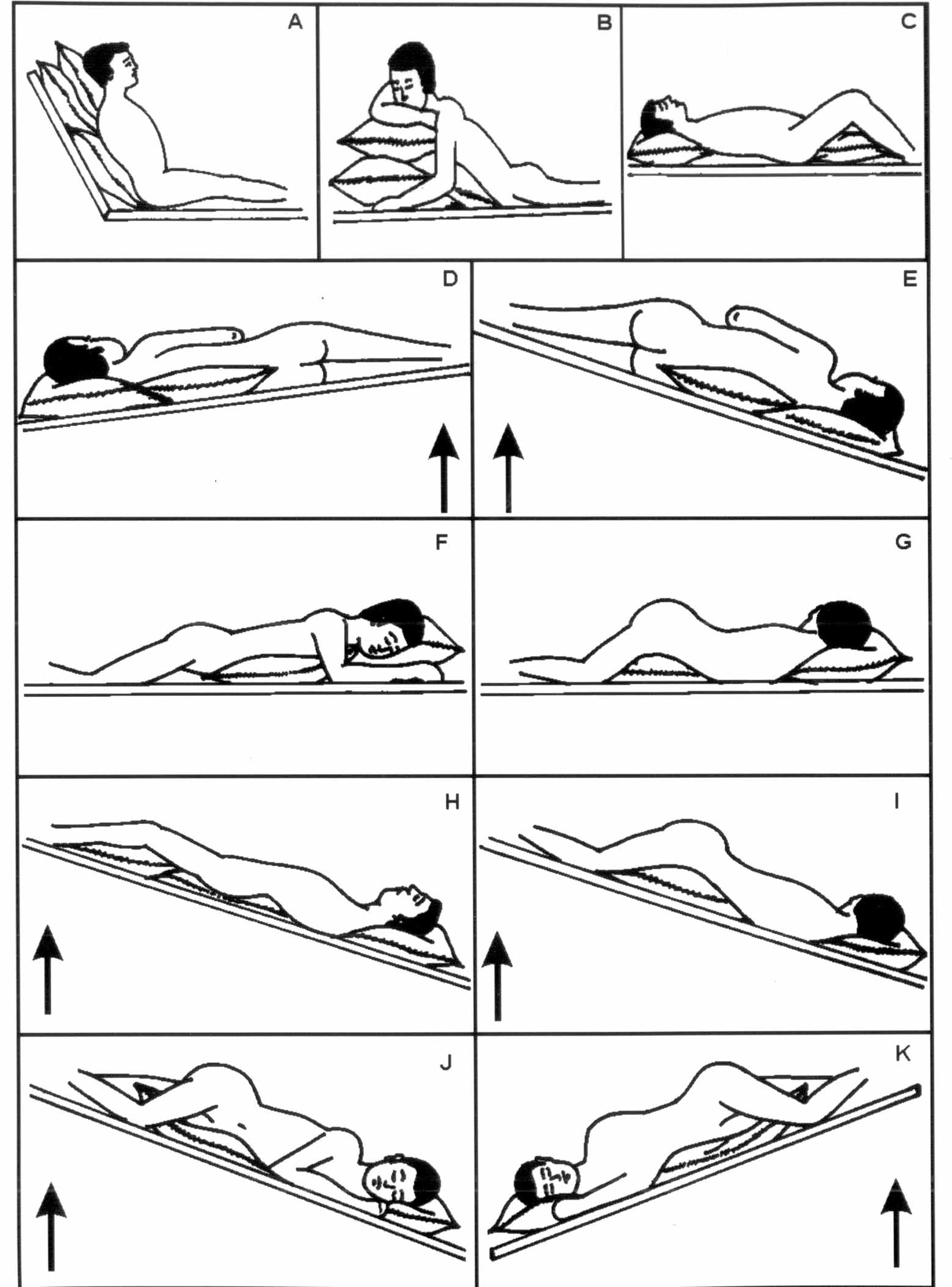
Respiratory ailments still remain a major cause of morbidity and mortality in developing countries. Chest physiotherapy is an important adjuvant in the treatment of most respiratory illnesses in children compared to adults. Even minor reduction in diameter of pediatric airway, especially in infants results in clinically significant reduction in the airway cross section, resulting in increase in airflow resistance and work of breathing(1). Definition Chest physiotherapy (CPT) is an airway clearance technique that combines manual percussion of the chest wall by the care- giver, strategic positioning of the patient for mucus drainage with cough and breathing techniques. It is useful for individuals with copious mucus or thick secretions, those with weak respiratory mechanics or those with ineffective cough. CPT consists of various manipulative procedures like positioning, chest percussion, vibration, thoracic squeezing and cough stimulation. Breathing exercise is an integral part of chest physiotherapy. It plays a significant role in airway clearance and parenchymal expansion by improving the efficiency of respiratory muscles. Surface Anatomy of Lungs A thorough knowledge of surface marking of the lobes and bronchopulmonary segments is essential for better understanding of chest physiotherapy. A line from the second thoracic spine to the sixth rib in the mammary line corresponds to the upper border of the lower lobe or the major interlobar fissure. On the right side a horizontal line from the sternum at the level of the fourth costal cartilage, drawn to meet the line of the major interlobar fissure marks the boundary between the upper and middle lobes or minor fissure(2). The greater part of the lung as seen from the back of the chest is composed of the lower lobe and only the apex comprises of the upper lobe. The middle and upper lobes on the right side and the upper lobe on the left are represented in front. Postural Drainage (Positioning) Normally the mucocilliary blanket and cough reflex effectively clears the inflammatory exudate in normal conditions but is deranged during infection. Postural drainage prevents the accumulation and enhances mobilization of bronchial secretion from the airway utilizing gravity to facilitate drainage. Postural drainage is mere positioning of the child with assistance of gravity to mobilize the secretions towards the main bronchus. Mere tilting of the thorax does not effectively clear the airway secretions, but if complemented by deep breathing, effective coughing, percussion and vibration techniques would loosen and dislodge these secretions. Rationale of Postural Drainage During erect position only the segments of the right upper lobe and non-lingular portion of the left upper lobe receive gravitational assistance whereas the segment of the middle, lingular portion of left upper lobe and lower lobe segments of both lungs must drain against gravity. In normal healthy state the adequate patency of the trachebronchial tree and the effective function of the mucociliary mechanism clear off the bronchial secretion inspite of these disadvantages. In diseased state they get compromised and secretions get accumulated especially in the smaller airways that cannot be emptied without gravity assistance. Principles of Postural Drainage In general, the upper lobe segments have the advantage of gravity drainage both in erect as well as in semi recumbent position, so postural drainage can be facilitated in sitting or lying posture. The middle and lower lobes do not have the advantage of gravity drainage in erect, semirecumbent or recumbent postures. So a 14 and 18 inches footend elevation are required for postural drainage of middle and lower lobe segment(3). Padded firm adjustable table with different inclinations is available for postural drainage, but for practical purpose the foot end of the cot can be elevated using blocks. The affected area should be identified by clinical examination and chest skiagram prior to CPT. The positions for postural drainage of different bronchopulmonary segments are given in Fig. 1(4) .
Chest percussion Depending on the available area, the therapist can use single or both cupped hands or 3 fingers with the middle finger tented or a facemask with either the port covered or occluded by a finger and strike repeatedly at a rate of 3 per second(5) over that part of the bronchopulmonary segment which needs to be drained. The cupped hand/mask tends to trap a cushion of air, which softens the blow while striking, and the air column inside the cupped hand causes effective dislodgement of the secretions in the underlying bronchus as the compression wave is presumably transmitted to the underlying bronchus and gravitational aid causes flow of secretions from the bronchus towards the glottis. The movement should be only at the wrist without causing pain or discomfort and can be done throughout inspiration and expiration. Rings should be removed before percussion. Percussion should be vigorous but not painful and should not be done on bare skin, but over soft comfortable clothing or towels. Properly done percussion produces only sound rather than discomfort which the child gets used to in due course. Mechanical percussors are also available and maybe useful in adolescents. Vibration In this a rapid vibratory impulse is transmitted through the chest wall from the flattened hands of the therapist by isometric alternate contraction of forearm flexor and extensor muscles, to loosen and dislodge the airway secretions. Vibration is a technical procedure and is usually effectively executed only by a physiotherapist. Thoracic squeezing The expiratory phase is reinforced in this maneuver. The child is asked to take a deep breath and then exhale through the mouth as completely and rapidly as possible, as would be done for a forced expiratory volume determination. The depth of the expiration is increased by brief firm pressure from the operator’s hand compressing the sides of the thorax (thoracic squeeze). This is usually done by physiotherapist. Cough stimulation Child can be requested to cough. In uncooperative or small children tracheal stimulation or tickling can be done by placing index finger or thumb on anterior side of the neck against trachea just above sternal notch with gentle but firm inward pressure in circular pattern as the child begins to exhale(4). In certain diseases with respiratory involvement the child may have feeble or ineffective cough and cough reinforcement is of much help in such conditions. Here the child should be advised to cough out while the hand of the operator reinforces anticipated cough by synchronously compressing the lower half of the chest. The sputum may be collected in a container to quantify or demonstrate to the child and their parents. In small infants and children a bulb sucker can be used to clear the oral and nasal secretions. For home therapy, postural drainage with cupped hand percussion with cough reinforcement and suctioning or clearing the retained nasal and oral secretions is advised. Timing and duration of chest physio-therapy CPT should be done 1-4 times a day, preferably half an hour before meals or one and half hour after meals(6). The total duration should not exceed 30 minutes with 3-6 minutes in each position(5). Prior broncho-dilator inhalation (preferably salbutamol) may effectively clear the lung secretions in children with associated bronchospasm. Breathing exercise or deep breathing or vigorous activity such as skipping and jumping can precede postural drainage in order to loosen the secretions, provided such activity is not contraindicated. The procedure must be taught to the child’s parents. A printed sheet with pictures of various drainage positions explaining the procedures should be made available to the parents. Indications for chest physiotherapy (a) In conditions with copious retention of airway secretions like bronchiectasis, cystic fibrosis (CF), many airway clear-ance modalities other than conventional chest physiotherapy (CPT) like the flutter device, intermittent positive pressure breathing (IPPB) and high-frequency chest wall oscillations (HFCWO) are available(7). In CF physiotherapy tech-niques remove excessive secretions, thereby improving ventilation in the short term. In the long term, reduction of elastase-mediated damage to the airways might slow the progressive damage and impairment of mucociliary clearance(8). In CF, comparing various techniques with conventional CPT showed no difference between them but did show significant sputum expectoration than with no treat-ment(9). As no gold standard exists for physiotherapy in CF it would be appropriate to select a technique from the spectrum available that suits the individual’s requirements(10). (b) With thick mucus secretion leading on to segmental lesions/collapse. Poor secretion clearance affects normal mucus function, disrupting the physical, bio-logical, and chemical components of the pulmonary defense system. Excessive or retained secretions undergo qualitative changes to become thick, sticky and infectious, eventually injuring the healthy lung tissue and deranging O2 / CO2 exchange(11). (c) In children with weak respiratory mechanics like cerebral palsy and neuro-muscular disorders e.g., spinal muscular atrophy. (d) In children with weak cough like vocal cord palsy, brain stem lesion. (e) In kyphoscoliosis the lung function is restricted by decreased chest wall compliance and can result in unequal lung expansion (basal atelectasis on the con-cave side and over expansion of the convex side), leading to ventilation/per-fusion mismatch. These factors together increase the work of breathing and pre-dispose to respiratory failure(12). ( f ) In bedridden children, immobilization may limit or prevent physical exercise, impairing their ability to maintain aerobic capacity and lung volume(13,14). Physical exercise increases mucus elimination by as much as 40% compared to normal breathing and is an important component of normal airway clearance (15). (g) In bronchiolitis no clinically discernible benefit or impact on the course of the illness was found due of chest physio-therapy(16,17). (h) In acute severe asthma CPT does not improve lung function. It may be beneficial to expedite recovery in the presence of atelectasis and retained secretions, particularly in the ventilated asthmatic child. Inappropriate treatment in the presence of bronchoconstriction might greatly exacerbate the situation (17). (i) In pneumonia patients who had CPT had a longer duration of fever especially in the younger patients(8). Thus CPT may be harmful in patients who do not produce excessive sputum(19). Once the consolidatory phase begins to resolve, CPT might have some benefit in mobilizing and clearing secretions, especially in weak and uncooperative child(17). (j) In intensive care unit (ICU), CPT is the treatment of choice only for patients with acute lobar atelectasis. Prone positioning improves oxygenation in some patients with severe acute respiratory failure or ARDS. Positioning in side lying (affected lung uppermost) improves oxygenation in some patients with unilateral lung disease. Significant increases in heart rate, systolic and mean BP, cardiac output, oxygen consumption, carbon dioxide production and PaCO2 can occur during CPT especially in ICU setting. Sedation prior to CPT may decrease or prevent these adverse effects. Preoxygenation, sedation and reassurance are necessary before suctioning to avoid suction-induced hypo-xemia. There is very little or no evidence to suggest that routine physiotherapy in ICU prevents pulmonary complications or is effective in the treatment of pulmonary conditions (with the exception of acute lobar atelectasis) or facilitates weaning, decreases length of stay, and reduces mortality or morbidity. Routine positioning (with the exceptions cited above) is not of much help(20). (k) Prophylactic drainage of contralateral normal lung following the drainage of diseased lung. Contraindications (Table I)
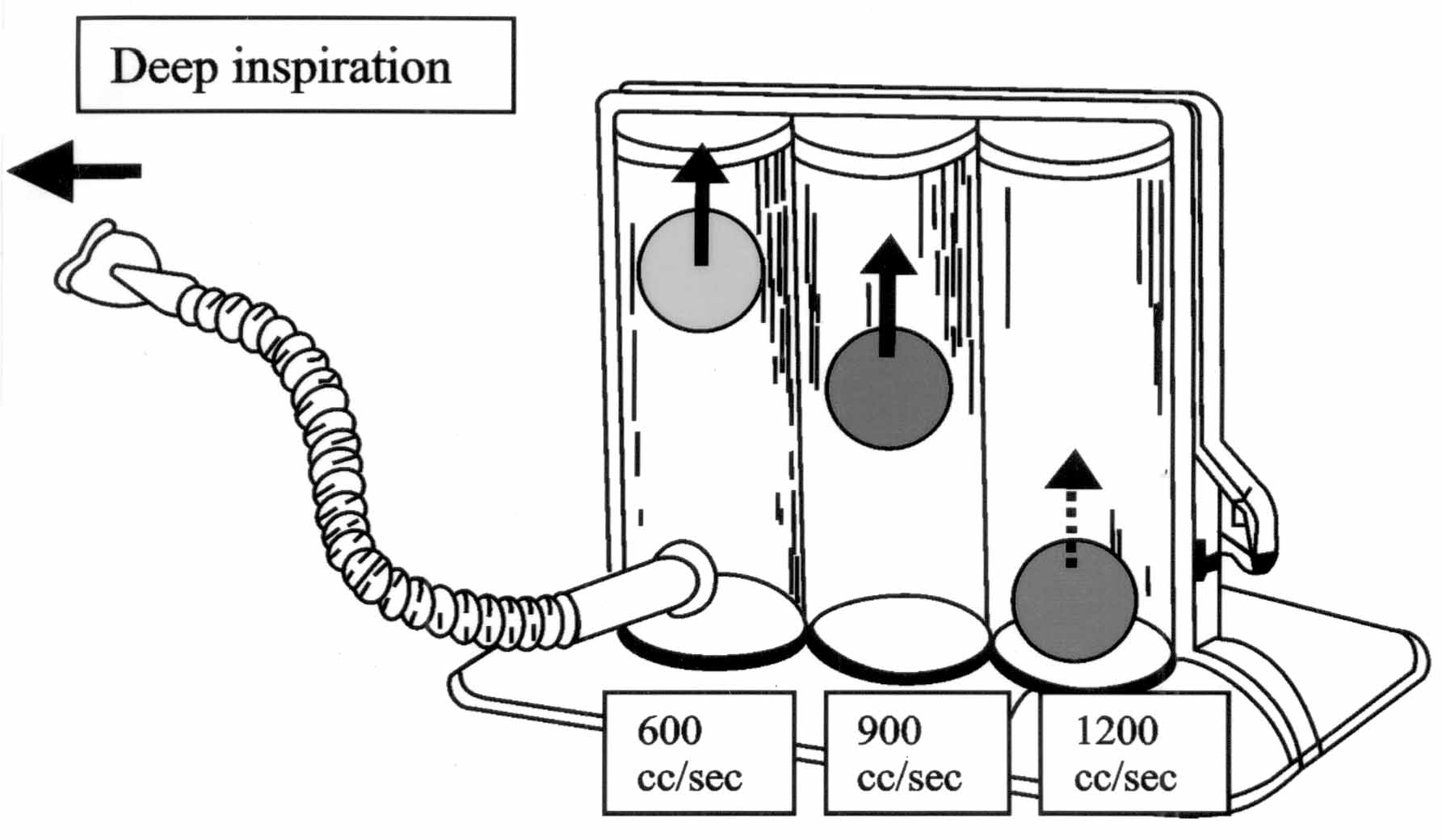
This include situations where proper positioning cannot be safely accomplished or injuries would preclude appropriate percussion/vibratory maneuvers or pre-existing disease processes could be exacerbated during CPT. The decision to use postural drainage therapy requires assessment of potential benefits versus potential risks. CPT should be provided for no longer than necessary to obtain the desired therapeutic results(21,22). Complications during CPT are hypoxemia, increased intracranial pressure, acute hypotension, pulmonary hemorrhage, pain or injury to muscles, ribs, or spine, vomiting, aspiration, bronchospasm and dysrhythmias. Limitations to CPT are in patients with ineffective cough and in critically ill or spastic children where optimal positioning may be difficult(22). Physiotherapy in young infants Physiotherapy for young infants may be done preferably with the baby lying on the physiotherapist or mother’s lap and pillows could be added to achieve the required position. During physiotherapy the baby should be positioned in such a way that the facial colour and breathing can be checked frequently. Toys, musical boxes can be shown to hold the attention of the toddlers while doing CPT to overcome their fear and apprehension(23). Breathing exercises Breathing exercises are meant to increase the breathing efficiency and functional tidal volume. It is a component of airway clearance therapy in CPT and is also used for pulmonary rehabilitation. Breathing exercise increases the diameter of airway above that of normal tidal volume and helps to loosen and dislodge bronchial secretion. This prevents alveolar collapse, facilitates lung expansion and peripheral airway clearance. Indications are (a) Obstructive lung diseases like chronic bronchitis, chronic asthma (not during exacerbation) and chronic obstructive pulmonary disease (COPD); (b) Restrictive lung defects due to kyphoscoliosis, obesity and neuromuscular disorders involv-ing the respiratory muscles; (c) Presence of pulmonary atelectasis during recovery phase of pneumonia and after drainage of pleural effusion/ empyema; and (d) Presence of conditions predisposing to the development of pulmonary atelectasis secondary to brochi-ectasis, cystic fibrosis, thoracic surgery, upper-abdominal surgery and immobilization. This can be initiated when the child is conscious, alert, hemodynamically stable with no evidence of airleak or respiratory distress. Breathing exercises like sustained maximal inspiration (SMI), assisting with tactile sense, exhaling through pursed lips and modified breathing exercises in children are described below. Sustained Maximal Inspiration (SMI) In SMI the patient is encouraged to make a larger than normal inspiratory effort to mimic natural sighing or yawning. In general, normal breathing without sigh results in alveolar collapse within one hour. In SMI the patient is asked to sustain his inspiratory effort for a minimum of 3 seconds, this increases trans-pulmonary pressure, inspiratory volumes, improves inspiratory muscle performance and re-establish or simulate the normal pattern of pulmonary expansion. When the procedure is repeated on a regular basis, airway patency is maintained and lung atelectasis is prevented and reversed(4). This is contraindicated in patients who are unable to deep breathe effectively (e.g., with vital capacity [VC] less than about 10 mL/kg or inspiratory capacity [IC] less than about one-third of predicted)(25). To be effective this should be done almost every hour when the patient is awake and each cycle should last for 30-60 seconds with 4-5 repetetions(3). The total duration should be less than 5 minutes to prevent hypercapnia. Incentive Devices use the principle of SMI and have a positive reinforcement on the patients by helping them to visualize their progress through visual indicator(3). Though several such devices are available, the incentive deep breathing exerciser (Fig. 2) is most suitable for pediatric age group. Evidence suggests that deep breathing alone without mechanical aides can be as beneficial as incentive devices in preventing or reversing pulmonary complications(25). In infants a cry is equated to deep breathing.
Assisting With Tactile Sense Here the therapist’s places his hand over the chest where the muscular movement is desired and the patient is encouraged to concentrate on expanding that part of chest under the placed hand. Exhaling through pursed lips The patient is asked to breath in slowly through the nose for 3 slow counts, then purse the lips as like blowing a whistle and then asked to breathe out gently through pursed lips for 6 slow counts. The air should escape naturally and not be forced out. The inhalation and exhalation ratio should be 1:2. Modified breathing exercises in children Modified breathing exercise is mandatory in children because they might not cooperate like adults. The principle is to attract children and not to create boredom. It can be accompanied by musical tune that would evince interest in a child. Various modified forms of breathing exercises like group exercises, running, balloon blowing, abduction, adduction and forward movement of upper limbs, blowing air into the water with a straw, blowing a trumpet, flute and mouth organ playing are found effective in children(23). Laughing is a good exercise and babies can be tickled to laugh. Conclusion Chest physiotherapy is essential in the airway clearance of acute and chronic respiratory disorders with retained airway secretions. This definitely helps to improve and maintain the well being of the patients within the limitations imposed by the impaired lung function. Regular CPT plays a significant role in reducing the morbidity in children with chronic lung diseases like cystic fibrosis.
| ||||||
|
References | ||||||
|
|
![]()