|
Lateral
Cranial Meninfocele |
Man Mohan Harjai
Maneet Gill
Kanwarjit Singh
From the Department of Surgery, Armed Forces Medical College, Pune 411 040, India.
Reprint. requests: Lt. CoI. Man Mohall Harjai, Reader, Department of Surgery, Armed Forces Medical College, Pune 411 040, India.
Manuscript Received: April 7, 1998; Initial review completed:
June
29, 1998;
Revision Accepted: August 13, 1998
Usually cranio-spinal dysraphism has a
posterior mid line defect, the majority being in the lumbosacral region. Laterally placed meningoceles are uncommon. Till date only two cases of lateral frontal encephalocele have been reported(1). We report an unusual case of temporal encephalocele.
Case Report
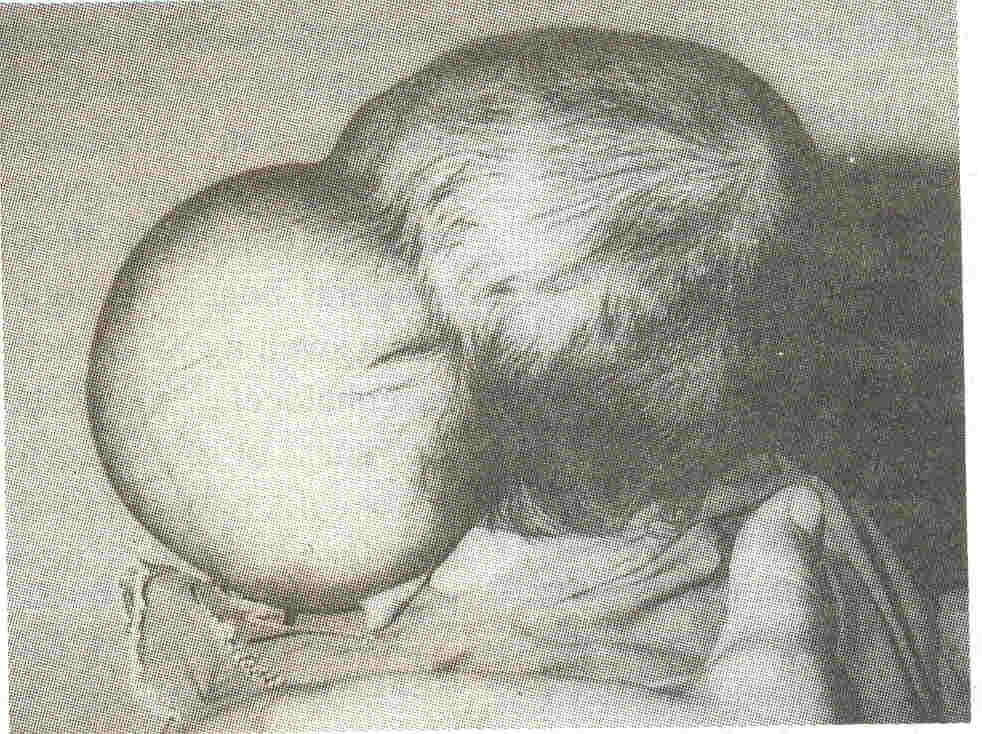
A 2-month-old female infant presented with a gradually increasing swelling over the
left side of the head since birth. The swelling was almost as big as her head. The swelling was 12 x 6 x 4
cm in the region of the left temple extending on to the frontal region anteriorly and the parietal region posteriorly (Fig.1).
It was cystic, fluctuant, transiIIuminant and conducted an impulse on crying. Clinical diagnosis of an encephalocele was made. An ultrasound confirmed the cystic
nature of the swelling. At surgery a large cyst was dissected free from the
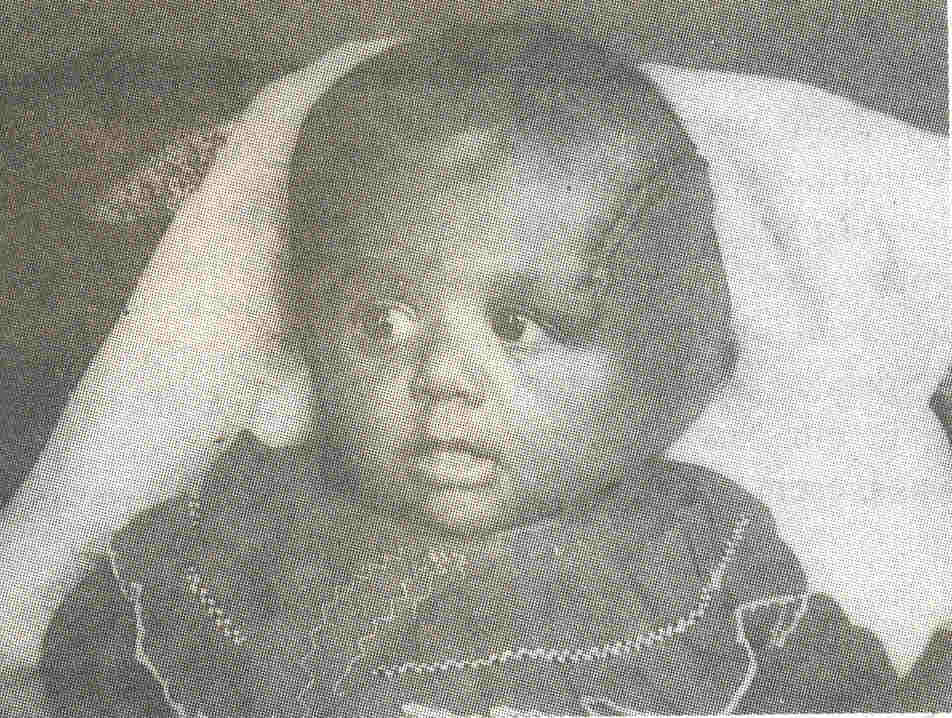
surrounding skin and found to have a' narrow neck protruding through a small defect between the parietal and the temporal bones. There were no neural elements forming the contents of the cyst. The neck was secured and the cyst excised. This was followed by water tight closure of the duramater. Post-operatively the wound healed well (Fig.
2). The fluid from the cyst (taken per-operatively), revealed leukocytes 8/mm3; proteins 470 mgldl; sugar 23 mg/dl and chloride 115 meq/L, very similar to normal CSF. Histopathology revealed a lining of flattened to cuboidal epithelium, with papillationsat a few places. The wall was composed of connective tissue.
 |
|
Fig. 1. Posterior view of giant lateral temporal meningocele. |
 |
|
Fig. 2. Photograph after removal of the lateral meningocele. |
Discussion
The sequence of events in human CNS ontogenesis follows a complex pattern which starts at around the 18th day of gestation with the formation of neural plate and carries on till early post-natal period when neuronal
migration, axosomatic and axo-dendritic synaptic connections take place. Interwoven in this neural sequence is the development of the vertebral column and the skull from the mesoderm. Cranio-spinal dysraphic states can be due to failure of fusion of bone in the region of the vertebral column-spina bifida (occulta, cystica or aperta) or due to improper development of the skull-cranium
bifidum. Skull defects account for less than 10% of all cranio-vertebral anomalies.
Our case is one of cranium bifidum. Such lesions are usually classified as 'Encephaloceles' whether or not they contain neural tissue. In western countries the lesion in cranium bifidum involves the occipital bone in the midline posteriorly in 85% of cases. In Asia, the majority of encephaloceles are an- terior(2) and involve the frontal or nasal bones, but still in the midline. In our case the involvement was lateral, which is very rare. Matson(3) in his series of 1396 cases of spinal dysraphism, found an incidence of 0.3% for lateral meningocoeles, and of these, almost all were lumbosacral. From India, Sharma
et al.(1) have reported a series of 619 cases of spinal dysraphism. They have been able to trace 10 cases of lateral cervical meningocele and only 2 of lateral frontal meningocele in world literature. In
'Lehman
syndrome' multiple lateral meningoceles are associated with presence of wormian bones, malar hypoplasia, downslanted palpebral fissures, high narrow palate and cryptorchidism(4). However, in our case no other associated anomaly was present.
Defective calvarial ossification can result in encephaloceles presenting at atypical sites. An anterior basal encephalocele obstructing
the nares can be mistaken for a nasal polyp and removal attempted. ln our case the calvarial defect was between the parietal and temporal bones. A high index of suspicion that a swelling at the ectopic sites could be a encephalocele must be maintained. An awareness of such a lesion will avoid a sense of bewilderment and proper management will lead to normal. development of the infant.
|
1.
Sharma Y, Mohanty S, Singh DR. Uncommon cranio-spinal dysraphism. Ann Acad Med Singapore 1996; 25: 602-608.
2.
Menkes JH, Till K. Malformations of the central nervous system.. Ill: Textbook of Child Neurology, 5th edn. Ed. Menkes JH. Baltimore: Williams and Wilkins; 1995. p 253.
3.
Matson DD. Neurosurgery of Infancy and Childhood, 2nd edn. Springfield, IL, Charles C Thomas, 1969.
4.
Lehman RA, Stears JC, Wesenberg RL, Nusbaum ED. Familial osteosclerosis with abnormalities of the nervous system and meninges. J Pediatr 1977; 90: 49-54.
|
