|
Severely malnourished
under-five children in India are estimated to
constitute 6.4%, in addition to 19.8% who are
moderately malnourished according to the National
Family Health Survey (NFHS) – 3(1). This translates
to about 8.1 million children with severe acute
malnutrition (SAM) in India. Currently available
facilities for hospitalized care of children in
India would be inadequate even if they were utilized
exclusively for the treatment and rehabilitation of
children with SAM(2). Limitations in availability as
well as access to facility based care, therefore,
make community management of SAM a priority. This
would include screening and anthropometry of
malnourished children, identification of those who
can be managed without hospitalization and their
nutritional rehabilitation and monitoring in their
communities and homes. Small hospitals and
facilities where children hospitalized with SAM are
managed often lack kitchens where recommended diets
to rehabilitate these children can be hygienically
prepared every day. A ready to use therapeutic food
(RUTF) product that can be administered to children
with SAM in their homes or in small community
facilities is, therefore, only one component of
community management of SAM and the capability to
produce RUTF is just one step in that direction.
RUTF Production
The production of RUTF is a
simple process and consists of three basic steps -
grinding, mixing and packaging(3). Typically, the
ingredients used in the production of RUTF are milk
powder, vegetable oil, peanuts, sugar, minerals and
vitamins(3). Shelled groundnuts are roasted in a
roaster at a temperature of approximately 160ºC
for 40-60 minutes. This is followed by grinding them
into smaller particle sizes in a grinder such as a
hammer mill. Skimmed milk powder, the ground
peanuts, vegetable oil, powdered sugar and the
minerals and vitamins are then blended in a
planetary mixer with less than 0.1% emulsifiers and
anti-oxidants. The paste is then homogenized to
further reduce particle size (< 200 µm) and is then
packed. The shelf life of RUTF paste can be extended
to 2 years by nitrogen-flush packaging, which has
been shown to extend shelf lives of milk
products(4). A production line with a rated capacity
of 1.5 tonnes per day that includes a roaster,
planetary mixer and a nitrogen flush packaging
system is estimated to cost about 35-50 lakh rupees.
Nitrogen flush packaging machinery is the most
expensive component of an RUTF production line but
paste that is not packed in airtight packages will
need to be consumed within a few months,
considerably limiting its utility, especially when
storage and transportation is unpredictable.
Nitrogen flush packaging is often the rate limiting
step and will depend on the size of the pouches –
larger pouches will hasten packaging but will be
inappropriate for single day consumption by a single
child. Particle size reduction machines such as
pulverizers, hammer mills and universal grinders,
mechanical mixers such as barrel mixers and
planetary mixers and packaging machines are readily
available for small batch production of 1 tonne per
week and can be customized for higher output.
Lentils and rice have been used
in alternative RUTF recipes but are yet to be well
evaluated(5). Peanut butter is being produced in
some parts of the country for export – peanut butter
can also be directly sourced from such companies and
used to prepare RUTF. This is very likely to
increase cost and may be recommended for situations
where machinery to grind peanuts into the size
required is not available ("Hand made" RUTF).
Quality Control and Quality
Assurance
RUTF must be tested for
aflatoxins – a major issue with peanuts, apart from
testing for microbial contamination, heavy metals,
pesticides, lipid oxidation, moisture content, fat
and protein estimation, water activity and minerals
or vitamins concentrations(6,7). If a mineral and
vitamin premix from a certified supplier is added to
RUTF, the concentration of one single vitamin or
mineral can be estimated to ensure the quality and
homogeneity of the product. This will reduce the
costs associated with quality evaluation, including
those related to the complexity of handling multiple
laboratory instruments and analytical errors in
estimating multiple micronutrient concentrations.
When batch volumes are large, the frequency of
testing also can be reduced bringing down costs
further.
Production Models of RUTF
Self help groups and village
industries: A number of food products that are
current market leaders or favourites are made by
self-help groups or village/ cottage industries
(e.g. Lijjat Papad)(8). A number of such
industries strive for societal good like gender
equality, sustainability and poverty alleviation
while producing very high quality food products(8).
Often such companies are considered to be free of
conflicting commercial interests. The ingredients
will need to be provided in the form of ready to
mix, pre-ground ingredients for "hand mixing" in
homes. This model is unlikely to result in large
quantities of RUTF being produced in single batches.
The cost of quality testing will be far higher since
each small batch will need to be tested.
Dairy cooperatives: Beginning
with the success of the Kaira District Cooperative
Milk Producers’ Union, the dairy cooperative
movement has spread all over the country. Dairy
cooperatives have also since diversified from milk
into a range of food products like chocolates, baked
goods and even oils(9). Amul, the brand of the
Gujarat Cooperative Milk Marketing Federation and
Mother Dairy, of the National Dairy Development
Board, are among the top brands in India(10). Amul’s
sales and distribution network that reaches every
corner of the nation is supported by the largest
cold chain in the world and over 5 lakh retail
outlets(9). Similarly, other cooperatives have
popular brands (Mother Dairy, Vijaya, Aavin, and
Verka) that rely on efficient and reliable
distribution networks within each state. In addition
to the necessary equipment and most (often all)
ingredients being available in house, the
distribution channels of these cooperatives will be
invaluable in making RUTF available across the
country.
Niche food companies:
A number of niche food companies exist all over the
country that have held a major chunk of the market
share for products like spices, traditional snacks,
heat and serve foods and extruded products like
pasta. Some of these companies have been
participating in food fortification programs (Swagat
Foods (P) Limited makes iron fortified rice premix
using Ultra Rice™ technology). Others provide
packaged foods for public health programs and
clinical trials (Christy Friedgram Industry makes
ready to use products for Integrated Child
Development Scheme and double fortified salt for the
mid day meal program in South India). Compact AS, a
Norwegian company that manufactures therapeutic food
products used by aid agencies, has commenced
production of RUTF in India through its subsidiary,
Compact India Pvt Ltd.
Large private food companies are
capable of large-scale production of RUTF. Their
volumes of production may support regional demands
of RUTF. Doubts will be expressed about the business
models of some of these companies. Strong,
enforceable guidelines on marketing of RUTF and
non-therapeutic modified RUTF-like products will be
needed to limit the abuse of RUTF.
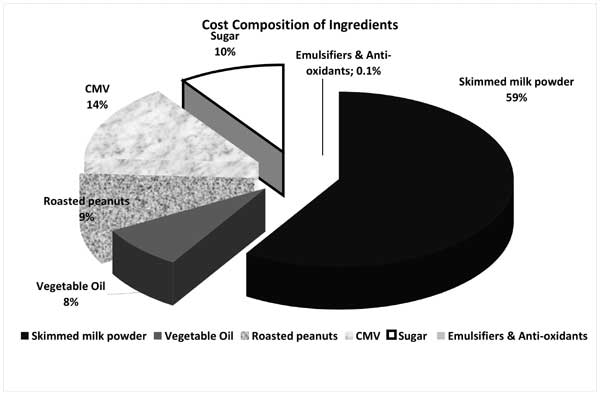
The scale of operations and the
costs of production vary by the production model.
Skimmed milk powder accounts for nearly 60% of the
ingredient costs (Fig 1). Hence milk
cooperatives that produce skimmed milk powder will
be ideally placed to produce cheaper RUTF with lower
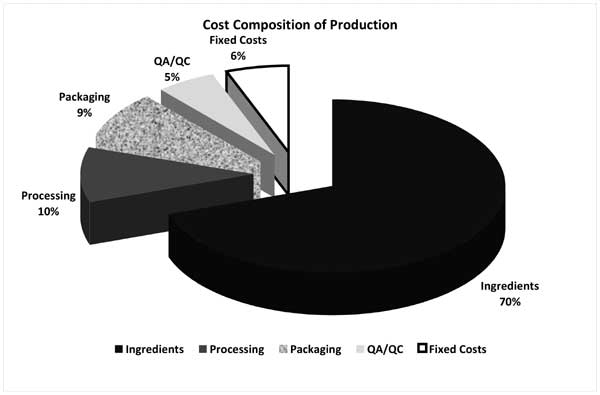
ingredient costs. Fixed costs account for a small
proportion of the overall cost of RUTF production in
models with specialized or customized equipment
capable of producing 15 tonnes of RUTF per day (Fig
2). Fixed costs also account for a small
percentage (<3%) of the cost of RUTF for smaller
companies capable of producing about 1.5 tonnes per
day of RUTF on less specialized equipment. Nearly
80,000 metric tonnes of RUTF will be required to
treat severely malnourished children in India with
300 g of RUTF per day for 30 days.
 |
|
Fig. 1 Cost
composition of ingredients required for RUTF
production. |
 |
|
Fig. 2 Cost
composition of RUTF production at production
volumes of 15 tonnes per day. |
Opportunities for RUTF Production
and Distribution in India
Ingredients required for the
manufacture of RUTF are readily available in India (Table
I). India is the number one producer of milk in
the world and over 1.6 lakh tonnes of milk powder is
produced in India every year. Peanuts are ubiquitous
in Indian diets and India is the largest exporter of
shelled groundnuts in the world. Easy domestic
availability of these ingredients with pre-existing
distribution channels and local vendors keeps costs
of these ingredients low unlike in Africa where the
bulk of ingredients are imported. India is home to a
large domestic food processing industry that deals
in dairy foods, baked goods, heat and serve foods
and spices that already use indigenously
manufactured equipment that are required (or can be
easily adapted) for the production of RUTF. Bharat
Immunologicals and Biologicals Corporation Limited (BIBCOL),
a public sector company that manufactures vaccines
and zinc tablets has developed a composite mineral
and vitamin (CMV) formulation. This CMV, based on
the WHO composition recommended for treatment of
SAM, can be added directly as a premix to F-75,
F-100, RUTF and other therapeutic nutritional
products(13). This product is likely to be available
for acceptability trials by the end of the year (personal
communication). The entire spectrum of
ingredients and equipment required for production of
RUTF is indigenously available – RUTF made in India
will therefore be a sustainable solution with local
production that can vary from small to large-scale
models in the public or private sector.
Table I
Availability of Indigenous Ingredients for RUTF Production in India(11,12)
| Commodity |
World production
rank |
Annual
production
(in metric tonnes) |
Exports
|
| |
|
|
| Milk |
1 |
109 million |
N/A |
| Skimmed milk powder |
6 |
162,201 |
25% of annual
production is exported |
| Groundnuts |
2 |
9 million |
Largest exporter of shelled
groundnuts – 240,000 tonnes |
| Refined sugar |
2nd largest producer |
26.3 million |
3rd largest exporter at
2,261,228 metric of sugarcane tonnes |
Challenges to RUTF Production and
Distribution in India
Severe acute malnutrition is
almost always an illness that stems from the lack of
sufficient food – few children get malnourished when
sufficient quality food is available. The
availability or the capability to produce RUTF does
not address prevention of SAM or directly improve
food security in these households. Irrespective of
how reasonably indigenously produced RUTF is priced,
it will remain beyond the purchasing power of most
households where severe malnutrition occurs. For
these children, RUTF will have to be provided by
governments (local or central) or be channeled
through non-profit and aid agencies. Therefore, the
treatment of SAM, a condition arising from food
insecurity, through commercial processed food is
seen as a paradoxical, conflicting situation. It can
be argued that some resources will be directed to
procure RUTF that could possibly be used to improve
access to food for these vulnerable sections of
society through enhancements in employment,
agricultural production, food rations or subsidized
food. While this maybe true in part, the treatment
of millions of severely malnourished children, many
out of whom die everyday is as pressing a need as
the prevention of further malnutrition through
improved access to food. These therefore, must not
be viewed as competing activities, much like the
treatment of any other illness (e.g. Tuberculosis,
HIV etc.) while concerted efforts are made towards
preventing it.
Varied interpretations of the
Supreme Court ruling on hot cooked meals have also
led to confusion. The Supreme Court had ruled that
hot cooked meals must be provided for children
through the Integrated Child Development Scheme (ICDS)
(14). This cannot be directly interpreted to
preclude the use of food based therapeutic
interventions for children who suffer from illnesses
or the use of RUTF for children with SAM.
Uncertainty about the support for community
management of SAM based on RUTF will deter food
companies from investing or venturing into RUTF
production.
The Way Forward
Voices from various sections of
society will need to be heard before a viable
community management program can be effectively
instituted for the management of SAM. The meeting
organized on "Nutrition Therapy in SAM" at the All
India Institute of Medical Sciences in November 2009
was a major step in this direction. A number of
concerns raised against the use of RUTF are not
characteristics of the product itself but seem to be
directed against international or multinational
agencies and corporations. While every voice of
concern cannot be assuaged, considerable choice must
be offered in production models and scales to fit
the needs and views of market segments. Multiple
producers and suppliers must be supported to prevent
monopolization of the RUTF market. The Government
and aid agencies (local and global) will remain the
largest procurers of RUTF for children with SAM. In
the absence of clearly stated governmental positions
on the use of RUTF, few companies will be willing to
produce RUTF for use in India. The fact that Compact
India Pvt Ltd has established a production facility
for RUTF and other nutritional products for SAM at
Manesar, Haryana makes it unambiguously certain that
RUTF can be produced in India on a large scale.
Most children with SAM cannot be
accommodated in hospitals; many families cannot
afford their earning members to stay with their
children in hospitals for many weeks. Treatment in
the homes of severely malnourished children provides
a feasible solution in such scenarios. Efficacy
trials will compare standard hospital care for SAM
with community management; far removed from real
life situations of limited care. Can we refuse to
provide an alternative when we are unable to provide
standard hospitalized care to millions of children
with severe acute malnutrition?
Acknowledgments
We acknowledge all vendors,
suppliers and manufacturers who provided inputs for
projections in this article. We also thank Mr Mukesh
Juyal for helping with the manuscript preparation.
Contributors: KNB conceived,
designed and conducted the analyses and interviews
and prepared the manuscript. UCMN also designed the
analyses and revised the manuscript for important
intellectual content. All authors approved the final
manuscript.
Disclaimer: All projections
are based on data and costs obtained from vendors
and food manufacturers in India. Since no data is
available from companies that are actually already
manufacturing RUTF, these are only estimates.
Funding: None.
Competing interests: None
stated.
References
1. International Institute for
Population Sciences (IIPS) and Macro International.
2007. National Family Health Survey (NFHS-3),
2005–06: India: Volume I: 273.
2. Gupta P, Shah D, Sachdev HPS,
Kapil U. National workshop on "Development of
guidelines for effective home based care and
treatment of children suffering from severe acute
malnutrition". Indian Pediatr 2006; 43: 131-139.
3. Manary MJ. Local production
and provision of ready-to-use therapeutic food (RUTF)
spread for the treatment of severe childhood
malnutrition. Food Nutr Bull 2006; 27: S83-89
4. Lloyd MA, Hess SJ, Drake MA.
Effect of nitrogen flushing and storage temperature
on flavor and shelf-life of whole milk powder. J
Dairy Sci 2009; 92: 2409-2422.
5. Bahwere P, Sadler K, Collins
S. Acceptability and effectiveness of chickpea
sesame-based ready-to-use therapeutic food in
malnourished HIV-positive adults. Patient Prefer
Adherence 2009; 3: 67-75.
6. Peraica M, Radiæ B, Luciæ A,
Pavloviæ M. Toxic effects of mycotoxins in humans.
Bull World Health Organ 1999; 77: 754-766.
7. Okoth SA, Ohingo M. Dietary
aflatoxin exposure and impaired growth in young
children from Kisumu District, Kenya: Cross
sectional study. Afr J Health Sci 2004; 11: 43-54.
8. Ramanathan M. Women and
Empowerment: Shri Mahila Griha Udyog Lijjat Papad.
Economic and Political Weekly 2004; 39: 1689-1697.
9. Welcome to Amul - The Taste of
India. Available at: http://www.amul.com/products.html.
Accessed June 3, 2010.
10. Synovate news. Available at:
http://www.synovate.com/news/article/extra/20070824/Asia%27s%20Top%201000%20brands%20
fact %20sheet.pdf. Accessed June 3, 2010.
11. FAOSTAT, Food and
Agricultural Organization of the United Nations.
Available at: faostat.fao.org. Accessed May 2, 2010.
12. Hand Book of Sugar
Statistics, Indian Sugar Mills Association, Ministry
of Consumer Affairs, Department of Food & Public
Distribution, Govt. of India; 2009.
13. Management of Severe
Malnutrition: A Manual for Physicians and Other
Senior Health Workers. Geneva: World Health
Organization; 1999.
14. Deshpande M, Dasgupta R, Baru
R, Mohanty A. The case for cooked meals concerns
regarding the proposed policy shifts in the mid-day
meal and ICDS programs. Indian Pediatr 2008; 45:
445-449.
|


