|
|
|
Indian Pediatr 2016;53:
345-346 |
 |
Synovial Sarcoma in a Neonate
|
|
Venkatraman Radhakrishnan, Anjana Joel, *Shirley
Sundersingh and #Anand
Raja
From Departments of Medical Oncology, *Pathology and
#Surgical Oncology, Cancer Institute, Adyar, Chennai, India.
Correspondence to: Dr Venkatraman Radhakrishnan, Associate
Professor, Department of Medical Oncology, Cancer Institute (WIA), Adyar,
Chennai 600 020, India.
Email: [email protected]
Received: July 28, 2015;
Initial review: September 29, 2015;
Accepted: December 28, 2015.
|
|
Background: Malignant tumors in neonates are rare. Case
characteristics: A tumor was detected in the left biceps of a 3-day
old neonate. Tumor biopsy and molecular study confirmed the diagnosis of
synovial sarcoma. The child received multi-modality treatment
with surgery and chemotherapy. Outcome: The child is disease-free
on follow-up period of 12 months. Message: Synovial sarcoma can
rarely occur in a neonate.
Keyword: Chemotherapy, Malignancy, Neonate,
Tumor.
|
|
M
alignancies in the neonatal age group are rare,
and are usually congenital in origin [1]. Neuroblastoma and teratomas
are the most common cancers seen in neonates. We present a neonate with
synovial sarcoma who was successfully managed with multimodal treatment
including chemotherapy and surgery.
Case Report
A 21-day-old girl was brought to our hospital by her
parents with complaints of swelling in her left arm. The child was born
to non-consanguineous parents. She was a full-term normal vaginal
delivery, and weighed 3 kg at birth. The mother had an uncomplicated
pregnancy and her antenatal ultrasound studies were normal. The child
received BCG vaccine in her left arm on the second day of life. The
parents noticed a swelling in her left arm below the BCG vaccination
site, 2 days after the vaccine was administered. The child was seen by a
general surgeon, who suspected the swelling to be BCG vaccine-related
abscess in the left biceps muscle, and attempted surgical drainage of
the swelling. However, no pus was drained and the swelling could only be
removed piecemeal. The histopathological examination (HPE) of the tissue
was consistent with sarcoma. The swelling increased in size after the
surgical exploration and the parents reported to our hospital for
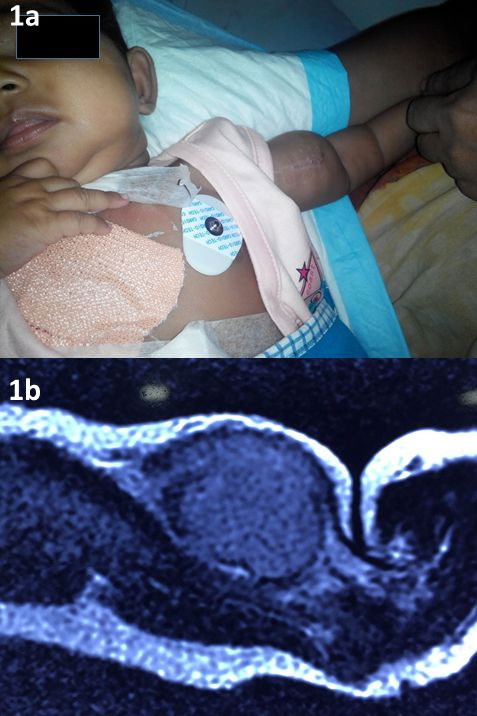
further management. On evaluation, a hard non-tender mass (5×3 cm) was
palpable in the left biceps muscle (Fig. 1a). The mass was
mobile in the direction perpendicular to the axis of the muscle fibres.
There were no dysmorphic features, and no other significant findings
were noticed on examination. Magnetic Resonance Imaging (MRI) of the
left arm showed a well-defined mass (3.4×3.1×2.4 cm) in left biceps
muscle. The mass was iso-intense on T1 and hyperintense on T2 (Fig.
1b). The computed tomographic (CT) imaging of chest and ultrasound
imaging of abdomen and pelvis did not show any evidence of metastatic
disease. Histopathological examination of patient’s formalin-fixed
operated specimen at our hospital confirmed the diagnosis of synovial
sarcoma (Web Fig. 1). Immunohistochemistry
(IHC) showed that the tumor cells were positive for EMA, CD68, SMA,
CD99, Vimentin, CD34 and CD56, and were negative for Keratin, Myogenin
and Desmin. Polymerase Chain Reaction (PCR) of tumor specimen was
positive for SYT-SSX4 translocation, which confirmed the
diagnosis of synovial sarcoma. The child received six cycles of
chemotherapy with Ifosfamide 900 mg/m 2/day
for three days and adriamycin 15 mg/m2/day
for two days given once in every three weeks. Three cycles of
chemotherapy were given before surgical resection of the tumor, and
three cycles were given after the resection. There was a decrease in
size of the mass by 50% after the first 3 cycles of chemotherapy.
Complete wide local excision of the tumor bearing biceps brachii muscle
and adjoining soft tissue was done by a team of surgical oncologist and
plastic surgeon. The histopathological examination of the grey white
area of the specimen revealed only fibrosis, chronic inflammatory cells
and foreign body giant cells with no residual tumor suggesting a
complete pathological response to chemotherapy. Microscopic examination
all the margins, adventitia and perineurium were free of tumor. The
patient was not given radiotherapy to the local site in view of her age,
anticipated significant long-term toxicity, and complete pathological
response to chemotherapy. The patient is currently on follow-up for last
12 months and is disease-free. Her growth and development are normal.
 |
|
Fig. 1 (a) soft tissue swelling in the left
biceps muscles; (b): MRI showing mass in left biceps muscle.
|
Discussion
Neonatal malignant tumors are extremely rare and
histologically heterogeneous. They are challenging and difficult to
treat when compared to older children. Chemotherapy and radiotherapy are
associated with increased short-term and long-term toxicities in
neonates because of the immaturity of liver, lungs, brain and kidneys.
Soft tissue neoplasms in neonates are commonly benign and vascular in
origin [2]. Rhabdomyosarcoma is the most common malignant soft tissue
tumor in neonates. Synovial sarcoma in a neonate is exceedingly rare. In
an earlier report [3], the diagnosis of synovial sarcoma in the neonate
having mass in left arm was made on histopathological examination alone,
and was not confirmed by molecular studies. The gold standard for
diagnosing synovial sarcoma currently is the demonstration of t(x,18)
translocation by PCR [4]. The t(x,18) translocation involves the
translocation of SYT gene on chromosome 18 and either SSX-1, SSX-2 or
SSX-4 gene on X chromosome. The SYT-SSX4 translocation seen
in our patient is rarer than the commonly seen SYT-SSX1 or
SYT-SSX-2 translocation [5]. This case is being presented for its
rarity and successful management and also to alert the pediatrician that
not all swellings in the neonatal period are benign. Early diagnosis and
effective treatment is vital for improving outcomes in neonates with
malignant tumors.
Contributors: VR, AJ: clinical management
and drafting of report; SS: pathological examination and drafting of the
report; AR: surgical management and drafting of the report.
Funding: None; Competing interests: None
stated.
References
1. Orbach D, Sarnacki S, Brisse HJ, Gauthier-Villars
M, Jarreau PH, Tsatsaris V, et al. Neonatal cancer. Lancet Oncol. 2013;14:e609-20.
2. Ferrari A, Orbach D, Sultan I, Casanova M, Bisogno
G. Neonatal Soft tissue sarcomas. Semin Fetal Neonatal
Med. 2012;17:231-8.
3. Köse D, Annagür A, Erol C, Uðraþ S, Köksal Y.
Synovial sarcoma in a premature newborn. Pediatr Int. 2014;56:e17-20.
4. Skytting B, Nilsson G, Brodin B, Xie Y, Lundeberg
J, Uhlén M, et al. A novel fusion gene, SYT-SSX4, in synovial
sarcoma. J Natl Cancer Inst. 1999;91:974-5.
5. Kerouanton A, Jimenez I, Cellier C, Laurence V,
Helfre S, Pannier S, et al. Synovial sarcoma in children and
adolescents. J Pediatr Hematol Oncol. 2014;36:257-62.
|
|
|
 |
|
