|
|
Case Reports Indian Pediatrics 2000;37: 662-664 |
|||||||||||||||||||
|
Fetal Brain Disruption Sequence |
|||||||||||||||||||
|
Shubha R. Phadke
Fetal Brain Disruption sequence (FBDS) is characterized by congenital severe micro-cephaly with overlapping cranial sutures, prominent occipital bones, rugosities on scalp and imaging and autopsy evidence of partial brain disruption. Such a phenotype indicates severe damage due to infective or ischemic etiology. We are reporting one such case.
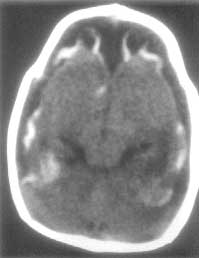
An 8-month-old male child was brought with the chief complaints of abnormal head size and delayed psychomotor development. He had an abnormal shaped head since birth, and could not hold his head or sit without support till this age. He did not respond to sound and had a fixed staring gaze. On examination, he showed severe microcephaly; occipitofrontal circumference was 32 cm (12 SD below normal), There were prominent palpable ridges at the sites of sutures. The skull appeared collapsed (Fig. 1) and he had a convergent squint. The scalp was normal. He had hyperextended lower limbs, hypertonia, hyperreflexia and bilateral extensor plantar reflex (Fig. 2). His fundus examination showed optic atrophy of both eyes. The CT showed severe arrest of brain growth and calcification in the thin cortical mantle. The skull bones were overlapping at sutures (Fig. 3). The mother had history of high grade fever without rashes at 4 months of gestation. However, there was no serological evidence of intrauterine infection in the child.
In this case, the severe microcephaly with sutural overlap, gross neurological impairment and CT scan showing marked brain damage is consistent with the diagnosis of fetal brain disruption sequence. Fetal brain disruption sequence(1) is a phenotype resulting from marked brain destruction during second or an early 3rd trimester causing fall in intracranial pressure and collapse of skull (leading to microcephaly and overlapping sutures). The exact mechanism producing decreased intracranial pressure leading to skull collapse is unknown. The characteristic features especially the overlapping sutures and scalp rugae are obvious during neonatal period and these findings may disappear later, as was the case in this child. The degree of brain damage that gives rise to this phenotype is associated with severe neurological abnormality in the form of spasticity, seizures, blindness and extremely poor cognitive development. The severely affected children die during neonatal period(2) while mildly affected cases may show better prognosis with achievement of some developmental milestones(3). The etiologies could be prenatal infection or vascular insult. The positive serological test for any of the TORCH group of infections during neonatal period or early infancy can give clue to a definite etiology(4). Thromboembolic phenomenon in one of the twins following death of the co-twin is known to give rise to severe brain damage and microcephaly(5). Though the etiologies may vary, the diagnosis of FBDS phenotype is important as it is not associated with increased risk of recurrence in the family, as most of the probable etiologies are environmental and not likely to recurr during the next pregnancy. However, one should be cautious in giving low risk of recurrence as an occasional case of recurrences in a family has been reported(6). This calls for a good ultrasonographic follow up during the next pregnancy.
|
|||||||||||||||||||
![]()