|
|
Case Reports Indian Pediatrics 2008;45:154-156 |
||||
|
Pulmonary Alveolar Microlithiasis in Siblings |
||||
|
Rajoo Thapa From the Department of Pediatrics, The Institute of Child Health, Kolkata 700 017, India. Correspondence to: Dr. Rajoo Thapa, The Institute of Child Health, 11, Dr. Biresh Guha Street, Kolkata 700 017, West Bengal, India. E-mail: [email protected]
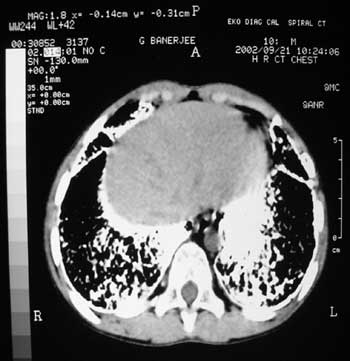
Abstract: Key words: Children, Pulmonary alveolar micro-lithiasis. Introduction Pulmonary alveolar microlithiasis (PAM) is a rare disease of unknown etiology characterized by the widespread intra-alveolar deposition of laminated calcispherites in the lung(1). Most patients are between the ages 30 to 50 years at the time of diagnosis. Disorders of calcium metabolism are typically absent. It is often diagnosed incidentally following a chest radiograph. There are few reports of this disorder in children, since it does not cause any symptoms in its early course but chronically progresses over many years. Case Report Case 1: A nine-year-old boy, born to non-consanguineous parents, presented with complaints of occasional mild upper respiratory tract infections. The child was otherwise healthy. There was no history of contact with tuberculosis. On examination, his weight and height were below the fifth percentile. Systemic examination was normal. Relevant hematological investigations were normal. Chest radiograph showed bilateral micronodular calcified densities (with characteristic sand storm like picture) concentrated mainly over the lower two-thirds of both the lung fields obliterating the cardiac, mediastinal, diaphragmatic borders and the interlobar fissures (Fig. 1). Pulmonary function testing showed moderate restrictive changes with no breathing problems under exercise. HRCT revealed microcalcifications located in the subpleural regions around the perivascular bundles and in the perilobar areas. No microcysts or fibrotic changes were appreciated (Fig. 2). Bone scintigraphy using Tc 99m diphosphonate revealed moderately increased soft tissue radiotracer in both lung fields, which confirmed the calcific nature of the lesions.
Based upon the clinical presentation and the investigations, a diagnosis of pulmonary alveolar microlithiasis was made. Case 2: The family members of the index case were screened by chest radiography. The boy had a younger sister who was four years old. Her height and weight were on the fifth percentile and was otherwise healthy. Her chest radiograph showed the presence of bilateral micronodular calcified densities, which were more discrete and concentrated in the lower two thirds of both lung fields. Fine, interrupted lines of calcification along the cardiac, mediastinal and diaphragmatic borders and along the interlobar fissures were noted. HRCT scan reported micronodular calcifications in the subpleural regions, around the perivascular bundles and in the perilobar areas, patchy and considerably less extensive than in the brother, but comparatively more prominent than the nodules in the parenchyma. Ground glass opacities were reported in the posterior lower zones. No microcysts or fibrotic changes were noted. On bone scintigraphy, mildly increased soft tissue radiotracer uptake was appreciated in both lung fields. The parents and the elder sister had no features suggestive of PAM in the chest radiograph. Discussion PAM is a disease of undefined etiology characterized by the formation of lamellar concretions of calcium phosphate or "microliths" within the alveoli, creating a classic pattern on the chest radiograph. There are lesser number of pediatric case reports of PAM compared to adults. Schmidt, et al.(2) described the occurrence of asymptomatic PAM in two Turkish siblings in whom the diagnoses were confirmed by transbronchial lung biopsy and broncho-alveolar lavage. The parents were consanguineous and they had another sibling who was normal, thereby suggesting an autosomal recessive mode of inheritance. Helbich, et al.(3) reported on a 31 year old woman with PAM. Thirty four members of the family were screened and two more asymptomatic cases were detected, a 13-year old boy and a 6-year old girl. The diagnosis was confirmed in the boy by open lung biopsy. Because of the positive family history and characteristic features of PAM on the chest radiograph and on HRCT, no open lung biopy was required for confirmation of the disease in the girl. Senyigit, et al.(4) reported 6 additional cases of PAM from Turkey. Three cases had been diagnosed earlier, and 3 new cases were detected during the screening of the family members. In their series, all the patients were male and the mean age was 11.5 years ranging between 5 and 29 years. Five of the patients were cousins and the other one was their uncle. The cases were diagnosed by bronchoalveolar lavage in 5 patients and transbronchial biopsy in one. PAM was incidentally discovered in a five year old boy being evaluated for multiple exostoses. Neither disorder was identified in other members of the immediate family(5). Caffrey and Altman(6) described the disorder in premature twins who died at the age of 12 hours and reviewed 66 reported cases. Turktas, et al.(7) described a 10 year old boy who presented with cough of 3 years duration. A 13-year old child with PAM and calcified pericardium is also described(8). Erelel, et al.(9) reported on 2 asymptomatic siblings with PAM, a 7-year old girl and her 13-year-old brother. In the girl, chest X-ray and computed tomography revealed diffuse interstitial changes but no uptake of technetium 99m (99mTc) on bone scan was noted in the lung. The microliths stained pink with Papanicolaou dye in bronchoalveolar lavage (BAL) fluid but not with von Kossa. In the brother, characteristic radiological findings and 99mTc uptake in the lung were detected. The microliths stained pink with Papanicolaou in BAL fluid and black with von Kossa. They hypothesized that the first case was in the early phase of PAM because of lack of 99mTc uptake. The differential diagnoses of PAM would include military tuberculosis, varicella pneumonia, pulmonary fungal infections, pulmonary alveolar hemosiderosis, several pneumoconioses, pulmonary alveolar proteinosis and metastases, specially from thyroid neoplasms. The reported cases reiterate the fact that not all mottled shadows on a chest radiograph represent military tuberculosis, especially if the disease course is indolent. Alternative diagnoses must be considered. The biopsy of the lung tissue may not be necessary in the diagnosis of PAM as shown in the present report. The findings on HRCT coupled with the uptake of Tc99m diphosphonate scan in the lungs may be sufficient for the confirmation of the diagnosis. Thorough screening of the family members of the index case must be performed to detect the disease at the earliest. Contributors: RT: manuscript drafting and review; DG: patient care and follow up; AG: diagnosis, overall coordinator and guide. Competing interest: None. Funding: None stated. | ||||
|
References | ||||
|
|
![]()