|
|
Letters to the Editor Indian Pediatrics 2004; 41:867-868 |
||
|
Ellis-Van Crevald syndrome |
||
|
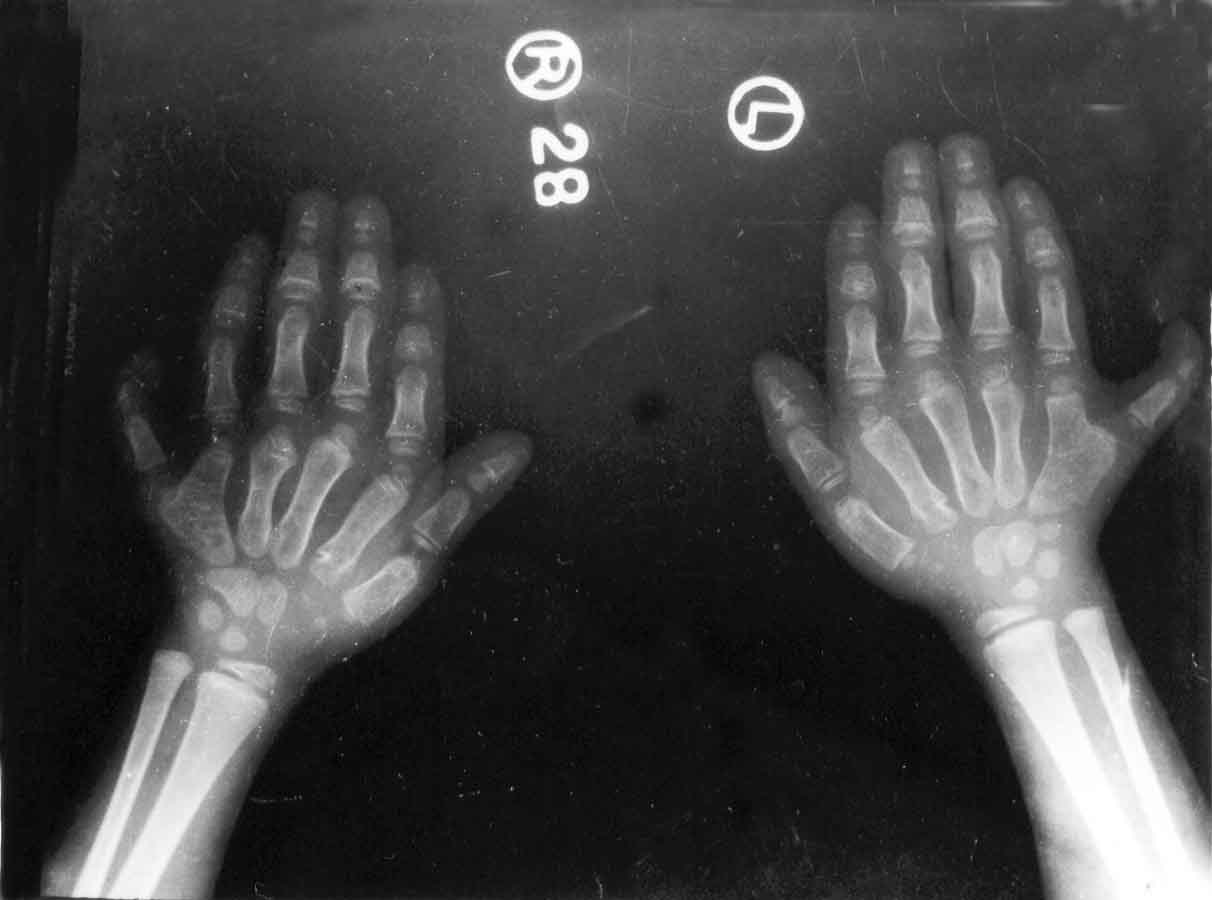
The Ellis-Van Crevald dysplasia is a short limbed dwarfism, characterized by ectodermal dysplasia, polydactyly (postaxial) and congenital heart disease (atrial septal defect or a single atrium). The condition is inherited as an autosomal recessive trait and is evident at birth. Here we present a case of Ellis-Van Crevald syndrome. A six year old child with symmetric polydactyly of both hands and genu valgum deformity was referred for radiographic assessment. On physical examination, there were six digits in both hands with dysplastic finger nails. The upper and lower extremies were shortened out of proportions to the trunk with genu valgum deformity. Radiograph of hands revealed bifid 5th metacarpals and complete duplication of the little fingers bilaterally with short distal and middle phalanges as compared to proximal ones (Fig. 1). Both knees showed hypoplasia and irregularity of lateral portion of upper tibial epiphyses with dome shaped metaphysis leading to valgus deformity. Chest radiograph revealed enlarged cardiac shadow, which on further assessment with 2D echocardiography revealed an atrial septal defect of ostium secondum type. The case was diagnosed as Ellis-Van Crevald syndrome.
Ellis Van Crevald (EVC) syndrome is a skeletal dysplasia with an incidence of approximately l out of 1,50,000 live births. A high prevalence has been reported among certain world populations like Amish and Arabs of Gaza strip. The disorder was first described by Ellis and Van Crevald in 1940. The inheritance is an autosomal recessive manner, that means a child with EVC is borne to average sized parents both carrying gene for EVC. The parents have 25% chances with each pregnancy of having child with EVC, if both are carrier of the gene. Clinical features include postaxial polydactyly of hands which is seen in all patients. Polydactyly may be just extra soft tissue not adherent to the skeleton and devoid of bone, cartilage, joint or tendon, or the digit may show duplication with components like bifid metacarpal or there may be a complete digit formation with its own metacarpal and complete soft tissue. Patient may also have polydactyly in feet. There is short limbed disproportionate dwarfism with extremities shortened out of proportion to trunk. Ectodermal manifestations include absent or hypoplastic fingernails or toenails, dysplastic teeth or teeth present at birth (natal teeth) and sparse hair. Fusion between upper lip and gum may be seen. In addition renal abnormalities and hydrocephalus have been noted in some patients. Congenital heart defects occur in about 50% of patients. The most common heart defects are atrial septal defects. Other less common defects are ventricular septal defects, hypoplasia of the aorta and a single atrium(1). Radiological features include postaxial polysyndactyly, short ribs, short iliac wing, horizontal acetabulum with medial and lateral spurs (trident pelvis), premature ossification of femoral capital epiphyses. Proximal tibial epiphysis is hypoplastic laterally with dome shaped metaphysis; in addition medial tibial diaphyseal exostosis, genu valgum and fibular shortening may be seen at knee. Carpal development is delayed and carpal fusions are seen especially between capitate and hamate. In addition to this some patients may also demonstrate polycarpyly with ninth carpal bone appearing in distal row(2). The form of EVC syndrome presenting in neonatal period has skeletal changes similar to those of asphyxiating thoracic dystrophy(3). However, they represent different conditions, and Jequier(4) has suggested that the two can be differentiated as follows: (a) polydactyly in asphyxiating thoracic dystrophy involves the lateral side of the hand, whereas in EVC it usually involves the medial side; (b) congenital heart disease is almost always present in EVC but is not a particularly common feature of asphyxiating thoracic dystrophy; (c) consanguinity is more common in EVC; and (d) the thoracic cage deformity is usually not as pronounced in EVC. Death in childhood is common owing to cardiac and pulmonary complications, and if they survive morbidity is high. Future testing for gene mutations may provide valuable information for premarital counseling and prenatal diagnosis. Prenatal ultrasound is an accurate means of identifying skeletal dysplasia. Faisal Haque, Department of Radiodiagnosis, J. N. Medical College, A.M.U., Aligarh, India.
| ||
|
References | ||
|
|
![]()